Shiny liver Dr Ahmed Refaey FRCR Consultant Radiologist







































- Slides: 41
Shiny liver Dr. Ahmed Refaey FRCR Consultant Radiologist Prince Sultan Military Medical City
Format of the lecture • Detection of liver masses by CT • Hypervascular tumors of the liver • Case of the day
Detection of liver masses by CT * Triphasic study * arterial phase * portal venous phase * equilibrium phase ( delayed phase )
• When we give IV contrast, it is important to understand that there is a dual blood supply to the liver. • Normal parenchyma is supplied for 80% by PV & only for 20% by hepatic artery, so it will enhance in the portal venous phase. • All liver tumors however get 100% of their blood supply from hepatic artery , so when they enhance it will be in arterial phase
• In the arterial phase hypervascular tumors will enhance via the hepatic artery , when normal liver parenchyma does not yet enhances , because contrast is not yet in the portal venous system. • These hypervascular tumors will be visible as hyperdense lesions in a relatively hypodense liver
• In the portal venous phase hypovascular tumors are detected when the normal liver parenchyma enhances maximally. • These hypovascular tumors will be visible as hypodense lesions in a relatively hyperdense liver.
• In the equilibrium phase at about 10 minutes after contrast injection , tumors become visible, that either : - retain their contrast ( become relatively hyperdense to the normal liver ) - wash out their contrast faster than normal liver parenchyma ( become relatively hypodense to the normal liver ).
Hemangioma hcc
• Above: arterial phase showing hypervascular FNH • Middle: portal venous phase showing hypovascular metastases • Down: equilibrium phase showing relatively dense cholangiocarcinoma
Arterial phase imaging
Optimal timing Hypervascular tumors will enhance optimally at 35 seconds after contrast injection (late arterial phase)
• A patient who underwent two phases of arterial imaging at 18 and 35 seconds. • In the early arterial phase we nicely see the arteries , but we only see some irregular enhancement within the liver. • In the late arterial phase, we can clearly identify multiple tumor masses.
Portal venous phase
• Portal venous phase imaging work on the opposite idea. We image the liver when it is loaded with contrast through the portal vein to detect hypovascular tumors. • The best moment to start scanning is at about 75 sec.
• Hypovascular metastases seen as hypodense lesions in late portal venous phase
Liver metastases cancer colon
Equilibrium phase
• Starts when contrast is moving away from the liver and the liver starts to decrease in density. • This phase begins at about 3 -4 minutes after contrast injection and imaging is best done at 10 minutes after contrast injection.
• This phase can be valuable if you are looking for: 1 - fast tumor washout in hypervascular tumors 2 - retention of contrast in blood pool like in hemangioma 3 - retention of contrast in fibrous tissue in capsule ( HCC )or scar tissue ( cholangiocarcinoma or FNH )
• 1 - fast tumor washout in hypervascular tumors like HCC
• 2 - retention of contrast in the blood pool as in hemangioma
• 3 - retention of contrast in fibrous tissue in capsule ( HCC ) or scar tissue (cholangiocarcinoma , FNH)
Hypervascular hepatic tumors • 1 ry • • 2 ry Benign • Hypervascular Hemangioma metastasis Focal nodular hyperplasia • Primary hypervasculr tumours adenoma • Thyroid carcinoma • Choriocarcinoma Malignant • Renal cell carcinoma • Iselet cell tumors of pancreas HCC • Malignant pheochromocytoma Fibrolamellar HCC • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
Case of the day
• History : A 40 year old male came with abdominal pain
• Technique Triphasic contrast enhanced CT was performed for the chest, abdomen and pelvis.
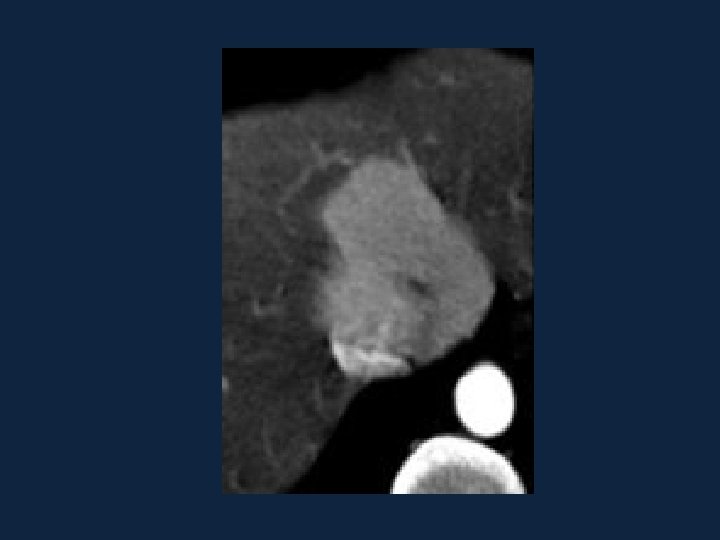
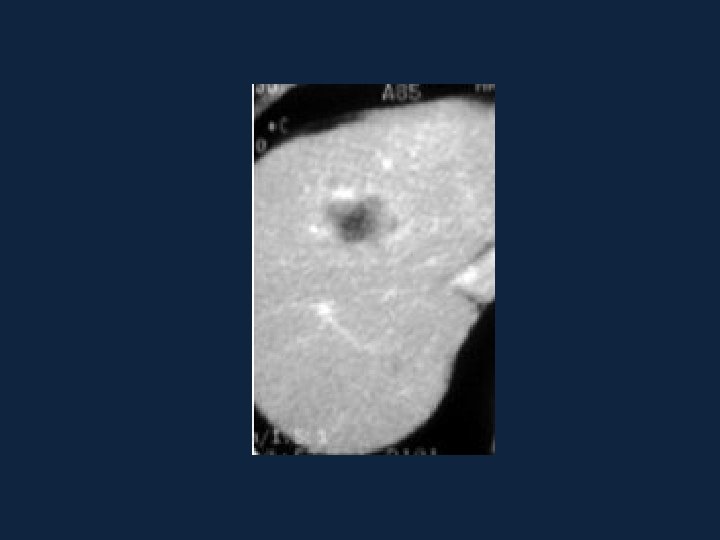
Arterial phase PV phase
Hypervascular hepatic tumors • 1 ry • 2 ry • Benign • Hypervascular • Hemangioma metastasis • Focal nodular hyperplasia • Primary hypervasculr tumours • adenoma • Thyroid carcinoma • Choriocarcinoma • Malignant • Renal cell carcinoma • Iselet cell tumors of • HCC pancreas • • Malignant pheochromocytoma Malignant melanoma Carcinoid tumor 15% of cancer breast
• • • Primary hypervasculr tumours Thyroid carcinoma Choriocarcinoma Renal cell carcinoma Iselet cell tumors of pancreas Malignant pheochromocytoma Malignant melanoma Carcinoid tumor 15% of cancer breast
• Primary hypervasculr tumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
• • • Primary hypervasculr tumours Thyroid carcinoma Choriocarcinoma Renal cell carcinoma Iselet cell tumors of pancreas Malignant pheochromocytoma Malignant melanoma Carcinoid tumor 15% of cancer breast
• • • Primary hypervasculr tumours Thyroid carcinoma Choriocarcinoma Renal cell carcinoma Iselet cell tumors of pancreas Malignant pheochromocytoma Malignant melanoma Carcinoid tumor 15% of cancer breast
• Location of carcinoid tumor: • Appendix ……………. 45% • Small bowel …………… 35% - ilium ( 91%). . Jejenum (7%). . Duodenum ( 2%) • Rectum ………………. . 10% • Colon ………………. . 5% • Stomach ……………. . < 3%
• Diagnosis Carcinoid tumor of the stomach with hypervascular metastasis to the liver
Carcinoid tumor
Carcinoid tumor • Low-grade malignancy, resemble adenocarcinoma, but do not have their aggressive behaviour • Clinical presentation: • Asyptomatic ( 66%) • Abdominal pain/intestinal obstruction ( 19%) • Nausea, weight loss (16%) • Palpable mass ( 14%) • Carcinoid syndrome ( 7%)
• Carcinoid syndrome: • Cause: excess serotonin level when the metabolic pathway to 5 -HIAA is bypassed (a) with extensive liver metastasis (b) with 1 ry pulmonary/ovarian carcinoids • Recurrent diarrhea (70%) • Right sided endocardial fibroelastosis (35%), resulting in tricuspid regurgitation and right heart failure • Desquamative skin lesions / pellagra /nausea /vomiting /fever/cutaneous flushing …. . (5%) • Prognosis: carcinoid syndrome has a higher morbidity and mortality than does the tumor itself
Thank you