1 Liver Topics 1 Liver Basics 2 Liver

1

Liver Topics 1. Liver Basics 2. Liver trauma 3. Liver infections 4. Liver cirrhosis and portal hypertension 5. Liver tumors 6. Liver resection and transplantation 7. Collection and revisions ? ? ?

Liver infections BY Prof. MOHAMMED A. OMAR Assistant Professor of HPB Surgery and Laparo endoscopy For contact: • elqefty@yahoo. com • 01064184848 • https: //www. facebook. com/Dr. Mohammed. Ahmed. Omar 3

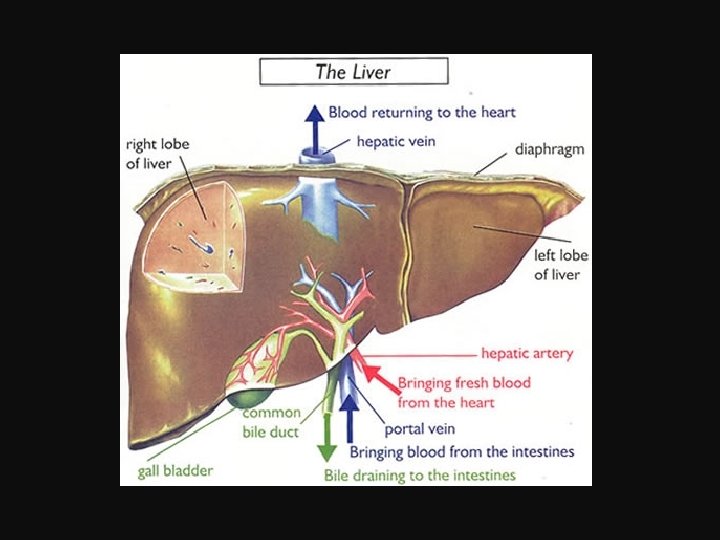
Introduction The following are the liver infections with surgical interest: 1. Viral hepatitis. 2. Pyogenic liver abscess. 3. Amoebic hepatitis and abscess. 4. Hydatid disease of the liver. 5. Hepatic Schistosomiasis. 6. Cholangitis.

Pyogenic liver abscess

Introduction • Highly fatal disease. • The key to improving the results of its treatment is an early diagnosis. • The development of modern diagnostic and interventional radiology, together with the evolution of antibiotics, contributed to a safer management of the problem
 Sources & routes of infection 1. Biliary tract (cholangitic abscess): This is")
Etiology (A) Sources & routes of infection 1. Biliary tract (cholangitic abscess): This is the commonest of all sources. • Cause: Ascending cholangitis • Organism: The likely organism is E. coli or other gram negative bacilli. 2. Portal vein (pyaemic abscess): • Cause: Suppurative appendicitis or colon diverticulitis. • Organism: Streptococci and anaerobes are the commonest organisms. 3. Arterial system (haematogenous abscess): • Cause: bacterial endocarditis, tonsillitis, or osteomyelitis. • Organism: Staphylococcus aureus is the usual causative organism. 4. Super added infections: • Amoebic liver abscess. • Hydatid cyst. 5. Direct spread: • Internally: gangrenous cholecystitis, penetrating peptic ulcer, …. . . • Externally: both penetrating and non penetrating trauma. 6. Idiopathic (cryptogenic): The source of infection is not possible to trace.
 Predisposing factors 1) Decreased immunity: 2) Secondary infection: An already existing liver lesion")
(B) Predisposing factors 1) Decreased immunity: 2) Secondary infection: An already existing liver lesion as • Infected hydatid cyst. • Infected amoebic abscess. • Infected haematoma. (C) Causative organism • The infection is polymicrobial in 45%. • Escherichia coli and Streptococcus milleri are the most frequently isolated organisms, but other enteric organisms such as Streptococcus faecalis, Klebsiella and Proteus vulgaris also occur.

Pathology • Site: more commonly in the right lobe. • Size: variable. • Content: § Liver parenchymal cell necrosis § Polymorphonuclear leucocytes and lymphocyte infiltration § Viable bacteria on the periphery. § Ultimately a fibrous capsule containing pus.

Clinical features Symptoms • Generally: High fever, rigors, profuse sweating, anorexia, nausea & vomiting. • Locally: Right hypochondrial or lower chest pain. Signs • Generally: Fever & tachycardia. • Locally: Tenderness at right hypochondrium & lower chest or tender hepatomegaly.

Complications 1. Recurrent bacteraemia. 2. Direct extension of the abscess. 3. – Pleural or pericardial effusion – Empyema Rupture of the abscess – Rupture into the pericardium, thoracic and abdominal fistula formation 4. Portal vein thrombosis =24 % 5. Hepatic Vein thrombosis= 22 % 6. Splenic vein thrombosis 7. Metastatic septic endophthalmitis occurs in as many as 10% of diabetic patients with a liver abscess caused by Klebsiella pneumoniae.

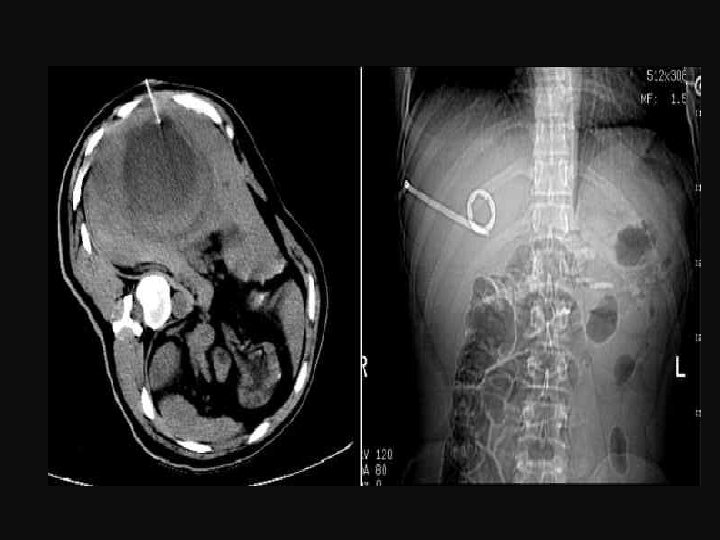
Investigations Laboratory 1. Blood picture: Leucocytosis & anaemia. 2. ESR: A high ESR. 3. Liver function test: 4. Blood culture: usually positive when taken during the height of pyrexia. Imaging 1. Abdominal ultrasound or CT scan 2. Abdominal X ray: 3. Chest radiography: Plain abdominal x ray demonstrating an abnormal collection of air in the right upper quadrant consistent with a pyogenic hepatic abscess.

• CT Scan showing air fluid level & rim enhancement with intravenous contrast typical of liver abscess
 Non opera tive management A) Medical treatment • The initial management with")
Treatment I) Non opera tive management A) Medical treatment • The initial management with administration of antibiotics according to bacterial sensitivity. • Precise microbiological identification. – In the event of a failure to isolate organisms, the choice of antibiotic should be based on the most likely etiological factor. • First line antibiotics would be a penicillin, aminoglycoside and metronidazole or a cephalosporin and metronidazole
 Closed percutaneous transhepatic abscess drainage (PTAD) • A simple one that is done")
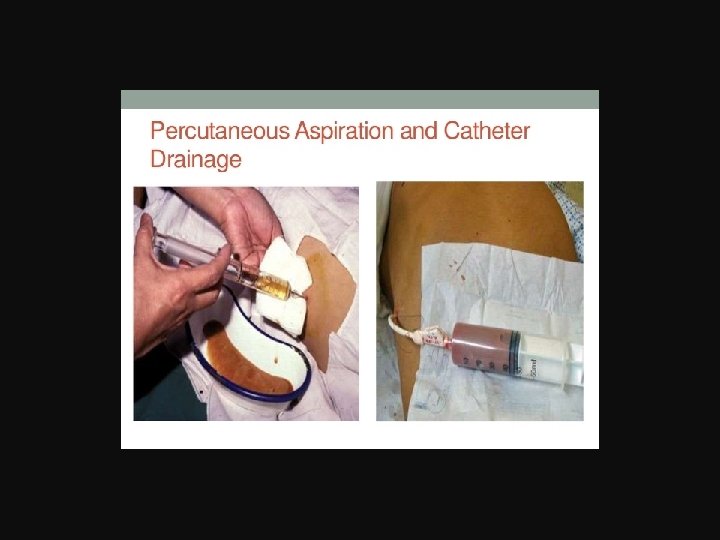
B) Closed percutaneous transhepatic abscess drainage (PTAD) • A simple one that is done under local anaesthesia. • The abscess is aspirated and then a tube drain is inserted. • It is as effective as open surgical drainage if the pyogenic abscess is single and unilocular. • Serial ultrasound examination to assess degree of resolution. • The reported success rate of PTAD averages 85%.
 Percutaneous aspiration • Success rates are somewhat similar to those for percutaneous catheter")
C) Percutaneous aspiration • Success rates are somewhat similar to those for percutaneous catheter drainage. • More than one aspiration is required. • In general, catheter drainage remains the treatment of choice, although a trial of a single aspiration is reasonable to consider.
 Endoscopic drainage • As the most frequent cause of hepatic abscess is biliary")
D) Endoscopic drainage • As the most frequent cause of hepatic abscess is biliary disease, flexible endoscopic treatment of these hepatic abscesses is practised in some centers. • This includes sphincterotomy and insertion of a nasobiliary catheter for continuous antibiotic lavage for 8 to 10 days.
 Operative management A) Surgical drainage • 1) Open surgical drainage – Indication: A.")
II) Operative management A) Surgical drainage • 1) Open surgical drainage – Indication: A. Patients who require surgical treatment of the primary pathology (e. g. , appendicitis). B. Failure of initial non operative management are: • 1. Unresolving jaundice. 2. multiloculation or multiplicity of the abscess. 3. Rupture on presentation. 4. Biliary communication. 5. Deterioration in the general condition of the patient. 6. Repeated episodes of septicaemia. 7. Failure of the abscess to decrease in size. 2) Laparoscopic surgical drainage: B) Liver resection: • This may be required for an infected hepatic malignancy, hepatolithiasis, or intrahepatic biliary stricture.

Amebic Hepatitis and Abscess

Incidence • It is common in tropical & subtropical countries • The low standards of hygiene, coupled with high humidity favour amoebiasis infestation. • Commoner than the pyogenic abscess. • It is more common in alcoholics and cirrhotic patients. • It is the commonest extra intestinal presentation of amoebiasis. • There is predominance in young males. • It represents 10 20% of liver abscess.
. • Source of infection: Colonic amoebiasis. •")
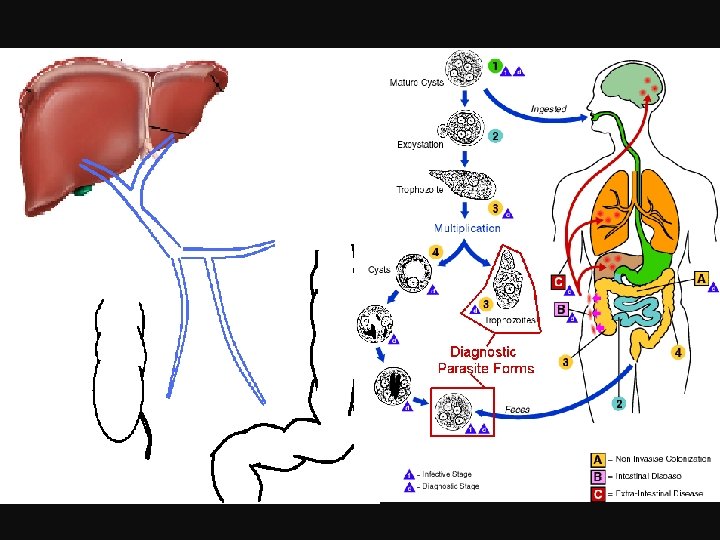
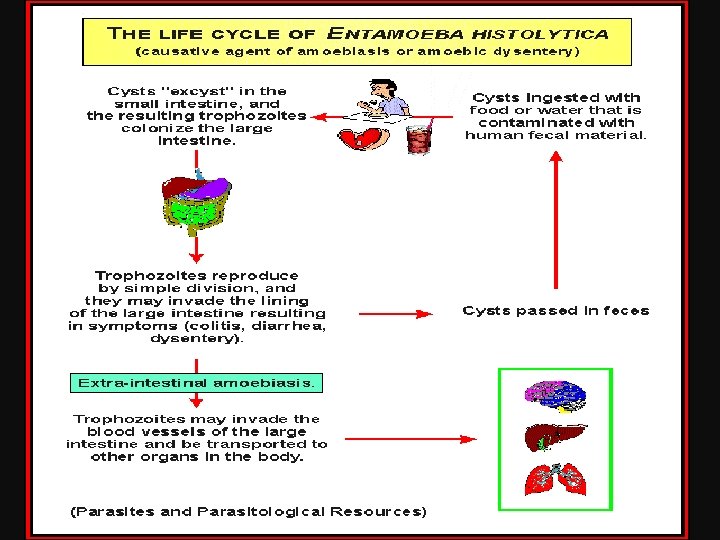
Etiology • Organisms: Entamoeba histolytica (protozoan parasite). • Source of infection: Colonic amoebiasis. • Route of infection: the portal circulation to the liver. Trophozoite of Entamoeba histolytica Cyst of Entamoeba histolytica

Pathology Pathogenesis

Pathology Stages A. Amebic Hepatitis B. Acute Amebic abscess C. Chronic Amebic Abscess

Anchovy sauce pus seen in amoebic liver abscess.

Clinical Picture • Type of Patient: Male more affected than female, 20 40 years old. • Onset: The condition usually develops soon after an attack of amebic dysentery. • Symptoms • General symptoms • Pain • A clear history, of an attack of dysentery is not always obtained. • Signs • General: • Local: • Chest :

Complications 1. Secondary infection: 2. Rupture: A. Upwards: B. Downwards: C. Outwards: D. Backward: E. In the blood stream: 3. Destruction of the liver with liver failure. 4. Calcification of a chronic liver abscess.
 laboratory • Stool examination for Entamoeba histolytica • Blood picture: anemia, eosinophilia")
Investigations A) laboratory • Stool examination for Entamoeba histolytica • Blood picture: anemia, eosinophilia & moderate leucocytosis. • Liver function tests: often normal. • Serological tests: complement fixation test & ELIZA. • Therapeutic test: B) Imaging • Liver scan: It may help to localize the abscess. – Ultrasonography, CT scanning & MRI – Isotope scanning • Radiography: chest X ray revealed C) Sigmoidoscopy:
 Liver conditions: a. Pyogenic abscess: b. Other causes of enlarged tender")
Differential Diagnosis (1) Liver conditions: a. Pyogenic abscess: b. Other causes of enlarged tender liver (2) Chest conditions: X ray will help to reach the diagnosis. a. Pulmonary tuberculosis. b. Empyema thoracis. c. Pneumothorax. d. Pleural effusion. (3) Acute abdomen: a. Acute cholecystitis. b. Subphrenic abscess: Difficult to differentiate. c. Right pyonephrosis. (4) Malaria: because of rigoris & fever. Blood film is diagnostic.
 Prophylactic: Treatment of amebic colitis. B) Curative: 1. Medical: a. Amebicidal drugs:")
Treatment A) Prophylactic: Treatment of amebic colitis. B) Curative: 1. Medical: a. Amebicidal drugs: a. Metronidazole (Flagyl): It is the treatment of choice. • 800 mg Tab. tid for 10 days. • inj. Metronidazole 500 mg IV tid for 10 days. N. B: Metronidazole not given in first trimester b. Tinidazole (Fasigyn): It is an effective drug. • 600 mg BD dose for 5 days • 2 gm (1*4) orally after lunch for 3 successive days. Broad spectrum antibiotics: it is used in conjunction with amebicidal drugs in 2 ry infected amebic liver abscess &if it ruptures.

c. Other drugs: 1. Injection dihydroemetine 1. 5 mg/kg/day IM for 5 days should be given under cardiac monitoring. 2. Chloroquine 250 mg BD given for 10 14 days. d. General measures: as bed rest, proper nutrition, analgesics & vitamins.

2. Aspiration: • Indications: § Lack of response to 3 days of metronidazole treatment. § Very large abscess. § Very toxic patient. § Secondary infected abscess • Technique: A) Percutaneous Needle Aspiration guided by ultrasound: B) Exploratory needle aspiration (closed drainage):

3. Percutaneous Drainage • Under U/S guidance pigtail catheter is placed into the abscess cavity percutaneously to drain the pus. • Catheter tube and abscess cavity has to be washed and irrigated at regular intervals with normal saline. • Disadvantages: It may fail if there is thick pus, multiloculated abscess, and multiple abscesses. • Complications: Procedure may cause bleeding and infection.

4. Open Drainage: Rarely needed. • Indications: § Presence of secondary infection. § If the abscess is pointing. § Case of rupture of abscess with peritonitis. § If aspiration is difficult because of multilocular abscess or the presence of thick pus. § Left lobe abscess. • Techniques: a. Posterior subpleural Approach: through 12 rib bed. b. Anterior Extraperitoneal approach:
 Treatment of complications: 1. Rupture into the lung and bronchus: 2. Rupture into")
C) Treatment of complications: 1. Rupture into the lung and bronchus: 2. Rupture into the pericardium:

Differences Between Amebic Liver Abscess and Pyogenic Liver Abscess Pyogenic liver abscess Amebic liver abscess • Leukocytosis <15 • Leukocytosis >15 • Serum antibodies to E. histolytica positive • Serum antibodies to E. histolytica negative • Aspirated pus shows no microorganisms • Aspirated pus shows bacteria • Jaundice uncommon (<8% of patients) • Jaundice common in presentation • Abnormal chest finding in physical examination uncommon • Abnormal chest findings in physical examination common • Younger patients (usually 20 to 40 yr) • Older patients (usually 60 to 70 yr) • Previously healthy • Presence of debilitating disease (cancer)

Cysts of the liver 1. Retention cysts. 2. Dermoid cyst 3. Traumatic cyst: Blood cyst. 4. Parasitic cyst: Hydatid cyst. 5. Polycystic liver 6. Degenerative cysts: Degenerating tumors.

Hydatid disease Cystic Echinococcosis

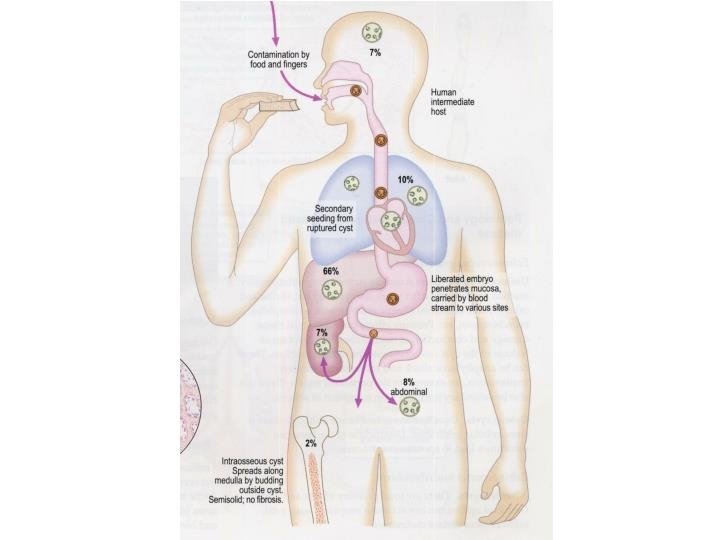
Etiology Incidence • Rare in Egypt. Common in cattle breeding countries like Algeria, Iraq, Libya, etc. Etiology • Organism: Tape worm Echinococcus Granulosus. • Definitive Host: Dogs • Intermediate Host: Sheep, cattle & man

Life cycle

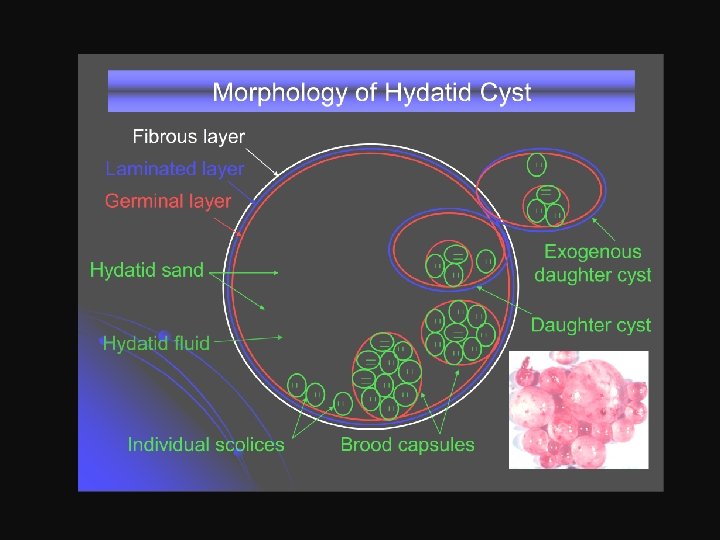
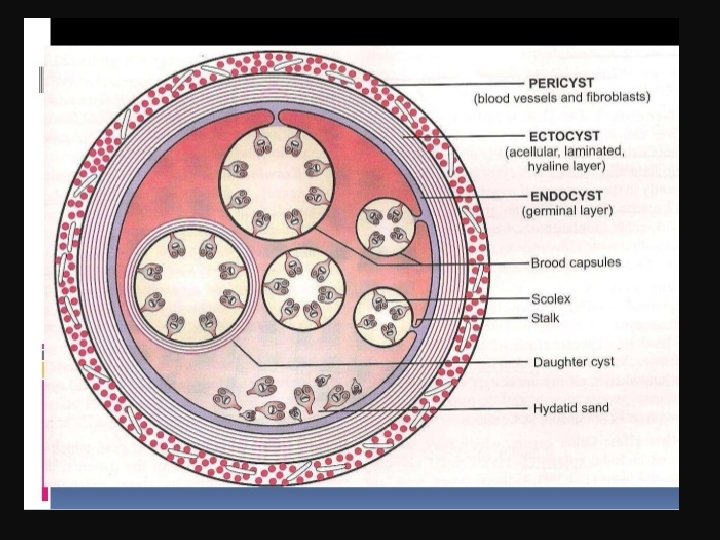
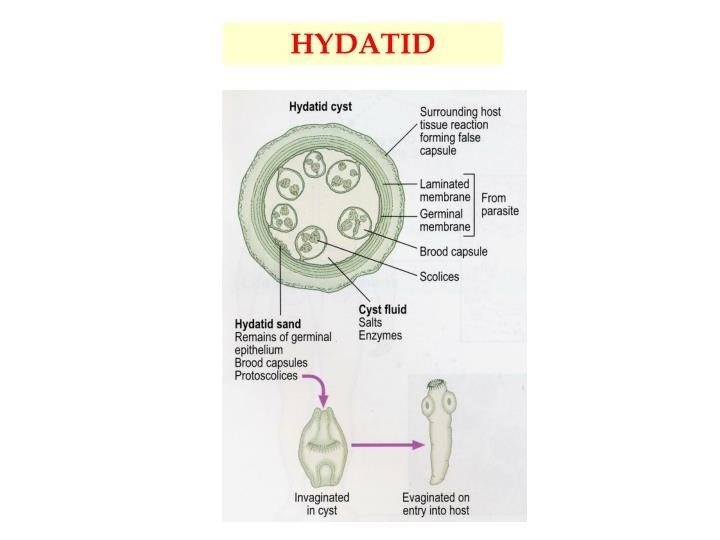
Pathology Gross picture: Microscopic picture: The hydatid cyst consists of 3 layers: • The adventitia (pseudocyst): • The laminated membrane (ectocyst): • The germinal layer (endocyst):

Clinical Picture 1. Symptomless for a long period 2. Intra abdominal mass 3. Hydatid thrill 4. Right upper quadrant pain. 5. Picture of complication.

Complications 1. Leakage of hydatid fluid. 2. Cracks in the laminated layer with satellite cysts around it. 3. Rupture of the cyst: Not uncommon, may be in: 1. Biliary tract: obstructive jaundice. 2. Peritoneal cavity leading to hydatidosis. 3. Thorax and pleural cavity leading to Empyema. 4. Blood stream leading to fatal anaphylactic shock or dissemination of hydatid cysts all over the body. 5. Renal pelvis causing hematuria & colic. 4. Secondary Infection leading to pyogenic liver abscess. 5. Pressure on surrounding: Liver, diaphragm & vessels. 6. Calcification and death of the cyst: This requires no treatment. 7. Liver failure

Multiple scolices removed from hydatid liver

Differential Diagnosis 1. Hepatoma. 2. Amoebic liver abscess. 3. Cystic disease of the liver.

Investigations 1. Blood picture: Eosinophilia. 2. Radiological evaluation: X ray, Ultrasonography, CT scan & MRI. 3. Direct assessment of E. granulosus and its viability 4. Serological tests. 1. Indirect hemagglutination reaction is of greater accuracy. 2. Complement fixation test: Best method of diagnosis. 3. ELIZA (Enzyme linked immunosorbent assay). 5. Casoni's test: 6. ERCP can show whether the cyst communicates with bile ducts or not.

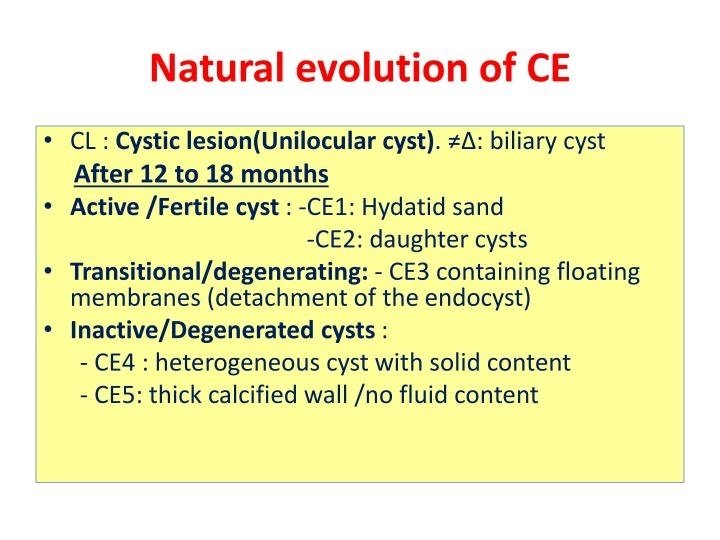
Investigations WHO-IWGE classification of hydatid cyst. CL: Cystic lesion; CE: Cystic Ecchinococcosis

Treatment • There is no “best” treatment option for CE. • Treatment indications are complex and are based on cyst characteristics, available medical/surgical expertise and equipment, and adherence of patients to long term monitoring. • Because treatment involves a variety of options and requires specific clinical experience, patients should be referred to recognized, reference and national/regional CE treatment centres, whenever available. • The available treatment include surgical, percutaneous and chemotherapy benzimidazoles (BMZ) based on WHO IWGE US classification of hydatid cyst
 Surgical treatment A. Indications: 1. Removal of large CE 2 CE 3 b")
B) Surgical treatment A. Indications: 1. Removal of large CE 2 CE 3 b cysts with multiple daughter vesicles. 2. Single liver cysts, situated superficially, that may rupture spontaneously or as a result of trauma when PT are not available. 3. Infected cysts, again, when PT are not available, 4. Cysts communicating with the biliary tree (as alternative to PT) 5. Cysts exerting pressure on adjacent vital organs.

B. Contraindications: 1. General contraindications for surgery apply. 2. Inactive asymptomatic cysts. 3. Difficult to access cysts. 4. Very small cysts.

C. Choice of surgical technique: The principles of surgery are: 1. Total removal of all infective components of the cysts. 2. Prevention of intraoperative protoscolex spillage. 3. Management of communication between cyst and adjacent structures. 4. Management of the residual cavity. 5. Minimize risks of operation.
 Total removal of all infective components of the cysts. A) Conservative surgery: •")
I) Total removal of all infective components of the cysts. A) Conservative surgery: • Marsupialization B) Radical surgery • Cystectomy • Pericystectomy • Liver resection
 Prevention of intra operative protoscolex spillage • This achieved by protection of peritoneal")
II) Prevention of intra operative protoscolex spillage • This achieved by protection of peritoneal tissues and organs with protoscolicide soaked green surgical drapes and injection of protoscolicide into the cyst before opening. • At present, 20% hypertonic saline is recommended. • The cyst is first aspirated and scolicidal agents (Hypertonic saline) is injected to make it three quarters full. • Hypertonic saline should be in contact with the germinal layer for at least 15 20 minutes to have effective scolicidal effect. • Its use should be avoided when communication between the cyst and the bile ducts is found, to avoid the risk of chemically induced sclerosing cholangitis. • Intraoperative dissemination of the mass in the peritoneum should be rinsed with hypertonic saline. Postoperative albendazole for 3 6 mo plus praziquantel for 7 d is recommended
 Management of cystobiliary communication 1. Suturing: using vicryl/PDS suture with T tube drain")
III) Management of cystobiliary communication 1. Suturing: using vicryl/PDS suture with T tube drain of bile duct. 2. Bipolar drainage – a drain is placed to cyst cavity and a T tube is placed into common bile duct. 3. Internal drainage procedures: like choledochojejunostomy; transduodenal sphincteroplasty; Roux – en Y cysto/intracystic hepatico jejunostomy; Roux – en – Y hepaticojejunostomy. 4. Reconstructive procedure like pericysto jejunostomy; bile duct repair. 5. ERCP sphincterotomy. 6. Liver resection. •
 Management of the residual cavity. • It is not advisable to drain the")
IV) Management of the residual cavity. • It is not advisable to drain the cavity except: – When infection is present. – When the contents of the cyst are bile stained, or – When there is uncertainty of its com plete removal. • Methods of residual cavaity management includes: 1. Omentoplasty 2. External drainage 3. Capitonnage: obliteration of the residual cavity by imbricating sutures from base of cavity to the edge of the cyst wall

An example of pericyctectomy material. An example of conservative surgery.

Benefits of surgery – Surgery may cure the patient completely but does not totally prevent recurrence. Risks of surgery – The risks include those associated with any surgical intervention, anaphylactic reactions, and secondary CE owing to spillage of viable parasite material. – Operative mortality varies from 0. 5% to 4%, but may be higher if surgical and medical facilities are inadequate.
 Percutaneous Treatment (PT) – This treatment was proposed in 1986 by the Tunisian")
B) Percutaneous Treatment (PT) – This treatment was proposed in 1986 by the Tunisian team that first used it in a prospective study. • PTs can broadly be divided into: 1. Those aiming at the destruction of the germinal layer (PAIR) 2. Those aiming at the evacuation of the entire endocyst (also known as Modified Catheterization Techniques).

A. PAIR A. Indications: It is indicated for 1. Inoperable patients 2. Refuse surgery 3. Relapse after surgery 4. Failure to respond to BMZ alone. Contraindications: PAIR is contraindicated for 1. CE 2 2. CE 3 b, 3. CE 4 4. CE 5, 5. Lung cysts. 6. Biliary fistulae contraindicate protoscolicide use.

C. Principle and technique: PAIR includes – Percutaneous puncture of cysts under US guidance and local anesthesia, – Aspiration of cyst fluid, – Injection of protoscolicide for 10– 15 min and – Re aspiration of the fluid. D. Choice of protoscolicides and prevention of protoscolex spillage – Protoscolicides used in PAIR are mainly 20% Na. Cl and 95% ethanol. – Transhepatic cyst puncture prevents peritoneal protoscolex spillage. – Prophylaxis with ABZ 4 h before and 1 month after PAIR is mandatory
.")
E. Benefits 1. PAIR confirms the diagnosis and removes parasitic material (Diagnostic and therapeutic). 2. Minimally invasive, 3. Less risky 4. Easy 5. Less expensive than surgery. F. Risks 1. Biliary fistulae after intracystic decompression, 2. Sclerosing cholangitis should the scolecidal agent reach the biliary vessels 3. Persistence of exo phytic daughter vesicles, 4. Anaphylactic reactions, 5. Secondary echinococcosis.

B. Catheterization techniques A. Indications: It is indicated for treatment of Types CE 2 and CE 3 a cysts and for post PAIR relapsing cysts B. Types 1. Percutaneous EVacuation Acuation of Cyst (PEVAC) 2. Modified catheterization technique (mocat) 3. Dilatable multi function trocar C. Principle and technique: • This technique involves inserting a 14 F catheter into the cystic cavity, which will allow the evacuation of the solid content (daughter vesicles and endocyst) by successive injections and aspirations of an isotonic saline solution. The drainage tube is removed when the drainage is less than 10 15 ml/24 hours.
 Medical (Antiparasitic drug treatment) A. Indications for drug therapy: 1. 4 30 days")
C) Medical (Antiparasitic drug treatment) A. Indications for drug therapy: 1. 4 30 days prior to intervention and to continue it for 1 month (albendazole) to 3 months (mebendazole) after the intervention. 2. Small (<5 cm) CE 1 and CE 3 a cysts in the liver and lung respond favorably to BMZ alone 3. Inoperable cysts. 4. Multiple or multiorgan cysts. 5. Recurrent hydatids. 6. Surgically unfit patients. 7. Cysts in lungs, bone, brain, eyes.
, 2. Cyst at risk of rupture.")
B. Contraindications: 1. Large cysts (over 10 cm), 2. Cyst at risk of rupture. 3. Honeycomb cysts (with septae). 4. Infected cysts. 5. Calcified cysts. 6. Pregnancy (ABZ is teratogenic).
 in divided doses for 3 6")
C. Drugs used: • Albendazole: (10 15 mg/kg/day) in divided doses for 3 6 months. • High dose mebendazole: (40 50 mg/kg/day) in three divided doses. – Both mebendazole and albendazole act against the germinal membrane of the hydatid cysts. – Mebendazole is comparable to that of albendazole, but requires higher doses for a longer period of time, due to its poor absorption. For the patients who can not use albendazole. • Praziquantel: (40 mg/kg/day) given as two divided doses. Alone or in combination with albendazole. It is more active against protoscoleces.

D. Benefits – BMZ can be used in patients of any age. However, there is little experience with children under 6 years old; – it is less limited by the patient’s status than surgery. – Average cure rate with standard dosage is 30%. – ABZ is more effective in young patients and for small CE 1 and CE 3 a cysts. – BMZ are less effective for CE 2 and CE 3 b D. Risks: – hepatotoxicity, – severe leucopenia and thrombocytopenia – alopecia – embryotoxicity and teratogenicity
 Watch and Wait approach • Some cysts do not require any treatment if")
D) Watch and Wait approach • Some cysts do not require any treatment if uncomplicated, namely, CE 4 and CE 5 (CL cysts should not be treated, until their parasitic nature has been proven).

Stage Size First option treatment Alternative treatment CE 1 CE 3 a Small Medium Large PAIR + ABZ (1 month) Mo. Cat + ABZ (1 month) CE 2 CE 3 b Small Medium Large CE 4 Any diameter ABZ for 6 months Surgical treatment + ABZ (1 6 months) "Watch and Wait" CE 5 Any diameter "Watch and Wait" Complicated cyst Any diameter Surgical treatment + ABZ (6 months) ± Interventional endoscopy in case of rupture in the biliary tract Surgical treatment in case of rupture Percutaneous drainage in case of infection + ABZ (1 month) ABZ for 6 months Refusal of intervention contraindication of invasive treatment Mo. Cat + ABZ (1 month) "Watch and Wait"

- Slides: 79