Complex care frailty in Camden 2016 Dr Stuart

















- Slides: 19
Complex care & frailty in Camden 2016 Dr Stuart Mackay-Thomas GP Partner Hampstead Group Practice Clinical lead Complex Care and Frailty, Dementia and Care Homes Camden CCG
Planned care LES and case studies Planned care LES for frailty requirements Available services for frail / complex care patients Case studies and discussion
Planned care LES requirements Practices should regularly review and discuss patients on their lists to identify patients who are frail and suitable for case management. Practices should use the risk stratification tool recommended by the CCG - currently the QAdmission score but this may change in future.
Planned care LES requirements Where a patient has been identified as “frail”, the practice should enter the patient onto the practice’s Frailty Register (FR) using Read Code EMISNQON 5 (“On frailty register”).
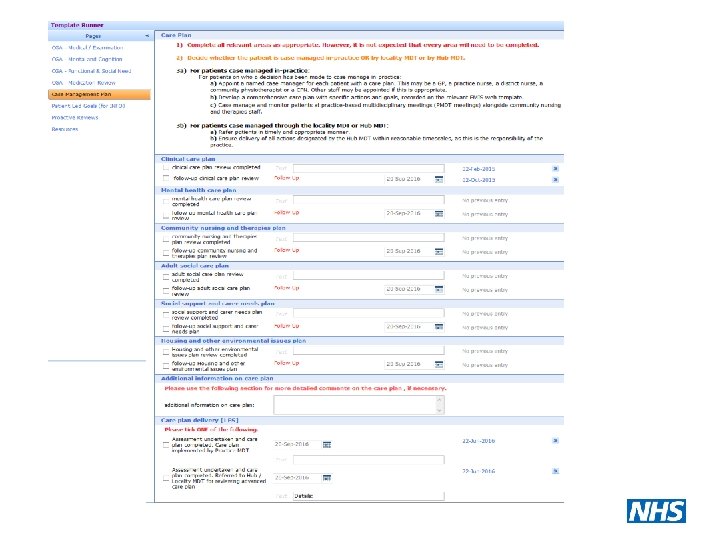
Planned care LES requirements Once the patient has been entered on the FR the practice should complete a comprehensive geriatric assessment (CGA) using the relevant clinical template. The CGA should be undertaken prior to or at the same time as the care planning appointment.
Planned care LES frailty • Decide which multidisciplinary forum the patient will be case managed under. • Appoint a named case manager for each patient with a care plan. • Case manage patients via the appropriate multidisciplinary team with regular follow up of care plans and re-evaluation of patient’s status according to the PC LES specification appendices, July 2016 • Undertake proactive home visiting of housebound patients on the FR. • Where patients are case managed through the Hub or Locality MDTs, ensure delivery of all actions designated by the Hub MDT for the practice.
Frailty levels and delivery of care Mild frailty or needs Practice MDT Moderate frailty / moderate complex needs Locality MDT Severe frailty / complex needs Borough-wide/ “Hub” MDT
Hub and locality locations South Camden Centre for Health Hampstead Group Practice Keats Group Practice West Hampstead Medical Centre Kentish Town Health Centre
Case study 1 An 80 year old female with ischaemic heart disease. She lives on her own, and is independent in personal ADLs. She is able to go out independently, travel on public transport and does her own shopping/manages her finances. The family help with heavy domestic ADLs. She has developed urge incontinence over the last few months, and is finding it difficult to manage, especially when outside. She has also noticed that her memory is causing problems at times; she has forgotten her medication and forgotten to pay the bills once/twice.
Case study 2 An 82 year old female with polymyalgia rheumatica and diet-controlled type 2 diabetes. She is able to mobilise outdoors with the help of one carer and a frame. There are some mild memory problems being noticed by the carers, and she was brought home from the supermarket once having got lost. She is now beginning to develop increasing problems with indoor mobility and has nearly fallen twice with the carers present.
Case study 3 A 90 year old man with severe heart failure, recurrent UTIs, and moderate dementia. Lives in flat with qds care (needs assistance with personal/domestic ADLs/assistance with transfers); children live outside London. Has had recurrent admissions with decompensated heart failure, delirium/falls. Has now developed a sacral grade 3 pressure sore, and is developing challenging behavioural problems. Also has oropharyngeal dysphagia, with poor oral intake, is refusing food and has a very poor nutritional state. The family are increasingly concerned about his general decline, and his ability to manage at home.
Discussion Please discuss the cases and consider: • who might best assess the patient • what interventions / care plan might help • what level of frailty the patient might be managed at
Complex/ Severely Frail Patients with the most complex level of need, requiring multilevel expert disciplinary intervention. The patients might be severely frail, and at risk to themselves or others due to their physical and mental health.
Moderately Frail Patients with a number of long-term conditions who require assessment, intervention and co-ordination by more than two disciplines. They might have moderate frailty, with a mixture of men-tal and physical problems.
Mildly Frail Usually older people needing collaborative working between disciplines for example medicine and district nursing. They might have one or two long term conditions including mental health problems, but are likely to be at low risk to themselves or others. They might be mildly frail.
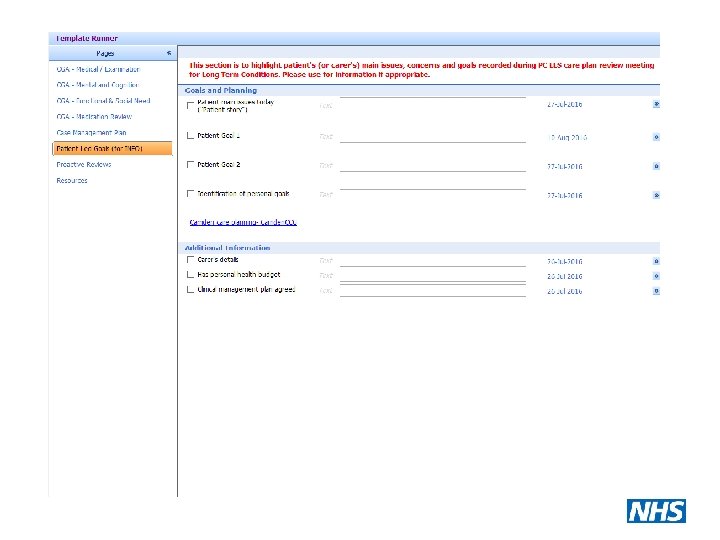
What is a care plan? National Coalition on Care Co-ordination – “. . . a person-centred, assessmentbased interdisciplinary approach. . . ” National Voices say a care plan isn’t – “ “A document, drawn up by a professional and given to a person, without any discussion with them. ”
Care planning • • Medical Nursing Mental health Social work including re-ablement / selfcare • Drug and alcohol use • Personal care needs