Classification of dental caries Dr Maji Jose 1

 • Smooth")









 caries")
 • Linear enamel caries is an atypical form of caries")





 • Characterized by sudden, rapid and almost uncontrollable destruction of")
 • Also called as nursing caries, baby bottle")


 • Is the rampant caries that develop patients undergone radiation")






")







: Deep structural defect. Caries has penetrated up")




: • Lesions involving cuspal tips and incisal edges of teeth.")
 World Health Organization (WHO) system • In this classification the shape and depth")
G. J. Mount classification • � Site")



 • A primary caries is one in which the lesion constitutes")
 • This type of caries is observed around the edges and")
- Slides: 51
Classification of dental caries Dr Maji Jose
1. Classification based on Anatomical Site • Occlusal (Pit and Fissure caries) • Smooth surface caries (Proximal and cervical caries) • Root caries
Pit and Fissure caries • Occurs on occlusal surface of molars& premolars, buccal & lingual aspects of molars, Lingual aspects of maxillary incisors • Highest prevalent site for caries as bacteria rapidly colonize the pits and fissures • Early caries lesions may be detected as brown or black discolouration of pits & fissures in which probe ‘sticks’ • Caries expand as it penetrates in to the enamel. • As caries progresses enamel becomes opaque/brownish white • Surface may appear intact, even when caries involve dentin extensively.
• Sealing of pits and fissures just after tooth eruption may be the most important event in their resistance to caries. • Shape, morphological variation and depth of pit and fissures contributes to their high susceptibility to caries.
Smooth surface caries • Less favourable site for plaque attachment, usually attaches on the smooth surface that are near the gingiva or are under proximal contact. • Smooth surface caries occur on proximal surface just below contact point or gingival third of buccal and lingual surface • Begin as chalky white opacity of enamel- no loss of continuity of enamel surface & not detectable by probing /in radiograph • White spot may become pigmented yellow /brown and may extend buccally /lingually in to embrassure • Enamel become bluish white, surface becomes roughened before frank cavitation occurs
• Lesion have a broad area of origin and a conical, or pointed extension towards DEJ. • V shape with apex directed towards DEJ. • After caries penetrate the DEJ softening of dentin spread rapidly and pulpally
• Cervical caries extend occlusally on buccal/lingual surface • Appear similar to proximal caries • But almost always produce wide open cavity
Root caries • “senile caries” seen in older patients whose periodontal disease has produced exposure of cementum to the oral environment. • The proximal root surface, particularly near the cervical line, often is unaffected by the action of hygiene procedures, such as flossing, because it may have concave anatomic surface contours (fluting) and occasional roughness at the termination of the enamel.
Root surface caries • These conditions, when coupled with exposure to the oral environment (as a result of gingival recession), favour the formation of mature, caries-producing plaque and proximal root-surface caries. • Actinomycetes viscosus/ odontolyticus/ naeslundi in old thick gingival plaques cause initiation of root caries.
Caries originating on the root is alarming because 1. It has a comparatively rapid progression 2. It is often asymptomatic 3. It is closer to the pulp 4, it is more difficult to restore
• The root surface readily allows plaque formation in the absence of good oral hygiene. • The cementum covering the root surface is extremely thin and provides little resistance to caries attack. • Root caries progresses laterally rather than deeply. • Root caries lesions have less well-defined margins, tend to be U-shaped in cross sections • Progress more rapidly because of the lack of protection from and enamel covering.
Root ( Senile) caries
Linear enamel caries (odontoclasia) • Linear enamel caries is an atypical form of caries observed in primary teeth • Seen to occur in labial surface of maxillary anterior teeth in the region of the neonatal line • The line, which represents a metabolic defect such as hypocalcemia or trauma of birth, may predispose to caries, leading to gross destruction of the labial surface of the teeth. • Morphological aspects of this type of caries are atypical and results in gross destruction of the labial surfaces incisor teeth
2. Classification based on rate of Progression • Acute caries • Chronic caries • Arrested caries
Acute caries · Acute caries is a rapid process involving a large number of teeth. · These lesions are lighter colored than the other types, being light brown or grey, and their caseous consistency makes the excavation difficult. · Pulp exposures and sensitivity are often observed ·It has been suggested that saliva does not easily penetrate the small opening to the carious lesion, so there are little opportunity for buffering or neutralization
Chronic caries • These lesions are usually of long-standing involvement, affect a fewer number of teeth, and are smaller than acute caries. • Pain is not a common feature because of protection afforded to the pulp by secondary dentin • The decalcified dentin is dark brown and leathery. • Pulp prognosis is better in that the deepest of lesions usually requires only prophylactic capping and protective bases. • The lesions range in depth and include those that have just penetrated the enamel.
Acute and Chronic Caries • Acute Caries • Fast • Kids and teens • Pale tan colour • Soft demineralized dentin • Painful • Large lesions • Chronic caries • Slowly progressing • Middle aged and older adults • Stained brown or black • Tacky or hard surface • Painless • Small lesions
Rampant caries
Rampant caries - (S/N) • Characterized by sudden, rapid and almost uncontrollable destruction of teeth, affecting surfaces of teeth which are caries free. • This involves proximal and cervical areas of lower anteriors also • Caries involvement of 10 or more teeth over a period of about a year is characteristic of rampant caries • Involves both primary and permanent teeth • Dietary, microbeal and physiological & genetic factors are significant in dev. of rampant caries
Nursing bottle caries -- ( S/N) • Also called as nursing caries, baby bottle syndrome, bottle mouth syndrome etc. • It is a type of rampant caries involving primary teeth • Caused due to 1. prolonged use of nursing bottle containing milk or milk formula, fruit juice etc. 2. Prolonged breast feeding 3. Use of sweetened pacifiers
Nursing bottle caries
• Present clinically as wide spread carious destruction of deciduous teeth mainly upper anteriors followed by first molars and cuspids. Severe involvement leaves only root stumps. • In contrast to rampant caries , in nursing bottle caries, lower anteriors are not involved because these teeth are covered and protected by tongue
Radiation caries - (S/N) • Is the rampant caries that develop patients undergone radiation therapy in head & neck region • This occur due to decreased salivary secretion and alteration in p. H that occur after radiation • Radiation may cause alteration in crystaline structure of enamel
Three patterns are seen…. 1. Caries like lesion encircling the teeth leading to the amputation of teeth 2. Second type appear as a brown of black discolouration. The occlusal and incisal aspect wears away 3. This type begin as a spot depression and spread to all surfaces leading to destruction of enamel shell and part of dentin leaving irregular discoloured stumps
Arrested caries
Arrested caries • Caries that has become static or stationary or do not progress further • Both deciduous and permanent affected • With the shift in the oral conditions, even advanced lesions may become arrested. • This occur due to break down of enamel which eposes the large open cavity without the possibility of further food impaction.
Arrested caries • Soft dentin from this exposed cavity is burnished off leaving hard brownish, polished dentin which is described as eburnation of dentin • Sclerosis of dentinal tubules and secondary dentin formation commonly occur • Exclusively seen in caries of occlusal surface with large open cavity in which there is lack of food retention • Also on the proximal surfaces of tooth in cases in which the adjacent approximating tooth has been extracted
3. Classification based on number of tooth surfaces involved • Simple- caries involving only one tooth surface • Compound- caries involving two surfaces of tooth • Complex- caries that involves more than two surfaces of a tooth
4. Classification based on Chronology • Early childhood caries • Adolescent caries • Adult caries • It has been stated that over a lifetime, caries incidence i. e. the number of new lesions occurring in a year, shows three peaks-at the ages 4 -8, 11 -19 and 55 -65 years
Early childhood caries two variants: Nursing caries and rampant caries. Teenage caries (adolescent caries) • This type of caries is a variant of rampant caries where the teeth generally considered immune to decay are involved. • The caries is also described to be of a rapidly burrowing type, with a small enamel opening. • The presence of a large pulp chamber causing early pulp involvement Adult caries • Root caries and cervical caries are more commonly found in this group.
5. Classification based on extent of the caries • Incipient caries • Occult caries • Cavitation
Incipient caries • The early caries lesion, best seen on the smooth surface of teeth, is visible as a ‘white spot’. • Histologically the lesion has an apparently intact surface layer overlying subsurface demineralization. • Significantly may such lesion can undergo remineralization and thus the lesion per se is not an indication for restorative treatment
• These white spot lesion may be confused initially with Enamel hypoplasia, which can be differentiated by – position away from the gingival margin – shape – symmetry [they usually affect the contra lateral tooth]. • Also on wetting the caries lesion disappear while the developmental defect persist
Occult carious lesions • are usually seen with low caries rate which is suggestive of increase fluoride exposure. • It is believed that increased fluoride exposure encourages remineralization and slow down progress of the caries in the pit and fissure enamel while the cavitations continues in dentine, and the lesions become masked by a relatively intact enamel surface. • These hidden lesions are called as fluoride bombs or fluoride syndrome.
Cavitation • Once it reaches the dentinoenamel junction, the caries process has the potential to spread to the pulp along the dentinal tubules and also spread in lateral direction. • Thus some amount of sensitivity may be associated with this type of lesion. • This may be generally accompanied by cavitation
6. Classification based on Tissue involvement • • • Initial caries Superficial caries Moderate caries Deep complicated caries
• 1. Initial caries: Demineralization without structural defect. This stage can be reversed by fluoridation and enhanced oral hygiene • 2. Superficial caries (Caries superficialis): Enamel caries, wedge-shaped structural defect. Caries has affected the enamel layer, but has not yet penetrated the dentin. • 3. Moderate caries (Caries media): Dentin caries. Extensive structural defect. Caries has penetrated up to the dentin and spreads two-dimensionally beneath the enamel defect where the dentin offers little resistance.
• 4. Deep caries (Caries profunda): Deep structural defect. Caries has penetrated up to the dentin layers of the tooth close to the pulp. • 5. Deep complicated caries (Caries profunda complicata) : Caries has led to the opening of the pulp cavity (pulpa aperta or open pulp).
7. Classification based on pathway of caries spread • Forward caries • Backward caries “Forward-backward” classification is considered as graphical representation of the pathway of dental caries.
8. Dental Caries-Black’s classification Class 1 lesions: • Lesions that begin in the structural defects of teeth such as pits, fissures and defective grooves. Locations include • Occlusal surface of molars and premolars. • Occlusal two thirds of buccal and lingual surfaces of molars and premolars. • Lingual surfaces of anterior tooth.
Class 2 lesions: • They are found on the proximal surfaces of the bicuspids and molars. Class 3 lesions: • Lesions found on the proximal surfaces of anterior teeth that do not involve or necessitate the removal of the incisal angle.
Class 4 lesions: • Lesions found on the proximal surfaces of anterior teeth that involve the incisal angle. Class 5 lesions: • Lesions that are found at the gingival third of the facial and lingual surfaces of anterior and posterior teeth.
Class 6 (Simon’s modification): • Lesions involving cuspal tips and incisal edges of teeth.
9) World Health Organization (WHO) system • In this classification the shape and depth of the caries lesion scored on a four point scale – D 1: clinically detectable enamel lesions with intact surfaces – D 2: clinically detectable cavities limited to enamel – D 3: clinically detectable cavities in dentine – D 4: lesions extending into the pulp
10. Classification by Mount and Hume (1998)G. J. Mount classification • � Site 1: pits, fissures • � Site 2: proximal surfaces • � Site 3: the cervical one third of the tooth
• Size 0: the earliest lesion that can be identified as the initial stages of demineralization • Size 1: minimal surface cavitation with involvement of dentine just beyond treatment by remineralization alone. • Size 2: moderate involvement of dentine. The remaining tooth is sufficiently strong to support the restoration,
• Size 3: the lesion is enlarged beyond moderate. Remaining tooth structure is weakened to the extent that cusps or incisal edges are split, or are likely to fail if left exposed to occlusal load • Size 4: extensive caries or bulk loss of tooth structure e. g. loss of a complete cusp or incisal edge, has already occurred.
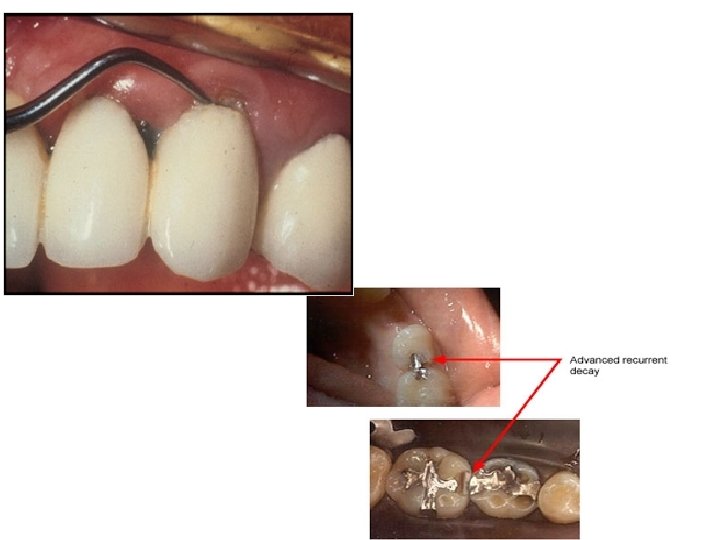
11. Dental Caries-Classification based on Virginity of the lesion • Initial/Primary • Recurrent/Secondary
Primary caries (initial) • A primary caries is one in which the lesion constitutes the initial attack on the tooth surface. • The designation of primary is based on the initial location of the lesion on the surface rather than the extent of damage.
Secondary caries (recurrent) • This type of caries is observed around the edges and under restorations. • The common locations of secondary caries are the rough or overhanging margin and fracture place in all locations of the mouth. • It may be result of poor adaptation of a restoration, which allows for a marginal leakage, or it may be due to inadequate extension of the restoration. • In addition caries may remain if there has not been complete excavation of the original lesion, which later may appear as a residual or recurrent caries