NearInfrared Spectroscopy LipidRich Plaque Study Update Ron Waksman
 Georgetown")


















- Slides: 21
Near-Infrared Spectroscopy: Lipid-Rich Plaque Study Update Ron Waksman, MD Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education, Med. Star Heart & Vascular Institute, Washington DC
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship • Grant/Research Support • Infraredx (for this study) • Consulting Fees/Honoraria Company • • • Boston Scientific Biotronik Biosensors Astra Zeneca Medtronic Vascular Abbott Vascular Symetis Med Alliance Life. Tech Amgen
Combination NIRS-IVUS Instrument TVC Imaging System™ • Laser • Computer with algorithms • Pull-back and rotation device TVC Insight™ Catheter • • Single use, 3. 2 Fr Dual modality Spectroscopy – lipid core plaque IVUS – plaque structure 3
NIRS 64 year old presents with STEMI in March 2012 Unstable angina October 2012 max. LCBI 4 mm 694 Madder R et al. Eur Heart J Img; 2016, doi: 10, 1093/ehjci/jev 340
Cardiac Arrest in 5 K Race associated with LAD Stenosis and a Circular Lipid Core Plaque Ventricular Fibrillation Courtesy Dr. Madder et al, JIC, In press. R
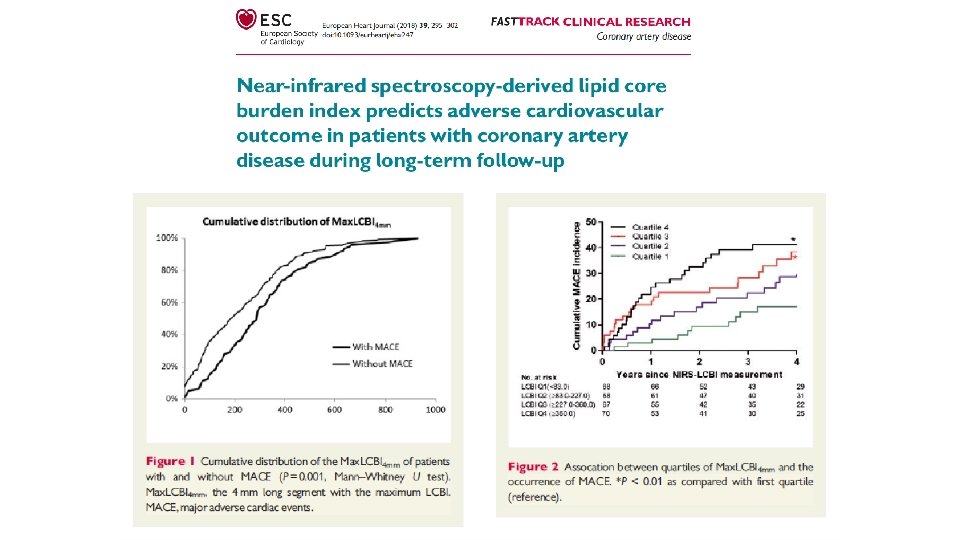
Clinical Validation – NIRS Predicts MACE Near-infrared spectroscopy predicts cardiovascular outcome in patients with coronary artery disease Oemrawsingh RM, Cheng JM, García-García HM, et al CONCLUSION: CAD patients with an LCBI equal to or above the median of 43. 0, as assessed by NIRS in a nonculprit coronary artery, had a 4 -fold risk of adverse cardiovascular events during 1 -year follow-up. Near-infrared spectroscopy-derived lipid core burden J Am Coll Cardiol. 2014 Dec 16; 64(23): 2510 -8. doi: index predicts adverse cardiovascular outcome in 10. 1016/j. jacc. 2014. 07. 998 patients with coronary artery disease during long-term follow-up Schuurman A-S, Vroegindewey M, Kardys I, et al. Large lipid-rich coronary plaques detected by nearinfrared spectroscopy at non-stented sites in the target artery identify patients likely to experience future major adverse cardiovascular events Madder RD, Husaini M, Davis AT, et al. CONCLUSION: Detection of large LRP by NIRS at non-stented sites in a target artery was associated with an increased risk of future MACCE. Long-term follow-up after near-infrared spectroscopy coronary imaging: Insights from the lipid c. ORe plaque association with CLinical events (ORACLE-NIRS) registry Danek BA, Karatasakis A, Karacsonyi J, et al. Eur Heart J Cardiovasc Imaging. 2016 Apr; 17(4): 393 -9. doi: 10. 1093/ehjci/jev 340. Epub 2016 Jan 22. CONCLUSION: NIRS-derived LCBI is associated with adverse cardiac outcome in CAD patients during long-term follow-up independent of clinical risk factors and plaque burden. CONCLUSION: During long-term follow-up of patients who underwent NIRS imaging, high LCBI in a non-PCI target vessel was associated with increased incidence of MACE. Cardiovasc Revascularization Med Mol Interv 2017; 18(3): 177– 81.
Identification of Vulnerable Patients by Intra-coronary NIRS • • 121 Patients Post PCI with single vessel chemogram. max. LCBI 4 mm ≥ 500 at a non-stented site in 9. 9% of patients. MACCE in 58. 3% of patients with a max. LCBI 4 mm ≥ 500 compared to only 6. 4% of those with a max. LCBI 4 mm <500 (p<0. 001; relative risk=9. 1). Madder et al, 2014 max. LCBI 4 mm ≥ 500
Relationship between Lipid Rich Plaque detected by NIRS and Outcomes • Non-target segment in culprit vessel in 121 patients, >1 year follow-up • MACCE: composite of all-cause mortality, non-fatal ACS, acute cerebrovascular events • 5 all-cause mortality, 8 non-fatal ACS, 1 CV event (total 14 events) MACCE in 2 years Hazard ratios for various threshold 24. 2 max. LCBI 4 mm (8. 1 -72. 1) 25 20 Max. LCBI 4 mm≥ 400 15 10. 2 (3. 4 -30. 6) 10 Max. LCBI 4 mm<400 5 2. 4 (0. 7 -8. 6) 2. 4 (0. 7 -7. 2) ≥ 100 ≥ 200 4. 6 (1. 6 -13. 8) 0 ≥ 300 ≥ 400 % of pts 74 (61%) 53 (44%) 36 (30%) 21 (17%) Madder R et al. Eur Heart J Img; 2016, doi: 10, 1093/ehjci/jev 340 ≥ 500 9 (7%)
LCBI in Non-culprit Artery Identifies: Vulnerable Patients • Prospective Single Center Study, 206 patients (ACS 47%) • Primary Endpoint: Composite of all-cause mortality, non-fatal ACS, stroke and unplanned PCI, >40 mm non culprit segment of NIRS LCBI in Non-culprit Artery Above the Median LCBI = 43 Rohit M. Oemrawsingh, MD, ET AL. JACC VOL. 6 4 , NO. 2 3 , 2014
THE LIPID - RICH PLAQUE STUDY Prospective Identification and Treatment of the Vulnerable Patient & the Vulnerable Plaque 9, 000 PCI patients imaging 2+ vessels 3, 000 patients max. LCBI 4 mm >250 100% follow-up • • • Cardiac death Cardiac arrest MI, ACS Revascularization Re-hospitalization for progressive angina 1562 patients 2 year follow-up 6, 000 patients max. LCBI 4 mm≤ 250 50% follow-up
Active Sites and Research Staff • • • • • Washington Hospital Center: Dr. Waksman, J. Lancaster Crittenton Hospital: Dr. Kazziha, M. Cribbs St. John Hospital, Detroit: Dr. Lalonde, T. Jacobson Charleston Area Medical Center: Dr. Lewis, J. Hogan Columbia University Medical Center: Dr. Ali, L. Jaquez Central Baptist Hospital: Dr. Skinner, J. Chapman St. John’s Hospital, Springfield: Dr. Goswami, S. Smith, J. Davis Emory University Hospital: Dr. Samady, E. Rasoul-Arzrumly Methodist Hospital: Dr. Artis, K. Armstrong Medical University of South Carolina: Dr. Powers, L. Carson Community Heart and Vascular Hospital: Dr. Dube, J. Greene-Nashold St. Luke’s Hospital: Dr. Walton, G. De. Freitas Davis Medical Center: Dr. Kim, E. Mansell Mc. Laren Macomb Hospital: Dr. Zainea, T. Gardner-Mosley Palm Beach Gardens Medical Center: Dr. Villa, E. Wettermann University of Minnesota Medical Center: Dr. Raveendran, E. Caldwell Amsterdam Medical Center: Dr. Wykrzykowska, R. Kraak Mc. Laren Bay Region: Dr. Lee, C. Quart Alexian Brothers Heart & Vascular Institute: Dr. Pop, E. Enger Northshore-LIJ Health System: Dr. Singh, P. Chu, G. Chan, M. Hyland • • • • • • Florida Hospital Orlando: Dr. Arias, K. Mink Latvian Centre of Cardiology: Dr. Erglis, S. Jegere University of California Los Angeles Medical Center : Dr. Tobis, L. Douangvila ACRC Cardiology/JFK Medical Center: Dr. Lovitz, J. Mitten Hillcrest Oklahoma Heart Institute: Dr. Leimbach, J. Durham Palmetto General Hospital: Dr. Diaz, R. Perez Delray Medical Center: Dr. Carida, P. Bech Emory Midtown: Dr. Liberman, T. Sanders Royal Brompton Hospital: Dr. Di Mario, D. Dempster New York Presbyterian Hospital – Cornell: Dr. Wong, H. Piscitell University of Texas Galveston: Dr. Fujise, S. Ronald Radboud University Medical Centre: Dr. ten Cate, I. Vereussel SUSCCH, Slovakia: Dr. Hudec, Zeleznikova Maasstad Ziekenhuis: Dr. van der Ent, C. van Vliet Erasmus Medical Center: Dr. Regar, E. Huijskens University of Edinburgh: Dr. Newby, L. Flint Metrohealth Hospital: Dr. Hodgson, J. Nichols Memorial West: Dr. Tami, M. Abdurrahman Heart Hospital Plano: Dr. Potluri, J. Mc. Cracken Golden Jubilee National Hospital: Dr. Mc. Entegart, E. Boyd San Giovanni Hospital: Dr. Prati, Dr. Imola Continued
LRP Study Endpoints • For the Test of the Vulnerable Patient Hypothesis • The primary endpoint for the test of the vulnerable patient hypothesis will be the increased incidence of NC-MACE within 24 months in patients with increased max 4 mm LCBI in all scanned arteries as opposed to those without increased max 4 mm LCBI • For the Test of the Vulnerable Plaque Hypothesis • The primary endpoint for the test of the vulnerable plaque hypothesis will be the increased incidence of NC-MACE within 24 months in coronary artery segments with increased max 4 mm LCBI as opposed to those without increased max 4 mm LCBI
Endpoint Assessment Flow Follow Up Patients N ~ 1563 Reported Patient-Level Event Cleveland Clinic will identify, if imaging is available, follow up event location Send to Cleveland Clinic Adjudication Team Adjudicated Patient-Level Non. Event Adjudicated Patient-Level Endpoint Event The provided follow up event location guides and drives MCRN Plaque Adjudication Team Send to MCRN Plaque Adjudication Team Adjudicated Plaque-Level Non. Event Reported by the site via EDC Adjudicated Plaque-Level Endpoint Event Collaborative Effort: Feedback Between Both Teams at Each Step
Methodology for the Vulnerable Plaque Endpoint Ware Segment containing Endpoint Event Culprit Lesion • Developed a standardized method of determining location of plaques using Ware Segments and Subsegments • Utilizing systematic, blinded adjudication process guided by Cleveland Clinic Cau se nd of I ex re u d ce Pro Suspected Vulnerable plaque in nonculprit artery scanned at index Cause of Follow Up Endpoint Event
Ware Segments: A Standardized Method of Plaque Adjudication • • The MCRN Plaque Adjudication Team confirms the culprit lesion provided by Cleveland Clinic and translates the culprit vessel into standardized Ware Segments and Subsegments Ware Segments – – • 30 mm each; 120 mm total Proximal, Mid, Distal, and Distal Ware Subsegments – – 10 mm; 3 per segment Ex: prox 1, prox 2, prox 3 Prox 1 1 Prox 2 2 Prox 3 3 1 2 3 1 Proximal Mid Distal 2 3
LRP Cumulative Enrollment 1600 1400 1200 1000 800 Enrolled Complete Mar 2016 • Ending 2 year follow up window April 2018 • Stay tuned for these trial results in this calendar year!!! 1281 2 yr Follow Up Group 600 400 200 0 Apr-14 Jul-14 Oct-14 Jan-15 1563 Apr-15 Jul-15 Oct-15 Jan-16
Progress of Follow-up
LRP Events Distribution
Planned to report Study Results in the fall of 2018 Stay Tuned