Xray Peculiar aortic arch arlllckkkh Peculiar aortic arch



 • Positioning • Neurophysiological facilitation of")
")
 NO! -")
19– 25")

 forward enough (the physio on the left")












……")
…… Some studies have stated that 60 cm. H 2")
…… But many clinicians say that 40 cm. H 2")
…… NO SAFE PRESSURE identified in the literature")





 …abdomen…. (to ensure patient not")
 …abdomen…. (to ensure patient not")

















")
 • Ventilator hyperinflation • Manual PEEP: don’t let bag empty")










 • Positioning • Neurophysiological facilitation")
- Slides: 64
X-ray
Peculiar aortic arch? arlllckkkh
Peculiar aortic arch? . . . Tumour arlllckkkh
PT to increase lung volume • (Pain management) • Positioning • Neurophysiological facilitation of respiration • Deep breathing • Manual hyperinflation
Position the patient. (is this how you would position the patient? )
Position the patient. (is this how you would position the patient? ) NO! - no chance of inflating the lower lobes
Or this? Cardiopulm Phys Ther J, 23(1)19– 25
Or this? NO Patient is still not forward enough to expand the lower lobes (and the physio isn’t watching the patient – best to ask the nurse to watch the monitors)
Or this? - yes, patient is (just) forward enough (the physio on the left is palpating for expansion, not doing manual techniques)
Heat-moisture exchanger – Y/N?
Heat-moisture exchanger – Yes
Squeeze bag slow or fast? blog. nialbarker. com
S. . L. . O. . W: a less turbulance → basal → peripheral blog. nialbarker. com
FIRST FEW BREATHS – TIDAL VOLUME q or DEEP BREATH q
FIRST FEW BREATHS – TIDAL VOLUME or DEEP BREATH x
TO JUDGE VOLUME. . . .
TO JUDGE VOLUME. . . . observe.
TO JUDGE PRESSURE. . .
Manometer
Manometer
Ambu bag manometer
Maximum safe pressure (normal lungs)……
Maximum safe pressure (normal lungs)…… Some studies have stated that 60 cm. H 2 O is OK
Maximum safe pressure (normal lungs)…… But many clinicians say that 40 cm. H 2 O is best
Maximum safe pressure (damaged lungs)…… NO SAFE PRESSURE identified in the literature
END-INSPIRATORY HOLD – only if the cardiovascular system is stable Longer positive pressure in the chest impedes cardiac output
HOW MODIFY TECHNIQUE IF EMPHASIS IS ON LOSS OF VOLUME?
HOW MODIFY TECHNIQUE IF EMPHASIS IS ON LOSS OF VOLUME? Emphasise slow inspiration and plateau
HOW MODIFY TECHNIQUE IF EMPHASIS IS ON SPUTUM RETENTION?
HOW MODIFY TECHNIQUE IF EMPHASIS IS ON SPUTUM RETENTION? Sharp let-go
THROUGHOUT, OBSERVE: …patient’s face……(to ensure patient is not distressed) …abdomen…. (to ensure patient not resisting the breath) …monitors…. (to ensure no adverse objective effects) …expansion…. (to ensure technique is effective)
THROUGHOUT, OBSERVE: …patient’s face……(to ensure patient is not distressed) …abdomen…. (to ensure patient not resisting the breath) …monitors…. (to ensure no adverse objective effects) …expansion…. (to ensure technique is effective) If secretions mobilised, stop MH, suction.
AFTER – CHECK: • •
AFTER – CHECK: • Breath sounds / added sounds
AFTER – CHECK: • Breath sounds / added sounds • breathing pattern • monitors • pt comfort
Complications
Complications VENOUS RETURN CARDIAC OUTPUT
Without hyperinflation With hyperinflation
But: Effect of MHI and suction on mean arterial pressure
Complications VENOUS RETURN CARDIAC OUTPUT BP sometimes BP sometimes
Distress Modify by technique and communication
Barotrauma - pneumomediastinum, surgical emphysema or pneumothorax
Barotrauma - pneumomediastinum, surgical emphysema or pneumothorax
Barotrauma - pneumomediastinum, surgical emphysema or pneumothorax
pneumomediastinum, surgical emphysema , pneumothorax Kamha 2008
pneumomediastinum, surgical emphysema, pneumothorax. Air under right hemi-diaphragm and bilateral chest drains
Modifications for: • • UNSTABLE CVS HIGH PEEP COPD ACUTE ASTHMA ACUTE HEAD INJURY FLAIL CHEST GUILLAIN-BARRÉ SYNDROME
• Unstable CVS End-inspiratory-hold? I: E ratio?
• Unstable CVS End-inspiratory-hold? - no I: E ratio? low + extra spontaneous breaths
• High PEEP (> 5)
High PEEP (> 5) • Ventilator hyperinflation • Manual PEEP: don’t let bag empty • PEEP valve
ACUTE ASTHMA ↓ NO
Normal Emphysema No
• Acute asthma
• ACUTE BRAIN INJURY
Flail chest
COPD - Type II c/o inspired gas + preferably no MHI because probably some emphysema
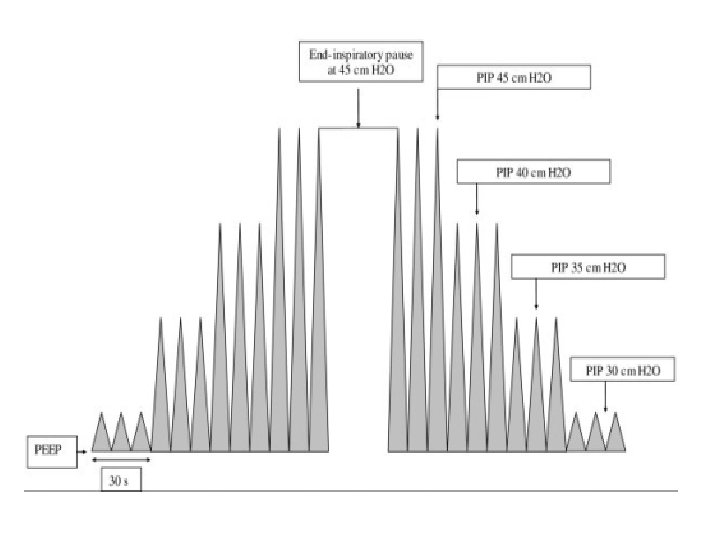
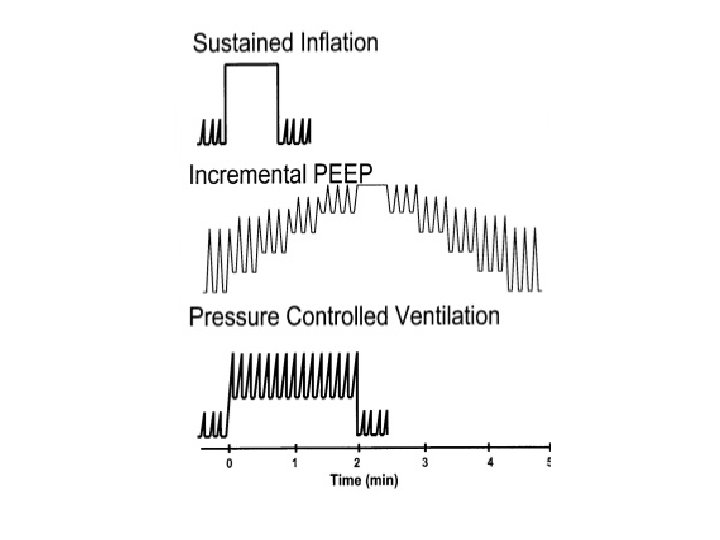
Ventilator hyperinflation VC - tidal volume gradually by 200 ml increments till PIP reaches 40 cm. H 2 O → cont. for 6 breaths → 30 secs rest → repeat → compliance and sputum cleared. Berney & Denehy 2002 PC - step-wise increase in PEEP up to 15 cm. H 2 O and VT up to 18 ml. kg-1 till PIP reaches 40 cm. H 2 O → maintained for 10 cycles → improved oxygenation immediately after CABG, with stabilisation of newly-recruited alveoli by PEEP. Claxton et al 2003 Pressure and/or time of the positive pressure breath increased, e. g. peak pressure of 45 cm. H 2 O and PEEP of 35 cm. H 2 O for one minute followed by PEEP of 10 cm. H 2 O Halter 2003 PEEP increased to 30 -40 cm. H 20 for 30 -40 seconds, after which a sufficient amount of PEEP is applied to keep the lungs open Benefit not sustained without on-going high PEEP Hess 2002
Ventilator hyperinflation or recruitment manoeuvre
Before recruitment – at Fi 02 of 70%: p. H: 7. 47, Pa. CO 2: 31, Pa. O 2: 59, Sa. O 2 91 After recruitment – at Fi 02 of 60%: p. H: 7. 45, Pa. CO 2: 34, Pa. O 2: 182, Sa. O 2 99. 5 www. anaesthetist. com/icu/organs/lung/r
Good relationships required
PT to increase lung volume SUMMARY • (Pain management) • Positioning • Neurophysiological facilitation of respiration • Deep breathing • Manual hyperinflation