Thrombocytopenia in pregnancy Dr hassanali Vahedian ardakani Medicaloncologist

Thrombocytopenia in pregnancy Dr. hassanali Vahedian ardakani Medicaloncologist Hemaotologist

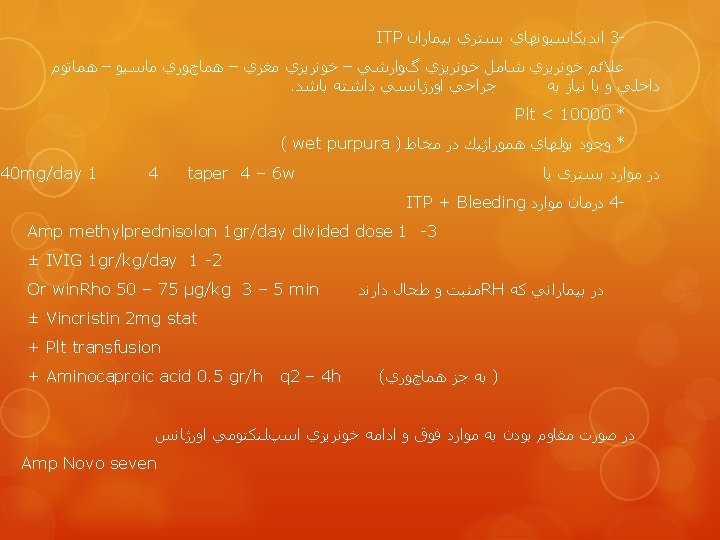
The only goal of treatment is to prevent serious bleeding. A normal platelet count is not a goal of treatment for ITP


Thrombocytopenia in pregnancy Asymptomatic thrombocytopenia is observed near term in about 5 percent of normal pregnancies, and thrombocytopenia, sometimes severe, develops in about 15 percent of women with preeclampsia

Major causes of thrombocytopenia during pregnancy Spurious, due to EDTA-induced platelet aggregation Gestational thrombocytopenia Preeclampsia-eclampsia, including HELLP syndrome Autoimmune thrombocytopenia (idiopathic or related to drugs, systemic lupus erythematosus, antiphospholipid antibodies, or HIV) Disseminated intravascular coagulation Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome or, rarely, congenital TTP Congenital platelet disorders Bone marrow disease Hypersplenism
")
Thrombocytopenia discovered incidentally during a normal pregnancy and its distinction from idiopathic (immune) thrombocytopenic purpura (ITP) Thrombocytopenia associated with preeclampsia/eclampsia and the HELLP syndrome and their distinction from thrombotic thrombocytopenic purpura-hemolytic uremic syndrome (TTP-HUS)

Thrombocytopenia in pregnancy Pseudothrombocytopenia Anytime Examine blood smear for platelet clumps, or giant platelets. Repeat platelet count in citrate or heparin anticoagulant. Usually caused by agglutinins dependent upon EDTA, the standard anticoagulant for blood counts. Gestational thrombocytopenia Typically late in gestation, frequency increases as term approaches Based on 5 criteria: [1] Mild thrombocytopenia (most >100, 000/µL, rarely <70, 000/µL) [2] No thrombocytopenia outside of pregnancy [3] Occurs late in gestation [4] No fetal/neonatal thrombocytopenia [5] Postpartum resolution

GESTATIONAL THROMBOCYTOPENIA — Incidental thrombocytopenia of pregnancy, also termed gestational thrombocytopenia, is defined by the following five criteria: 1. Mild and asymptomatic thrombocytopenia 2. No past history of thrombocytopenia (except possibly during a previous pregnancy) 3. Occurrence during late gestation 4. No association with fetal thrombocytopenia 5. Spontaneous resolution after delivery

Platelet counts are typically >70, 000/micro. L, with about two-thirds being 130, 000 to 150, 000/micro. L The frequency of gestational thrombocytopenia in women admitted for labor and delivery is 5 percent. neonatal thrombocytopenia did not occur in infants born to mothers with gestational thrombocytopenia

Many, if not all, of the features of gestational thrombocytopenia are similar to those of mild ITP, suggesting a possible immunologic etiology. Several observations support the hypothesis that gestational thrombocytopenia may be a mild and transient manifestation of ITP

If the mother's thrombocytopenia is not severe and only occurs during late pregnancy or at term, if her platelet count returns to normal following delivery, and if the infant's platelet count is normal, gestational thrombocytopenia is an appropriate diagnosis.

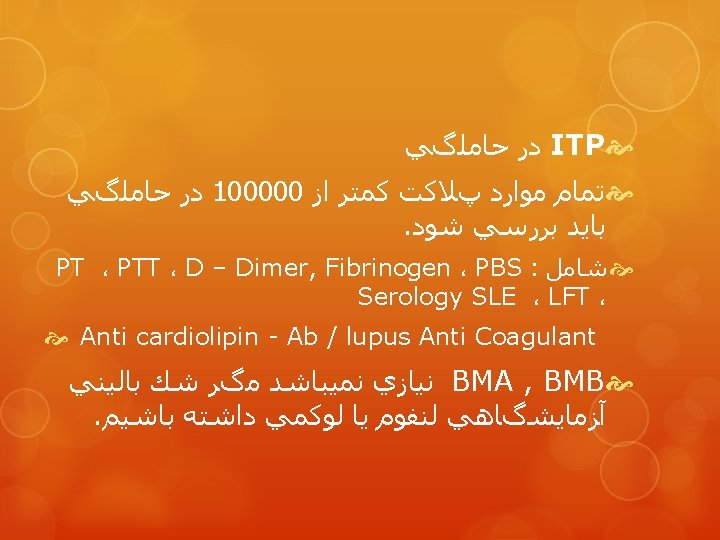
Immune thrombocytopenic purpura ITP. Anytime Presence of isolated thrombocytopenia with no evidence for alternative etiologies. May be indistinguishable from gestational thrombocytopenia if mild and occurs late during pregnancy. Platelet count may improve after delivery

ITP is the more likely diagnosis if thrombocytopenia occurs early during pregnancy or if the platelet count is very low (ie, <50, 000/micro. L). Accordingly, for women with mild thrombocytopenia who do not need treatment, the distinction from ITP may not be important during the pregnancy the distinction between ITP and gestational thrombocytopenia may not be possible during the pregnancy
 infants were")
50 women referred for thrombocytopenia discovered during pregnancy; 24 (38 percent) infants were thrombocytopenic either at birth or during the first two weeks of life

ITP DURING PREGNANCY AND DELIVERY Early in pregnancy the management of ITP is the same as if the patient were not pregnant, using prednisone as initial therapy to treat patients whose platelet counts are less than 30, 000 to 50, 000/micro. L, depending upon the presence or absence of symptoms (ie, bleeding).

Patients with chronic ITP who have persistent platelet counts less than 30, 000 to 50, 000/micro. L and who are not being treated prior to their pregnancy may need no treatment during their pregnancy, except in preparation for delivery.

Splenectomy should be deferred if possible, because the severity of thrombocytopenia may spontaneously improve after delivery. Furthermore, splenectomy may increase the risk of fetal death and premature labor in early pregnancy and uterine enlargement presents technical problems in performing a splenectomy later during pregnancy.

Rituximab is increasingly being used to treat ITP in non-pregnant patients. However, there is insufficient experience to know the safety of rituximab administered during pregnancy. It is therefore recommended to avoid rituximab during pregnancy unless the mother's health is critically dependent upon use of this medication Intravenous immune globulin (IGIV, IVIG) is an alternative TEMPORARY therapy that may help to delay splenectomy, although splenectomy remains the most effective treatment for severe, symptomatic ITP.

The greatest concern for ITP during pregnancy comes as term approaches and the risks of thrombocytopenia in the newborn infant must be considered. a summary of published case series suggests that there is an approximately 10 and 5 percent risk that the newborn infant will have a platelet count of <50, 000 or <20, 000/micro. L

The severity of ITP in the mother appears to correlate with the risk for thrombocytopenia in the infant. Neonatal thrombocytopenia may be predicted by the following situations: The mother has had a splenectomy The mother's platelet count has been <50, 000/micro. L at some time during the pregnancy

A platelet count >50, 000/micro. L is considered safe for delivery (vaginal or cesarean)

Counseling of pregnant women with ITP The following observations provide support for counseling of women with ITP who are pregnant, or who anticipate pregnancy: Although thrombocytopenia may occur in the infant, it is uncommon. Ninety percent of infants will have safe (>50, 000/microliter) or normal platelet counts. Even when severe thrombocytopenia occurs in the newborn infant, bleeding problems are almost always mild and can be effectively treated

Since intracranial hemorrhage is very rare in infants born to mothers with ITP, the occurrences should be investigated for other causes of thrombocytopenia, Cesarean delivery should be reserved for standard obstetrical indications only

Major causes of thrombocytopenia during pregnancy Spurious, due to EDTA-induced platelet aggregation Gestational thrombocytopenia Preeclampsia-eclampsia, including HELLP syndrome Autoimmune thrombocytopenia (idiopathic or related to drugs, systemic lupus erythematosus, antiphospholipid antibodies, or HIV) Disseminated intravascular coagulation Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome or, rarely, congenital TTP Congenital platelet disorders Bone marrow disease Hypersplenism

Preeclampsia After 20 weeks gestation Systolic or diastolic hypertension plus proteinuria

Criteria for the diagnosis of preeclampsia Systolic blood pressure ≥ 140 mm. Hg or Diastolic blood pressure ≥ 90 mm. Hg* and Proteinuria of 0. 3 grams or greater in a 24 -hour urine specimen •

Criteria for severe preeclampsia New onset proteinuric hypertension and at least one of the following: Symptoms of central nervous system dysfunction: Blurred vision, scotomata, altered mental status, severe headache Symptoms of liver capsule distention: Right upper quadrant or epigastric pain Nausea, vomiting Hepatocellular injury: Serum transaminase concentration at least twice normal Severe blood pressure elevation: Systolic blood pressure ≥ 160 mm Hg or diastolic ≥ 110 mm Hg on two occasions at least six hours apart Thrombocytopenia: Less than 100, 000 platelets per cubic millimeter Proteinuria: 5 or more grams in 24 hours Oliguria <500 m. L in 24 hours Severe fetal growth restriction Pulmonary edema or cyanosis Cerebrovascular accident

Acute treatment of severe hypertension in preeclampsia The goal is a gradual reduction of blood pressure to a level below 160/105 mm Hg. Sudden and severe hypotension should be avoided. Hydralazine: 5 mg IV, repeat 5 to 10 mg IV every 20 minutes to maximum cumulative total of 20 mg or until blood pressure is controlled. Labetalol: 20 mg IV, followed by 40 mg, then 80 mg at 10 minute intervals until the desired response is achieved or a maximum total dose of 220 mg is administered. Nifedipine: 10 mg orally, may repeat with 20 mg in 30 minutes

Timing of delivery is based upon gestational age, maternal and fetal condition, and the severity of preeclampsia. General management of antepartum women with mild preeclampsia consists of frequent laboratory monitoring (platelet count, liver and renal function tests), assessment of maternal blood pressure and symptoms, and frequent evaluation of fetal growth and well-being.
 be given to women diagnosed with preeclampsia")
We recommend antenatal glucocorticoids ( betamethasone) be given to women diagnosed with preeclampsia between 24 and 34 weeks of gestation We suggest delivery rather than expectant management of all women with preeclampsia who are ≥ 37 weeks of gestation Magnesium sulfate is more effective than phenytoin for prevention of eclamptic seizures. we suggest use of magnesium sulfate to prevent eclampsia in women with mild preeclampsia Mild preeclampsia is associated with good maternal and fetal pregnancy outcomes. The major consequences of severe preeclampsia are increased rates of maternal liver and kidney dysfunction, induced labor, cesarean delivery, preterm birth, fetal growth restriction, and difficulty breathing in the neonate.

Indications for delivery in preeclampsia Maternal indications Gestational age greater than or equal to 37 weeks of gestation Platelet count less than 100, 000 cells per cubic millimeter Deteriorating liver function Progressive deterioration in renal function (eg, creatinine >2 mg/d. L, oliguria) Abruptio placentae Persistent severe headaches or visual changes Persistent severe epigastric pain, nausea, or vomiting Fetal indications Severe fetal growth restriction Nonreassuring results from fetal testing Oligohydramnios

HELLP syndrome After 20 weeks gestation Diagnostic criteria for preeclampsia are present in 85 percent of cases Hemolysis: Microangiopathic hemolytic anemia with schistocytes, with other signs of hemolysis: increase serum LDH and indirect bilirubin, decreased haptoglobin Elevated liver function tests: Serum AST ≥ 70 IU/L Low platelets: Platelet count ≤ 100, 000/µL

HELLP syndrome and severe preeclampsia are probably part of a disease spectrum. We require the presence of all of the following criteria to diagnose HELLP : Microangiopathic hemolytic anemia with characteristic schistocytes (also called helmet cells) on blood smear. Other signs suggestive of hemolysis include an elevated LDH or indirect bilirubin and a low serum haptoglobin concentration (≤ 25 mg/d. L). Platelet count ≤ 100, 000 cells/micro. L Serum LDH ≥ 600 IU/L or total bilirubin ≥ 1. 2 mg/d. L Serum AST ≥ 70 IU/L

Differential diagnosis — HELLP syndrome may occasionally be confused with other diseases complicating pregnancy: acute fatty liver of pregnancy, gastroenteritis, hepatitis, appendicitis, gallbladder disease, idiopathic thrombocytopenic purpura, lupus flare, antiphospholipid syndrome, hemolytic-uremic syndrome, or thrombotic thrombocytopenic purpura

DIAGNOSIS — The diagnosis of HELLP syndrome is based upon the presence of the laboratory abnormalities comprising its name. Laboratory work-up includes ; Complete blood count with platelet count Peripheral smear AST, bilirubin, LDH We suggest obtaining these laboratory tests in all pregnant women with gestational hypertension, preeclampsia, or proteinuria with symptoms of preeclampsia

Severe maternal disease (eg, multiorgan dysfunction, disseminated intravascular coagulation, liver infarction or hemorrhage, renal failure, abruptio placenta) or nonreassuring fetal status is an indication for prompt delivery regardless of gestational age. For pregnancies ≥ 34 weeks of gestation, we recommend delivery rather than expectant management. In this population, the potential risks of preterm birth are outweighed by the risks associated with HELLP syndrome.

For pregnancies less than 34 weeks of gestation in which maternal and fetal status is reassuring, we suggest delivery after a course of glucocorticoids to accelerate fetal pulmonary maturity rather than expectant management or prompt delivery For gestations less than 30 to 32 weeks with an unfavorable cervix, we suggest cesarean delivery to avoid a potentially long induction We recommend not giving dexamethasone for treatment of HELLP syndrome. Dexamethasone does not accelerate resolution of laboratory abnormalities or reduce the risk of maternal complications.

DIAGNOSTIC CRITERIA — The diagnosis of TTPHUS is generally made on clinical grounds from the following characteristic clinical and laboratory findings : Microangiopathic hemolytic anemia Thrombocytopenia Acute renal insufficiency of varying degrees of severity Neurologic abnormalities, usually fluctuating Fever

Confirming the diagnosis For the purposes of treatment, only the presence of microangiopathic hemolytic anemia and thrombocytopenia without other cause is sufficient to make an initial diagnosis of TTP-HUS and initiate treatment with plasma exchange

TTP

: about 12 percent of TTP in pregnancy occurs in the first trimester, 56 percent in the second trimester, and 33 percent in the third trimester/postpartum, whereas preeclampsia-HELLP does not occur before 20 weeks of gestation and most cases are diagnosed in the third trimester
,")
Idiopathic TTP-HUS is associated with markedly reduced levels of ADAMTS 13 (<10 percent), often along with the presence of an autoantibody directed against ADAMTS 13. However, results of these tests should not influence the initial treatment decision to initiate plasma exchange.

TTP/HUS Typically late in gestation, frequency increases as term approaches. May occur after delivery Thrombocytopenia and microangiopathic hemolytic anemia without an alternative etiology. May be indistinguishable from severe preeclampsia or HELLP syndrome. Severe neurologic abnormalities and acute renal failure support the diagnosis of TTP/HUS. Persistent abnormalities ≥ 3 days after delivery also support the diagnosis of TTP/HUS.

For patients with severe thrombocytopenia and microangiopathic hemolytic anemia, plasma exchange may be indicated if the fetus cannot be delivered or if improvement does not follow delivery. The third postpartum day is often considered the limit for only supportive therapy or glucocorticoids without plasma exchange in anticipation of a spontaneous recovery
 continue to worsen")
If thrombocytopenia and hemolysis (as assessed by serum LDH levels) continue to worsen beyond 3 post-partum days, intervention with plasma exchange is appropriate for the presumed diagnosis of TTP-HUS Although TTP-HUS occurring at day three or four may not be distinguishable from "atypical preeclampsia/HELLP syndrome", plasma exchange treatment may also be beneficial in the latter disorder

If the disease is severe and the fetus is viable, delivery should be induced since this will resolve preeclampsia which may be confused with TTP-HUS. Although delivery does not generally cause resolution of TTP-HUS. there is anecdotal evidence that it may do so in selected patients. However, termination of the pregnancy is usually not required. There has been no report of transmission of TTP to the infant. However, intrauterine fetal death may occur due to placental infarction caused by thrombosis of the decidual arterioles

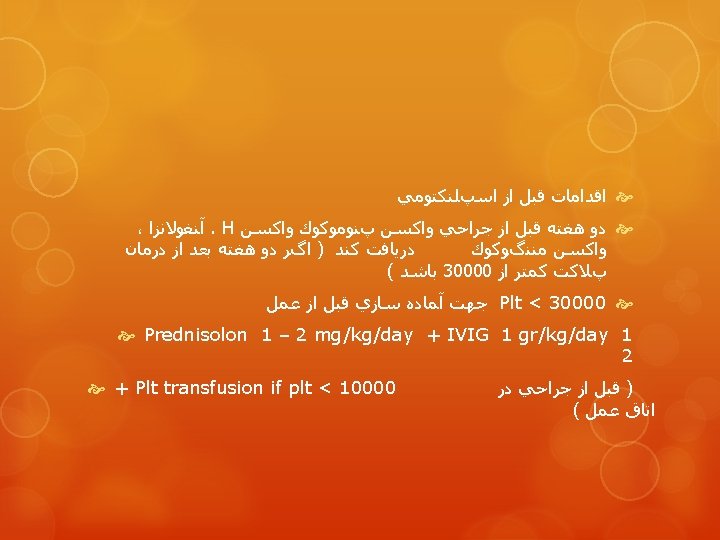
Platelet transfusion — Platelet transfusion is indicated if there is significant maternal bleeding (spontaneous or from surgical incisions), or if the platelet count is less than 20, 000 cells/micro. L. If cesarean delivery is planned, then some experts recommend platelet transfusion, as necessary, to achieve a preoperative platelet count greater than 40, 000 to 50, 000 cells/micro. L
 Anytime Complete history of drug ingestion, including nonprescription")
Drug-induced immune thrombocytopenia (except heparin) Anytime Complete history of drug ingestion, including nonprescription drugs and herbal remedies. Focus on drugs taken intermittently, or regularly for more than 1 week. Thrombocytopenia typically resolves in 5 -7 days after stopping the drug.

Heparin-induced thrombocytopenia Anytime Suspected in patients who have thrombocytopenia (or >50 percent decrease in platelet count) and who have begun heparin within previous 5 -10 days. Thrombocytopenia is typically mild; arterial or venous thrombi are commonly present. ELISA assay for heparin-dependent antibodies is sensitive; measurement of heparin-induced platelet serotonin release is more specific.
![Antiphospholipid syndrome Requires one clinical and one laboratory criterion: Clinical [1] Thrombocytopenia, [2] Adverse](http://slidetodoc.com/presentation_image_h2/a954867530dd0d1783dbda06a455d3cd/image-56.jpg "Antiphospholipid syndrome Requires one clinical and one laboratory criterion: Clinical [1] Thrombocytopenia, [2] Adverse")
Antiphospholipid syndrome Requires one clinical and one laboratory criterion: Clinical [1] Thrombocytopenia, [2] Adverse pregnancy outcome: ≥ 3 losses <10 weeks gestation or ≥ 1 loss ≥ 10 weeks gestation, <34 week delivery secondary to preeclampsia or placental insufficiency, [3] Arterial or venous thrombosis. Laboratory: Demonstration of anticardiolipin antibody, lupus anticoagulant, or positive RPR



- Slides: 60