Calcified Lesions A Pichard L Satler Ron Waksman




























")





. • Enzymatic")
- Slides: 38
Calcified Lesions A Pichard, L Satler, Ron Waksman, I Ben-Dor, W Suddath, N Bernardo, M Gaglia, M Lipinsky. Medstar Heart and Vascular Institute Medstar Washington Hospital Center Washington, DC
A. Pichard, MD I have no relevant financial relationships for this lecture.
Calcification • Angiography often misses severe calcification • Severe calcification has major consequences for immediate and longterm results of PCI
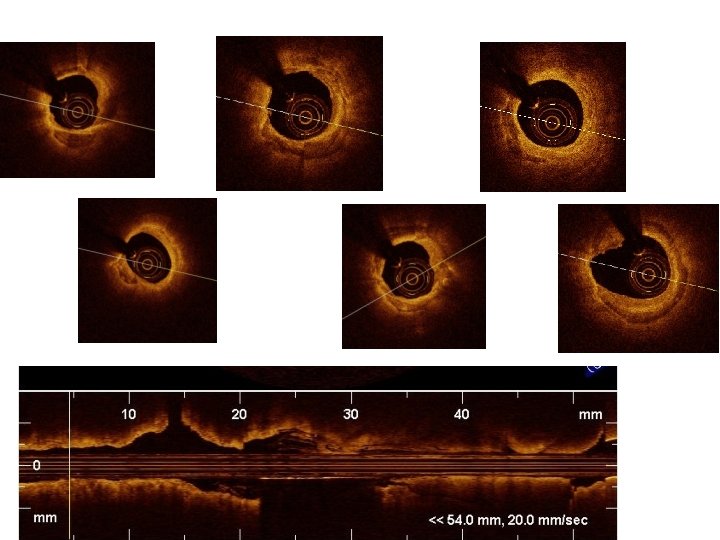
Calcium by IVUS and OCT Mintz, JACC Imaging 2015; 8: 461 -71
Calcification by Angio and IVUS n=1155 lesions Calcification detected: - 73% by IVUS - 38% by QCA
Restenosis of Calcified Vessels. Mosseri, Satler, Pichard, Waksman. CV Rad Medic 2005; 6: 147 -153 662 calcified lesions had IVUS guided stenting (BMS) and > 6 months f/u 0 -270° Arc of calcium (18% Rotational. Atherectomy) 271 -360° Arc of calcium (65% had Rotational Atherectomy)
Tools to Address Calcification • • • Semicompliant balloon: NO High Pressure NC Ballon: OK sometimes Cutting balloon: OK for “thin calcium” Scoring balloon: OK for “thin calclium” Excimer Laser: does not ablate Ca. May modify compliance. • Rotational Atherectomy: very effective • Orbital Atherectomy: very effective
Imaging is most important to address calcification effectively
Unsuspected severe LAD Calcification
After Rotablator and stent
Calcified LAD
After Orbital Atherectomy
After DES
ORBIT II Registry Single arm study of >400 patients with severe coronary calcification. 30 day results: 98% efficacy for stent delivery 99% <50% residual stenosis 1 year results: Death rate 2. 8% TLR 4. 5%
Instent Restenosis • Direct stenting? • Pretreat with balloon, Cutting Balloon, Laser?
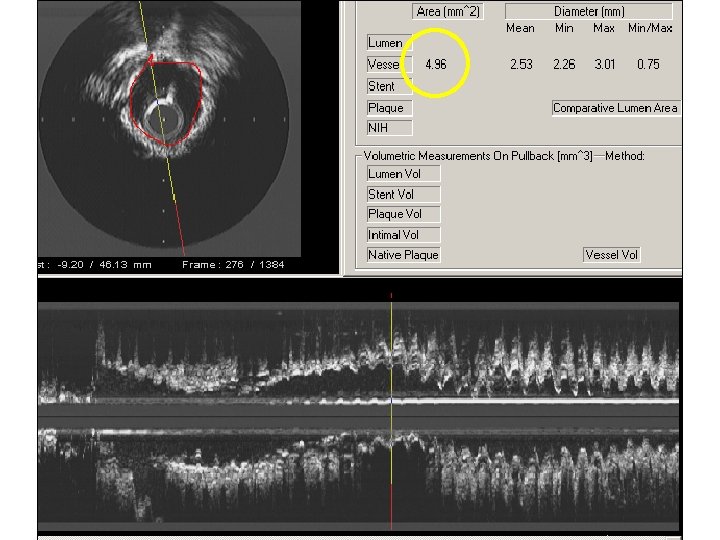
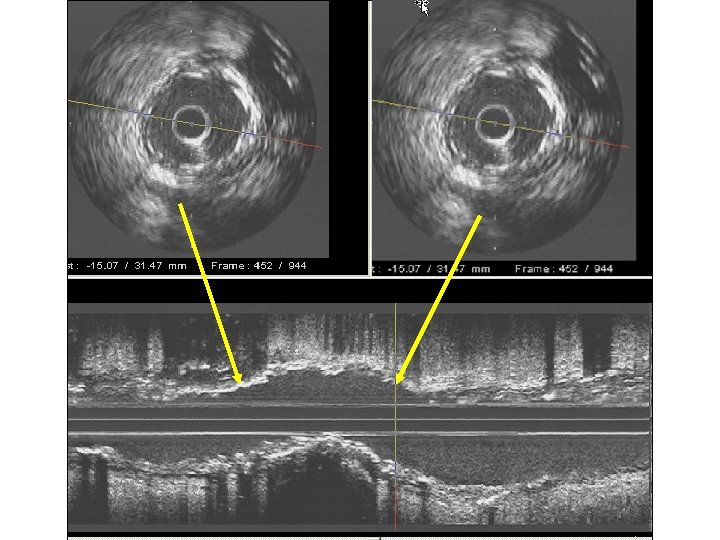
IVUS: Unexpanded Stent due to Concentric Calcification
A fully expanded balloon on angiography does not insure that the lesion/stent is fully expanded
Unexpanded Stent 3. 0 balloon at 28 atm
A Fully Expanded Balloon does not insure the Lesion has Expanded 3. 0 mm Quantum at 28 atm
IVUS after Quantum at 28 atm.
CX disease. IVUS: severe concentric calcification
1. 75 mm Burr
SES Stent 2. 75 x 23 mm at 20 atmospheres
Unexpanded Stent
Balloon at 24 atmospheres
Strategy for Ostial Disease
Strategy for Ostial Disease Direct Stenting A 5 m m Roto-Stent B
Calcified CX IVUS did not cross. 2. 5 Q balloon did not cross
IVUS after Rotational Atherectomy (7 min ablation)
Well expanded Stent after Roto, NC balloon and High Pressure deployment
Simple RCA lesion, no calcium on fluoro.
Concentric calcification with broken arcs: No need for Rotablator
Stent at 12 atm. Stent at 20 atm.
Conclusions • Severe calcification needs to be identified prior to stenting. • Appropriate lesion preparation indispensable in calcified lesions, both for immediate and long term outcomes. • Operators need to be familiar with dedicated tools to prepare calcified lesions. • IC Imaging indispensable for optimal PCI of calcified lesions.
Future ? • Prevention of coronary calcification (new insights into hormonal/metabolic pathways). • Enzymatic softening of existing calcification (Strauss et al. ). • Lithoplasty (Shockwave technology).