Lecture 18 ABNORMALITIES OF FETAL MEMBRANES AMNIOTIC FLUID

Lecture 18 ABNORMALITIES OF FETAL MEMBRANES & AMNIOTIC FLUID Prof. Vlad TICA, MD, Ph. D

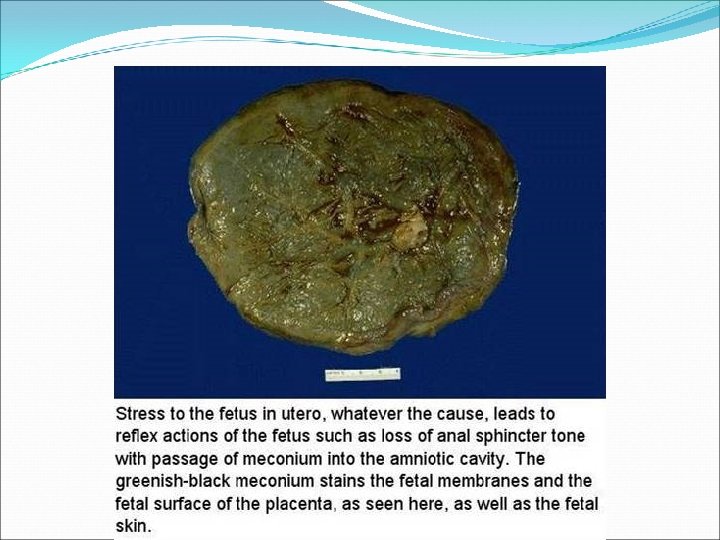
ABNORMALITIES OF FETAL MEMBRANES & AMNIOTIC FLUID MECONIUM STAINING �Staining of amniotic membrane within 1 -3 hrs after meconium passage �Neonatal mortality rate � 3. 3% in the group with meconium-stained membrane compared with 1. 7% in those without stng

CHORIOAMNIONITIS �Inflammation of fetal membrane is a manifestation of an intrauterine infection �Frequently associated with prolonged membrane rupture and long labor �(+) mononuclears & polymorphonuclear leukocytes infiltrating the chorion

DISORDERS OF THE AMNIOTIC FLUID VOLUME HYDRAMNIOS �Defined as amniotic fluid index >24 -25 cm �Mild → moderate degrees = 2 -3 L �Incidence: 1 % of all pregnancies � 2/3 - idiopathic � 1/3 is associated with fetal anomalies, maternal DM or multifetal gestation

HYDRAMNIOS �Mild hydramnios �Defined as pockets measuring 8 -11 cm in vertical dimension �Present in 85% of cases with excessive fluid �Moderate hydramnios �Defined as pockets containing only small parts & measured 12 -15 cm deep �Present in 15 %

HYDRAMNIOS PATHOGENESIS �Early in pregnancy �Amnionic cavity is filled with fluid similar in composition to ECF �During 1 st half of pregnancy �Transfer of H 2 O & other small molecules takes place not only across the amnion but thru the fetal skin � 2 nd trimester �Fetus begin to urinate, swallow & inspire amnionic fluid

HYDRAMNIOS SYMPTOMS �Severe dyspnea �Edema DIAGNOSIS �Clinical findings �Uterine enlargements in association with difficulty in palpating fetal small parts & in hearing FHT �By UTZ �Large amounts of amnionic fluid can always be demonstrated as an abnormally echo-free space between fetus & uterine wall or placenta

HYDRAMNIOS PROGNOSIS �The more severe the hydramnios, the higher the perinatal mortality rate �Maternal complication associated with hydramnios �Placental abruption �Uterine dysfunction �Postpartum hge

HYDRAMNIOS MANAGEMENT �Amniocentesis �Principal purpose is to relieve maternal distress �Amniotomy �Disadvantage is cord prolapse

HYDRAMNIOS MANAGEMENT �Indomethacin therapy �Impairs lung liquid production or enhances absorption �Decrease fetal urine production �Increase fluid movement across fetal membrane �Dose: 1. 5 -3 mg/kg/day �Disadvantage: � Potential closure of fetal ductus arteriosus
 < 5 cm �Risk: �Cord compression")
OLIGOHYDRAMNIOS �Defined as amniotic fluid index (AFI) < 5 cm �Risk: �Cord compression

OLIGOHYDRAMNIOS CONDITIONS FREQUENTLY ASSOCIATED WITH OLIGOHYDRAMNIOS Fetal Maternal Chromosomal abnormalities Uteroplacental insufficiency Congenital anomalies Hypertension Growth restriction Preeclampsia Demise DM Postterm pregnancy Ruptured membranes

OLIGOHYDRAMNIOS CONDITIONS FREQUENTLY ASSOCIATED WITH OLIGOHYDRAMNIOS Placenta Abruption Twin-twin transfusion Drugs Prostaglandin synthetase inhibitors ACE inhibitors Idiopathic

OLIGOHYDRAMNIOS EARLY-ONSET OLIGOHYDRAMNIOS �Almost always evident when there is obstruction of fetal urinary tract or renal agenesis �Exposure to ACE inhibitors �Fetal prognosis is poor

OLIGOHYDRAMNIOS PULMONARY HYPOPLASIA �Incidence @ birth: 1. 1 – 1. 4 in 1000 infants �(+) when amnionic fluid is scant � 3 possibilities that account for pulmonary hypoplasia: �Thoracic compression �Lack of fetal breathing movement decreases lung inflow �Failure to retain amnionic fluid or increase outflow with impaired lung growth and development

OLIGOHYDRAMNIOS IN LATE PREGNANCY �Amnionic fluid volume diminishes normally after 35 weeks �Significant oligohydramnios �Associated with increased risk of adverse perinatal outcomes �Fivefold increased cesarean delivery rate

AMNIOTIC FLUID EMBOLISM � 1926 - Ricardo Meyer � 1941 - Steiner & Luschbaugh autopsy series of 8 woman died of sudden shock during labor �Other studies revealed amniotic fluid debris in maternal kidney, liver, spleen, pancreas, brain
 or anaphylactoid syndrome of pregnancy �Incidence: 1/8000")
AMNIOTIC FLUID EMBOLISM �Amniotic fluid embolism (AFES) or anaphylactoid syndrome of pregnancy �Incidence: 1/8000 ~ 1/80000 �Maternal mortality: 60 ~ 90 % �AFES & Pulmonary thromboembolism → 20% perinatal maternal mortality

AMNIOTIC FLUID EMBOLISM PATHOPHYSIOLOGY �Entrance of amniotic fluid to maternal circulation: �Endocervical veins �Placental insertion site �Site of uterine trauma

AMNIOTIC FLUID EMBOLISM PATHOPHYSIOLOGY � Why Anaphylactoid Syndrome of Pregnancy? 1. A lag period 2. Amniotic debris in non-AFES mother 3. Variability of clinical signs & symptoms and its severity

AMNIOTIC FLUID EMBOLISM PATHOPHYSIOLOGY � Proposed Mechanisms: 1. Host immune responses 2. Abnormal amniotic fluid, atypical substance


AMNIOTIC FLUID EMBOLISM CLINICAL PRESENTATION � Onset most commonly during labor & delivery � Nonspecific symptoms: chills, nausea, vomiting, agitation � Cardiorespiratory collapse occurred at presentation in the majority � Some have tonic-clonic seizure

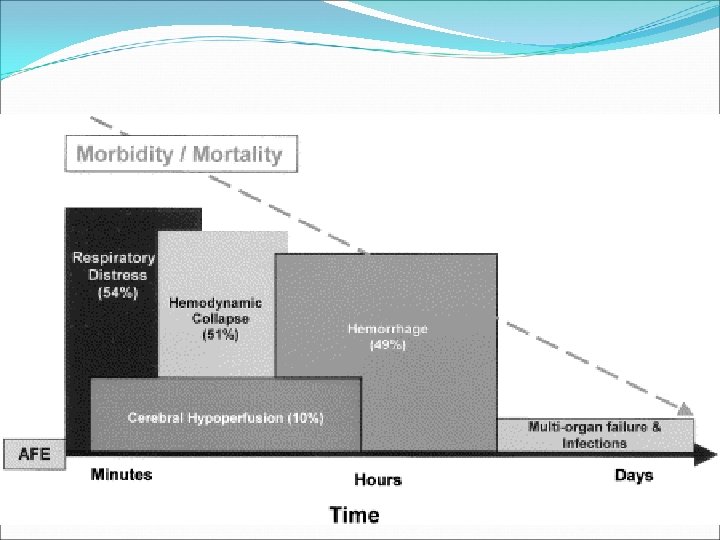
AMNIOTIC FLUID EMBOLISM CLINICAL PRESENTATION � Major clinical findings: � Hypoxia & respiratory failure � Cardiogenic shock � Disseminated intravascular coagulation (DIC) � Each of the above can be the dominant presentation

AMNIOTIC FLUID EMBOLISM CLINICAL PRESENTATION � Signs & symptoms similar to anaphylactoid or septic shock � Risk factors unknown? � Etiology unkown?
")
AMNIOTIC FLUID EMBOLISM HYPOXEMIA � Due to ventilation / perfusion mismatching � Some (15%) cases had bronchospasm � 50% - 1 st hour death were due to hypoxia and cardiogenic shock � May result in neurologic impairment

AMNIOTIC FLUID EMBOLISM HYPOXEMIA � 70% who initially survived developed pulmonary edema � May be cardiogenic / noncardiogenic � Evidence for endothelial-alveolar membrane damage → capillary leak → 1. High protein concentration in lung edema fluid 2. Amniotic fluid debris in sputum & alveoli
 � Pulmonary artery & pulmonary capillary wedge")
AMNIOTIC FLUID EMBOLISM CARDIOGENIC SHOCK (CARDIOVASCULAR COLLAPSE) � Pulmonary artery & pulmonary capillary wedge pressures ↑ � Cardiac output ↑ � LV stroke index ↑ � PA catheter data usually show CO↓ with relatively small increase in pulmonary vascular resistance � Arrhythmia, PEA, asystole may occur
 � Major clinical findings: � Hypoxia &")
AMNIOTIC FLUID EMBOLISM DISSEMINATED INTRAVASCULAR COAGULATION (DIC) � Major clinical findings: � Hypoxia & respiratory failure � Cardiogenic shock � 80% AFES develop DIC � The temporal correlation is not constant among DIC, cardiogenic shock, hypoxia � When AFES occurs postpartum and DIC is the major early finding, diagnosis may be delayed due to s/s mimics hemorrhage!

AMNIOTIC FLUID EMBOLISM DIAGNOSIS � Via symptoms & signs suspicion of AFES � Other causes of sudden cardiorespiratory failure: 1. Hemorrhage 2. Air or pulmonary embolism 3. Anesthetic complications 4. Anaphylaxis 5. Sepsis 6. Aspiration of gastric contents 7. Myocardial infarction

AMNIOTIC FLUID EMBOLISM DIAGNOSIS � Some authors require the amniotic fluid debris (eg. squamous and trophoblastic cells, mucin, lanugo) from the distal port of a pulmonary artery catheter to make the diagnosis � But, amniotic fluid components commonly are present in the maternal circulation in women with no signs & symptoms of AFES

AMNIOTIC FLUID EMBOLISM MANAGEMENT � Aggressive monitor � About maternal & fetal hypoxia � Pharmacologic therapy � Fluid support � Correct coagulopathy as needed

AMNIOTIC FLUID EMBOLISM MANAGEMENT � Monitoring: � Sp. O 2 � EKG � Arterial line � Fetal monitor if onset prior to delivery � Echocardiography � CVP alone is not sufficient � Pulmonary artery catheterization

AMNIOTIC FLUID EMBOLISM MANAGEMENT � Maternal Hypoxia � Secure airway � Intubation & Ventilation � Small tidal volume (6~8 ml/kg) � Normocapnia (~32 mm. Hg) � PEEP

AMNIOTIC FLUID EMBOLISM MANAGEMENT � Fetal Hypoxia � 65% fatal AFES present before delivery � Prevention of Fetal Hypoxia: � Maternal PO 2 keep > 47 mm. Hg; best above 65 mm. Hg � Fetal umbilical vein PO 2 >32 mm. Hg � Fetal compensation by elevated Hb level & cardiac output � Immediate delivery decreases fetal morbidity

AMNIOTIC FLUID EMBOLISM MANAGEMENT � Pharmacologic Therapy � Inotropic & vasoactive agents: � Norepinephrine � Dopamine � Dobutamine (often use norepinephrine in combination)

AMNIOTIC FLUID EMBOLISM MANAGEMENT � Fluid management � Pulmonary artery catheter insertion first, if possible � Avoid exacerbating pulmonary edema � Initial management with vasopressor is preferred � Correct coagulopathy with blood product as needed

PREMATURE RUPTURE OF THE MEMBRANES DEFINITIONS � PROM is defined as amniorrhexis prior to the onset of labor at any stage of gestation � Amniorrhexis means spontaneous rupture of membranes as opposed to amniotomy � PPROM is used to defined that the patient who are preterm with ruptured membranes, whether or not they have contractions

PREMATURE RUPTURE OF THE MEMBRANES ETIOLOGY AND RISK FACTORS � Vaginal and cervical infections � Abnormal membrane physiology � Incompetent cervix � Nutritional deficiencies

PREMATURE RUPTURE OF THE MEMBRANES DIAGNOSIS � It is based on the history of vaginal loss of fluid and confirmation of amniotic fluid in the vaginal � A sterile vaginal speculum examination should be performed � Before labor, vaginal examination should not be performed � Carry out a complete ultrasonic examination

PREMATURE RUPTURE OF THE MEMBRANES DIAGNOSIS � Confirmation of the diagnosis can be made by: � Testing the fluid with nitrazine paper, which will turn blue in the presence of the alkaline amniotic fluid � Placing a sample on a microscopic slide, air drying, and examining for ferning

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT � General considerations � Conservative expectant management � Management of chorioamnionitis � Tests of pulmonary maturity

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT General considerations � Membranes are a natural barrier to prevent infections � PPROM has high risks of infections and sepsus � PPROM can lead to oligohydramnios

PREMATURE RUPTURE OF THE MEMBRANES DIAGNOSIS OF OLIGOHYDRAMNIOS � Ultrasonic definition has been standardized � Criteria include: 1. Measure the amniotic fluid present in 4 quadrands by vertical axis 2. AFI: total being called the amniotic fluid index 3. A value < 5 cm is considered abnormal

PREMATURE RUPTURE OF THE MEMBRANES OLIGOHYDRAMNIOS RESULTS IN: � Fetal crowding with thoracic compression � Restriction of fetal breathing � Disturbances of pulmonary fluid production and flow � Constaints placed on fetal movements in utero can also result in positional skeletal abnormalities, such as talipes equinovarus

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT � If PROM occurs at 36 weeks or later, condition of the cervix is favorable, no spontaneous contractions, labor should be induced after 6 -12 hours � If PROM occurs prior to 36 weeks’ gestation, we should manage as followings:

PREMATURE RUPTURE OF THE MEMBRANES LABORATORY TESTS � Complete blood cells � Gram stain and culture of amniotic fluid � Pulmonary maturation studies of amniotic fluid

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT Conservative expectant management � The goal is to continue the pregnancy until the lung profile is mature � Take careful surveillance to diagnose subclinical infection and chorioamnionitis

PREMATURE RUPTURE OF THE MEMBRANES CLINICAL SIGNS & SYMPTOMS OF CHORIOAMNIONITIS � Maternal temperature is > 38 0 C � Fetal tachycardia � A tender uterus � Uterine irritability on nonstress testing � White blood cells elevates � Measure the amniotic fluid by ultranography

PREMATURE RUPTURE OF THE MEMBRANES

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT OF CHORIOAMNIONITIS � Use antibiotics depends on cultures and sensitivity � Once antibiotics have been started, labor should be induced � Vaginal delivery or cesarean section

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT OF CHORIOAMNIONITIS � Use antibiotics depends on cultures and sensitivity � Once antibiotics have been started, labor should be induced � Vaginal delivery or cesarean section

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT � Tocolytic therapy � Corticosteriods � Labor and delivery They are just the same with preterm labor !
 ratio")
PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT Tests of pulmonary maturity: � Lecithin/sphingomyelin (L/S) ratio maturity > 2 � Lamellar body number density (LBND) � Maturity: > 46. 000 LBND

PREMATURE RUPTURE OF THE MEMBRANES MANAGEMENT � Surfactant therapy � It is effective � Expensive

THANKS !
- Slides: 58