Teresa Gamucci Direttore Oncologia Medica ASL Frosinone Adiuvante



 probabile")

 Danno")


















 Assay Calculation of the Recurrence Score Result")





 Tamoxifen 20 mg PO QD x 5 yrs")
 and Overall Survival (OS) in Tamoxifen Alone Group RS Group")
 p-value*")

 • Donna 42 anni • Premenopausa • Marzo 2016 Intervento di")
 • Donna 65 anni • Postmenopausa • Febbraio Intervento di quadrantectomia")

- Slides: 55
Teresa Gamucci Direttore Oncologia Medica ASL Frosinone
Adiuvante e neoadiuvante: quali dubbi? • Dubbi? SI TANTI • Adiuvante o neoadiuvante : non è tanto questo il problema • Sottotipi molecolari: partiamo da qui
Malattia HER 2 positiva Quali dubbi? • Donna di 70 anni, giovanile • Lieve ipertensione arteriosa, lieve ipercolesterolemia • Nodulo mammario di 2 cm, linfonodi ascellari ecograficamente negativi E. I. carcinoma duttale infiltrante G 2 ER=neg Pg. R=neg ki 67=25% HER 2= 3+ • Seno piccolo DECISIONE
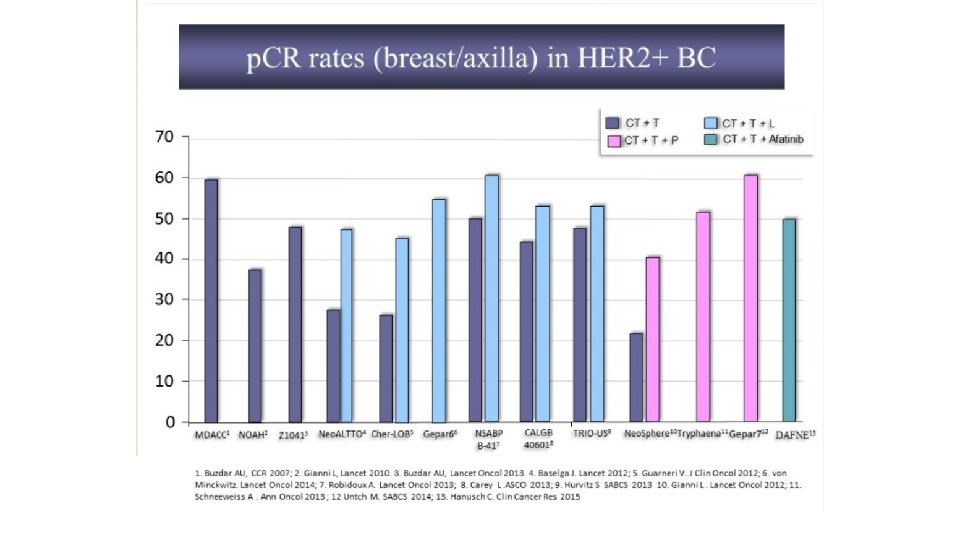
Scenari • Chemioterapia neoadiuvante con 4 EC 12 Paclitaxel + Trastuzumab (+ Pertuzumab) probabile RC intervento “minimo” + BLS Trastuzumab • Intervento chirurgico “più ampio” +BLS Chemioterapia adiuvante EC x SBAGLIATO! 4 12 Paclitaxel + Trastuzumab x 1 anno • Intervento chirurgico “più ampio”+ BLS Chemioterapia adiuvante 12 Paclitaxel + Trastuzumab x 1 anno
205 pts 10 Centri Oncologici Italiani 2003 -2011
Meccanismi di cardiotossicità acuta e tardiva delle antracicline 4 2 3 4 1) Danno DNA, topoisomerasi II 2) Aumentato stress ossidativo 3) Alterato metabolismo energetico (ATP), 4) Attivazione di morte cellulare (apoptosi/necrosi) 1 Sawyer DB et Al. Progr Cardiovasc Dis 2010
Congestive heart failure: antracicline e Trastuzumab No difference in the cardiotoxicity profile in trials with concurrent as compared to sequential administration of chemotherapy and trastuzumab 2012
406 pts Paclitaxel + Trastuzumab x 12 Trastuzumab
Results 3 years-rate = 99. 2% 3 years-rate = 98. 7% Tolaney, S. M. et al, NEJM 2’ 15
493 pts Docetaxel + Ciclofosfamide q 21 + Trastuzumab sett x 4 cicli Trastuzumab
Results 2 years DFS = 97. 8% 2 years OS = 99. 2% Jones SE et al, Lancet Oncology 2013
Malattia triplo-negativa Quali dubbi? • Donna di 39 anni • Zia materna operata a 50 anni per ca ovaio • Nodulo mammario di 3 cm, linfonodi ascellari ecograficamente positivi E. I. carcinoma duttale infiltrante G 3 ER=neg Pg. R=neg ki 67=35% HER 2= neg
The rate of pathologic complete response according to ER status Bedard PL. and Cardoso F. Nat Rev Clin Oncol 2011
196 pts ESMO 2015
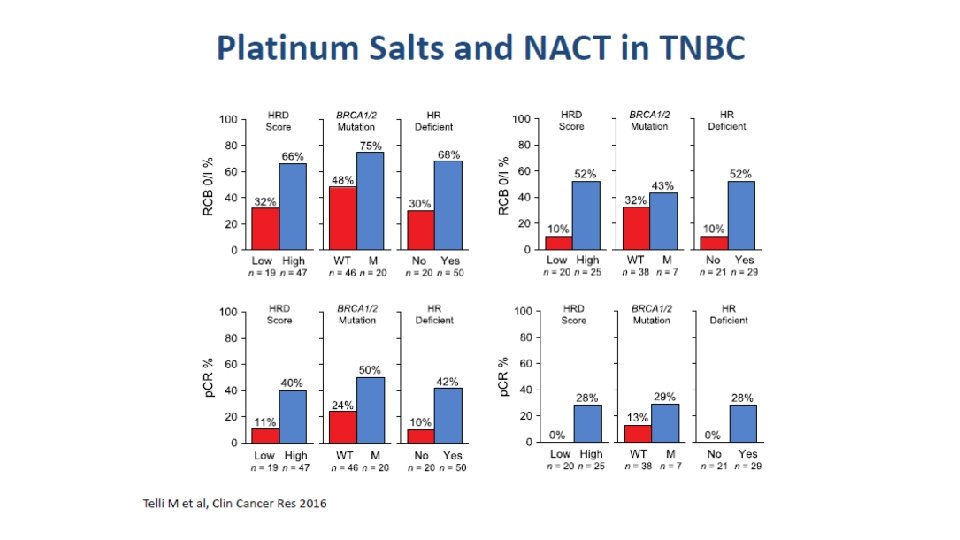
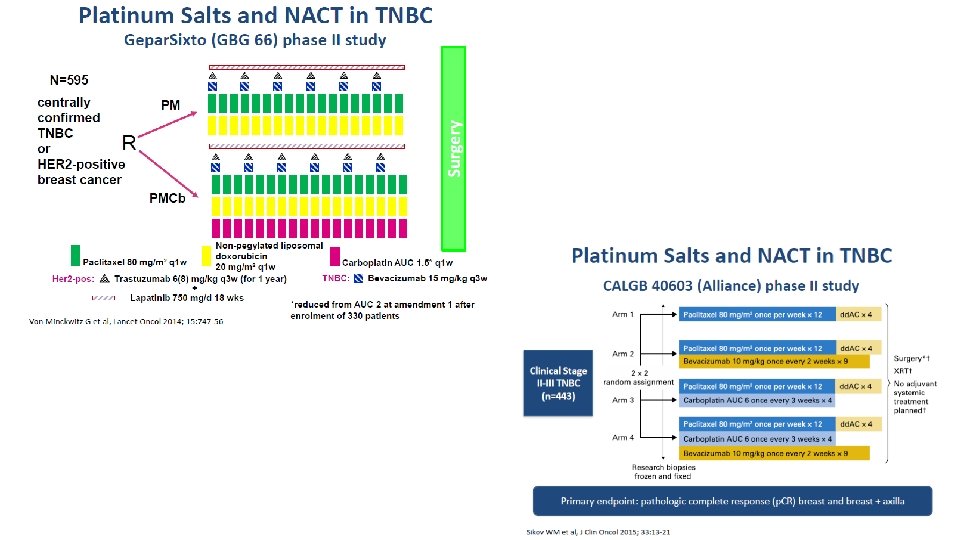
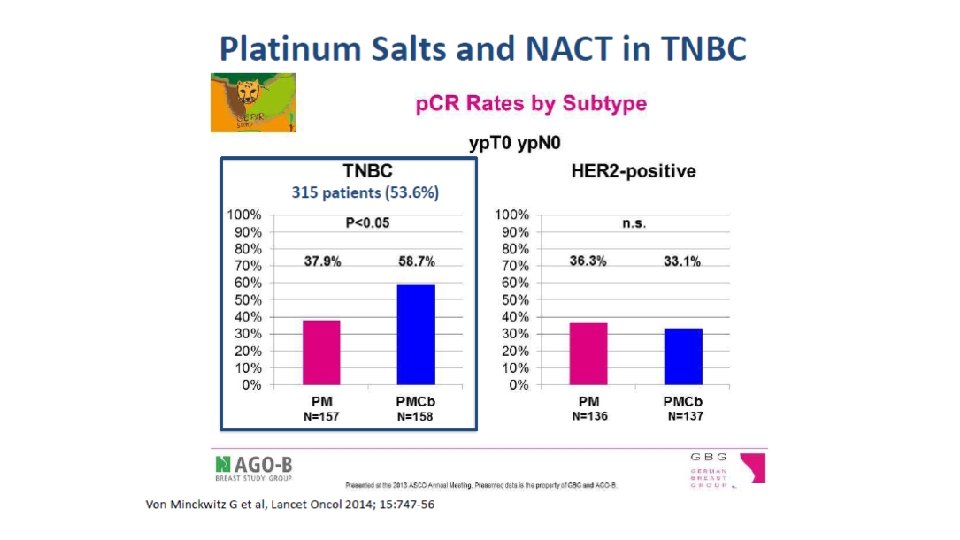
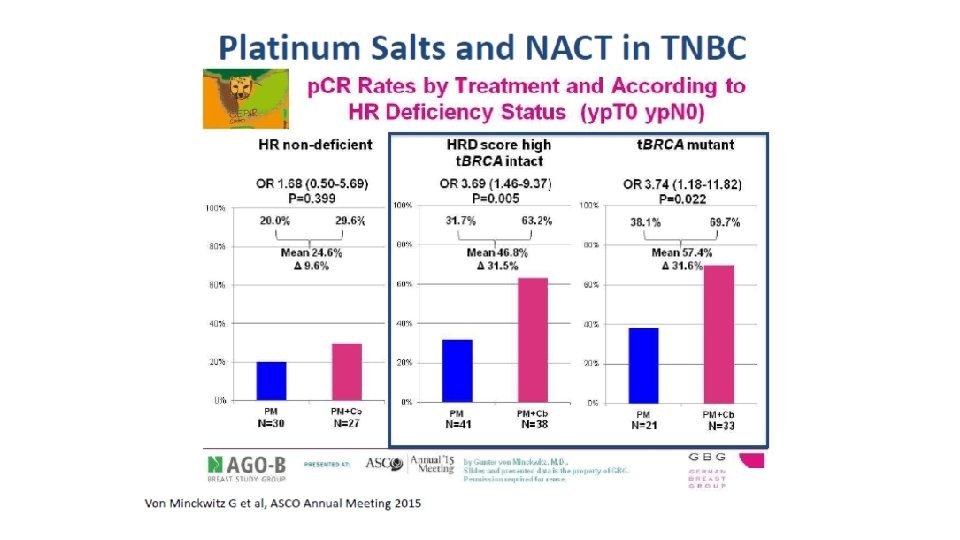
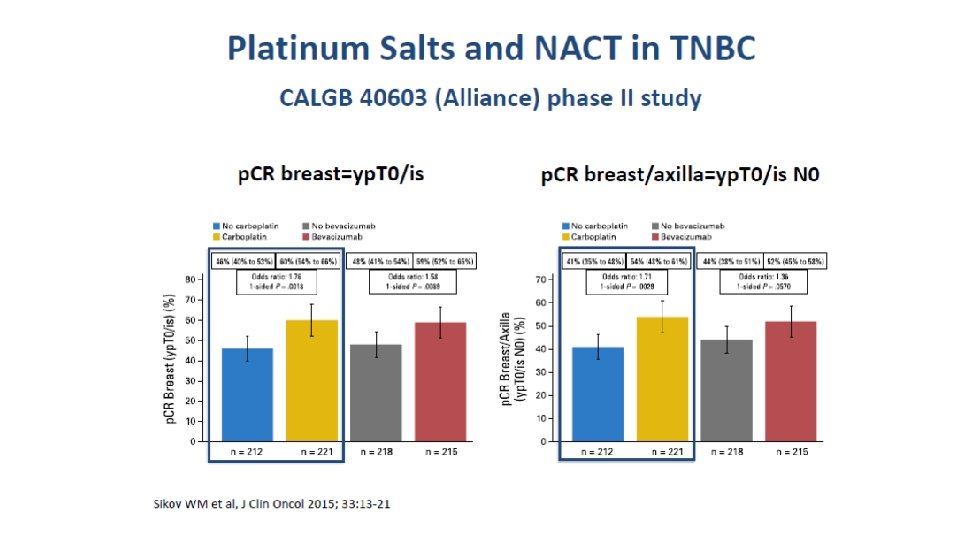
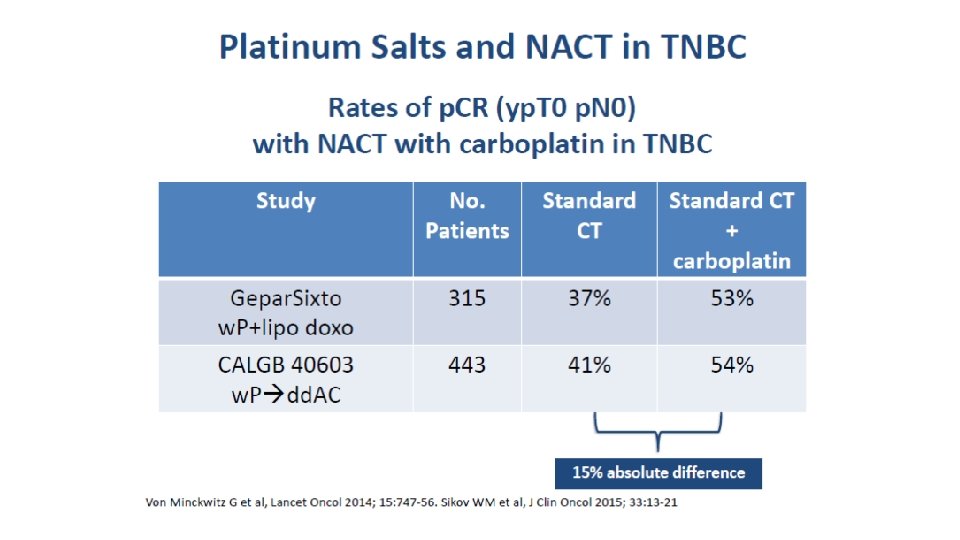
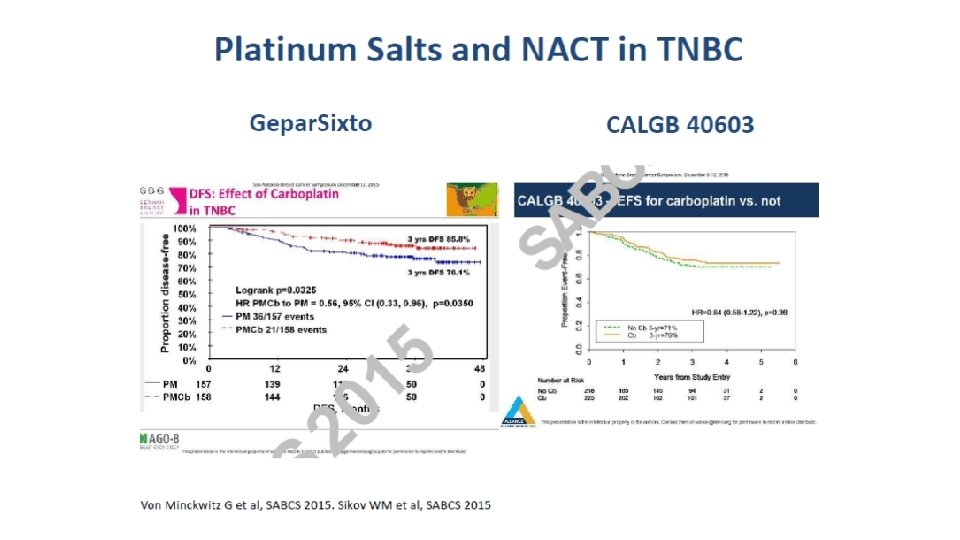
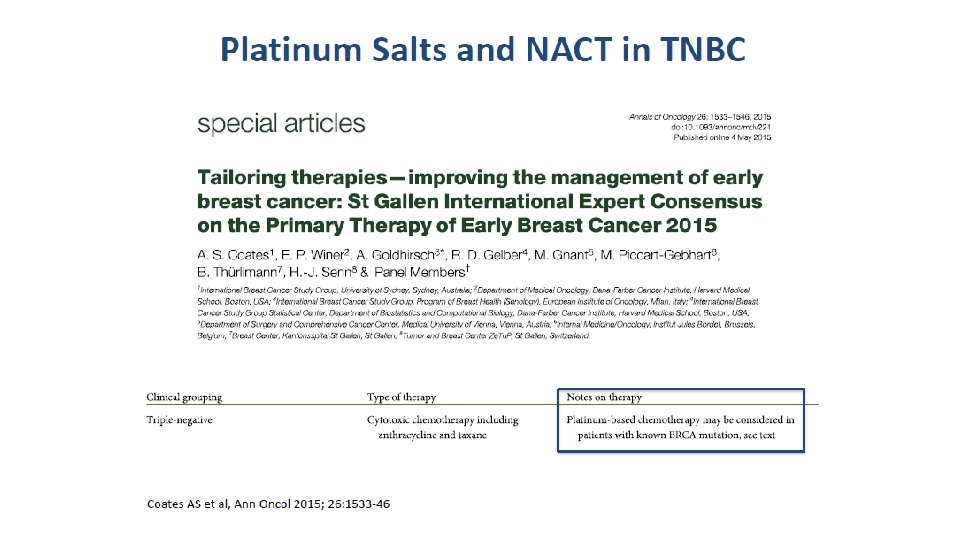
Malattia triplo-negativa Quali dubbi? DECISIONE CHEMIOTERAPIA NEOADIUVANTE QUALE? Platino si/Platino no
Critiche all’utilizzo dei Sali di platino nelle pazienti TN • I Sali di platino funzionano nelle BRCA mutate • La maggior parte delle paz BRCA mutate sono TN • Negli studi con sali di platino, la risposta ottenuta è dovuta al grippo delle BRCA mutate IN REALTA’ FORSE NO…
Azione del cisplatino
Sali di platino • In situations where the DNA repair is compromised synthetic lethality of the cell depends on • DNA repair factors deficient in functioning: • BRCA gene deficient in genotype or phenotype • Other Homologues Recombination Repair factors deficient in functioning (HRD) , eg ATM, MDC 1, MRE 11 • In presence of DNA damaging agents • Chemotherapy (Especially Platinum salts) • Radiotherapy
HRD is Strongly Linked with Cancer Breast BRCA 1 ATM BRCA 2 MDC 1 BRCA 1 ATM BRCA 2 Mre 11 H&N ATM Mre 11 NSCLC MDC 1 Ovarian Mre 11 TN Breast FANC BRCA CHK 2 MDC 1 Serous Ovarian ATM BRCA ATM /MRE 11 GI, HCC Mre 11 Head & Neck ATM /MRE 11 Pancreas BRCA 1 Paediatrics FANC NSCLC CRC MDC 1 MRE 11 BRCA 2 Kolvenbag G, 2015
Malattia Luminale Quali dubbi? Tumori Luminali: le decisioni difficili Luminal B = ER e/o Pg. R bassi e/o ki 67 < 20% HER 2 – Quando abbiamo davvero bisogno di aiuto da un test genomico?
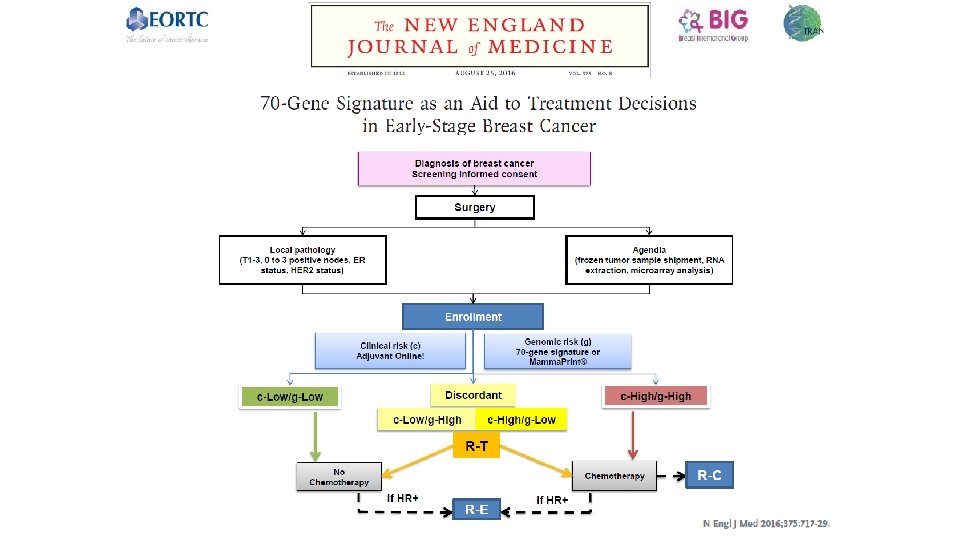
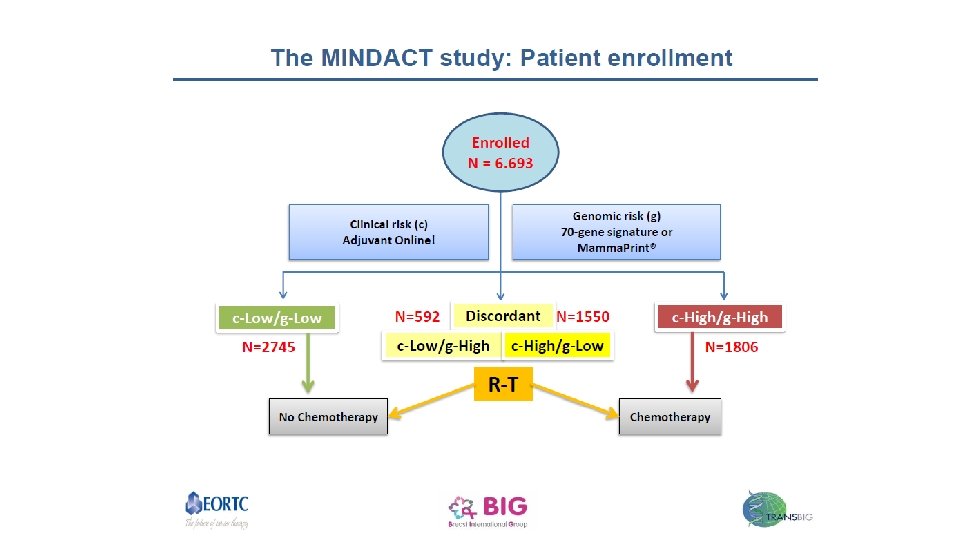
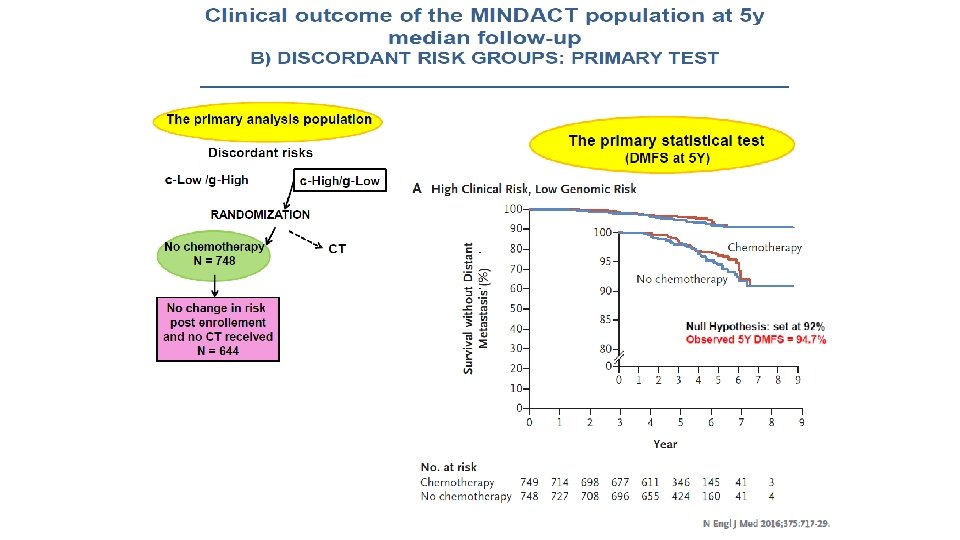
Discordant risk groups
MINDACT: Conclusions • MINDACT trial demonstrated that genomics can provide important informations in order to treat patients with EBC ● C-High/g-Low patients, including 48% Node positive, had a 5 -year DMFS rate in excess of 94%, whether randomized to adjuvant CT or no CT ● In the entire MINDACT population, the trial confirmed the hypotesis that the ‘genomic’ strategy leads to a 14% reduction in CT prescription versus the ‘clinical’ strategy. ● Among the c-High risk patients, the clinical use of Mammaprint is associated with a 46% reduction in chemotherapy prescription.
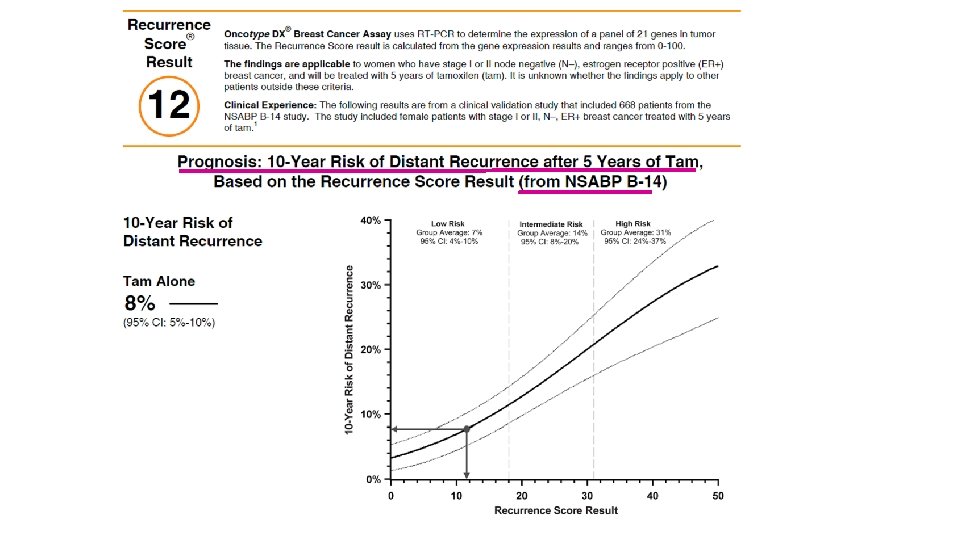
Oncotype DX® 21 -Gene Recurrence Score® (RS) Assay Calculation of the Recurrence Score Result Coefficient x Expression Level RS = + 0. 47 x HER 2 Group Score - 0. 34 x ER Group Score + 1. 04 x Proliferation Group Score + 0. 10 x Invasion Group Score + 0. 05 x CD 68 - 0. 08 x GSTM 1 - 0. 07 x BAG 1 Category RS (0 -100) Low risk RS <18 Int risk RS ≥ 18 and <31 High risk RS ≥ 31 Paik et al. N Engl J Med. 2004; 351: 2817 -28
The Recurrence Score® Result Stratifies Patients by their 10 -Year Distant Recurrence-Free Survival Paik et al. N Engl J Med. 2004; 351: 2817 -2826 Paik et al. N Engl J Med. 2004; 351: 2817 -28
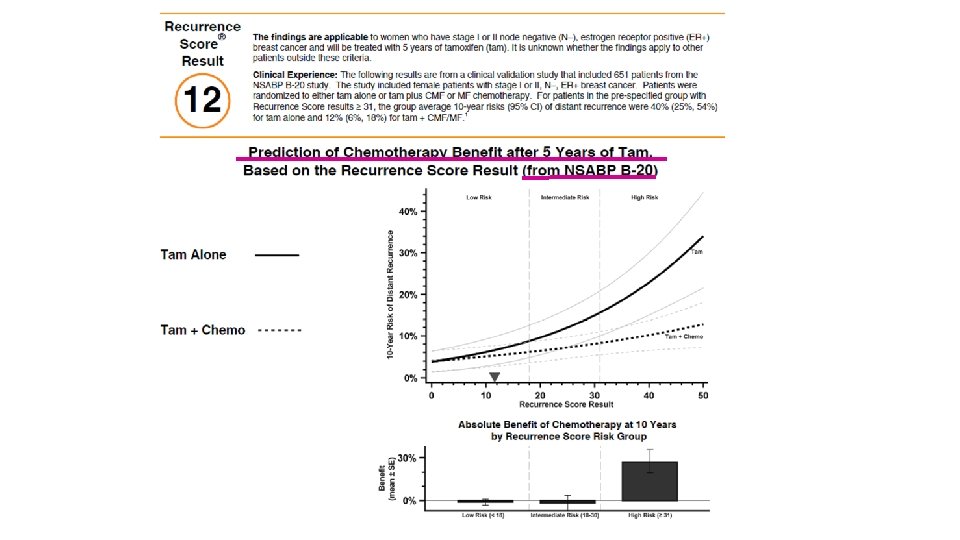
Chemotherapy Benefit and Oncotype DX® NSABP B-20 Chemo Benefit Study in N–, ER+ Pts Design Tam + MF Randomized Tam + CMF Tam Objective: Determine the magnitude of the chemo benefit as a function of the 21 -gene RS assay Paik et al. J Clin Oncol. 2006; 24: 3726 -3734. 42
The Oncotype DX® Assay: Patients Do Not Benefit Equally from Chemotherapy All patients Low RS Little, if any, benefit 28% Absolute Benefit Intermediate RS High RS Paik et al. J Clin Oncol. 2006; 24: 3726 -3734
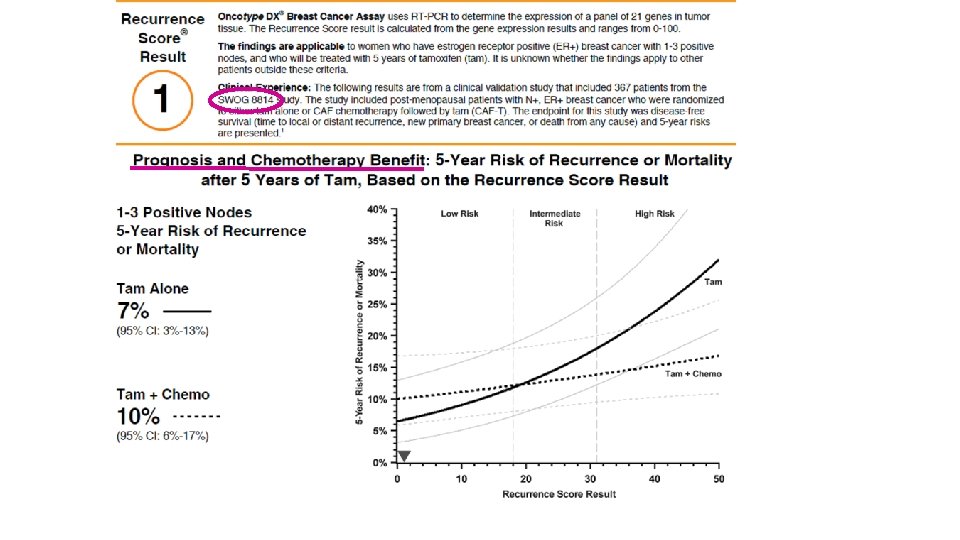
Prognostic and Predictive Value of the 21 -Gene Recurrence Score Assay in Postmenopausal Women with Node-Positive, Estrogen- Receptor-Positive Breast Cancer on Chemotherapy: A Retrospective Analysis of a Randomised Trial Albain KS et al. Lancet Oncol 2010; 11(1): 55 -65. Albain KS et al. San Antonio Breast Cancer Symposium 2009; Abstract 112.
21 -Gene Recurrence Score Assay in Postmenopausal Women with Node-Positive, Estrogen- Receptor-Positive Breast Cancer • • • A low 21 -gene recurrence score (RS) in postmenopausal patients with ER-positive, node-negative breast cancer predicts a lack of benefit from the addition of chemotherapy to tamoxifen (T) treatment (JCO 2006; 24: 3726). The value of the 21 -gene recurrence score assay in patients with ER-positive, nodepositive breast cancer that are treated with T alone is unknown. Study objectives: • Assess prognostic value of the 21 -gene recurrence score in patients with node -positive breast cancer treated only with T. • Assess whether 21 -gene recurrence assay allows for the prediction of a nodepositive subset of patients who do not benefit from anthracycline-based chemotherapy. Albain KS et al. Lancet Oncol 2010; 11(1): 55 -65.
SWOG-8814: Parent Trial Schema Tamoxifen (T) Tamoxifen 20 mg PO QD x 5 yrs Eligibility (n=1, 477) Postmenopausal ER or PR positive Axillary lymph node positive mg/m 2 CAF = Doxorubicin 30 day 1, day 8 Cyclophosphamide 100 mg/m 2 PO days 1 -14 5 -FU 500 mg/m 2 day 1, day 8; Cycle repeated q 28 days * Excluded R CAF-T CAF x 6 Cycles T x 20 mg PO QD x 5 yrs CAFT* CAF x 6 Cycles Concurrent T 20 mg PO QD x 5 yrs from analysis due to inferior efficacy Albain KS et al. Lancet Oncol 2010; 11(1): 55 -65.
Ten-Year Disease-Free Survival (DFS) and Overall Survival (OS) in Tamoxifen Alone Group RS Group 10 -year DFS Low (<18) 60% Intermediate (18 -30) 49% High (≥ 31) 43% DFS p-value* 10 -year OS OS p-value* 77% 0. 017 68% 0. 003 51% *Log-rank p-value stratified according to the number of positive nodes (1 -3 vs ≥ 4 positive nodes). Albain KS et al. Lancet Oncol 2010; 11(1): 55 -65.
Hazard Ratio: Ten-Year DFS, T versus CAF-T Groups RS Group HR (95% CI) p-value* Low (<18) 1. 02 (0. 54 -1. 93) 0. 97 Intermediate (18 -30) 0. 72 (0. 39 -1. 31) 0. 48 High (≥ 31) 0. 59 (0. 35 -1. 01) 0. 033 Entire RS sample — 0. 054 *Log-rank p-value stratified according to the number of positive nodes (1 -3 vs ≥ 4 positive nodes); HR = hazard ratio. Albain KS et al. Lancet Oncol 2010; 11(1): 55 -65
Conclusions • The RS is prognostic for patients with node-positive breast cancer treated with tamoxifen alone. • A high RS score predicts an improved DFS in patients with node-positive breast cancer treated with anthracyline-based chemotherapy followed by tamoxifen compared to tamoxifen alone. • A low RS score identifies women with node-positive breast cancer who may not benefit from the addition of anthracycline-based chemotherapy to tamoxifen treatment. Albain KS et al. Lancet Oncol 2010; 11(1): 55 -65.
Caso clinico (1) • Donna 42 anni • Premenopausa • Marzo 2016 Intervento di quadrantectomia SE mammella dx + biopsia linfonodo sentinella - E. I. Carcinoma duttale infiltrante della mammella G 3 - p. T 1 c(18 mm) p. N 0(sn) ER=100% Pg. R=100% ki 67=30% HER 2=score 0 ?
Caso clinico (2) • Donna 65 anni • Postmenopausa • Febbraio Intervento di quadrantectomia SI mammella dx + linfectomia ascellare - E. I. Carcinoma duttale infiltrante della mammella G 2 - p. T 1 c (1. 4 cm) p. N 1 a(1/14) ER=98% Pg. R=80% ki 67=32% HER 2=score 0 ?
Grazie per l’attenzione Sora Frosinone Cassino