Dr Ahmed Refaey FRCR Consultant Radiologist Riyadh Military
















































- Slides: 55
Dr. Ahmed Refaey , FRCR Consultant Radiologist Riyadh Military Hospital
Format of the lecture Anatomy Pathogenesis Imaging techniques Scanning protocoles Classification Examples
ANATOMY
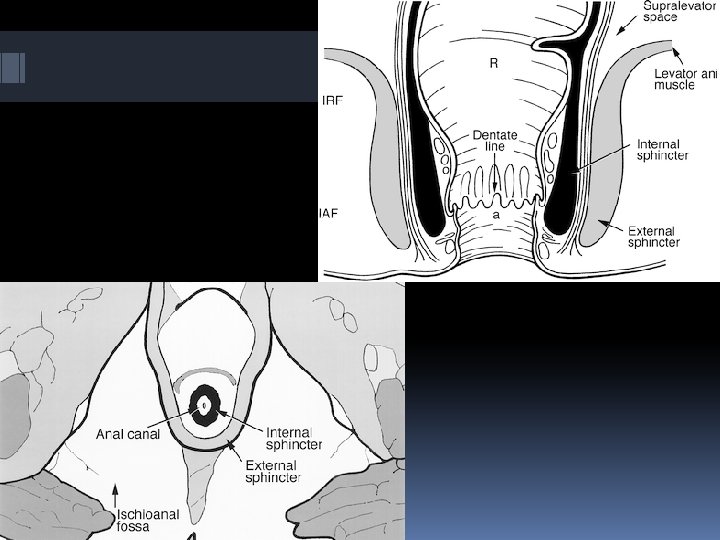
Anatomy Anatomical canal : - extends from perineal skin to dentate line Surgical canal : - extends from perineal skin to anorectal ring ( 1 -1. 5 cm abov e dentate line ) - total length 4 -5 cm
Anal sphincter comprised of 3 layers Internal sphincter - continuance of circular smooth muscle of rectum, involuntary, contracts at rest & relaxes at defecation Intersphincteric space External sphincter - voluntary striated muscle , continuous cranially with puborectal muscle &levator ani
Puborectal muscle has its origin on both sides of the symphysis pubis, forming a sling around the anorectum
The puborectal muscle is contracted at rest and accounts for the 8 O 0 angulation of the anorectal junction. It relaxes during defecation
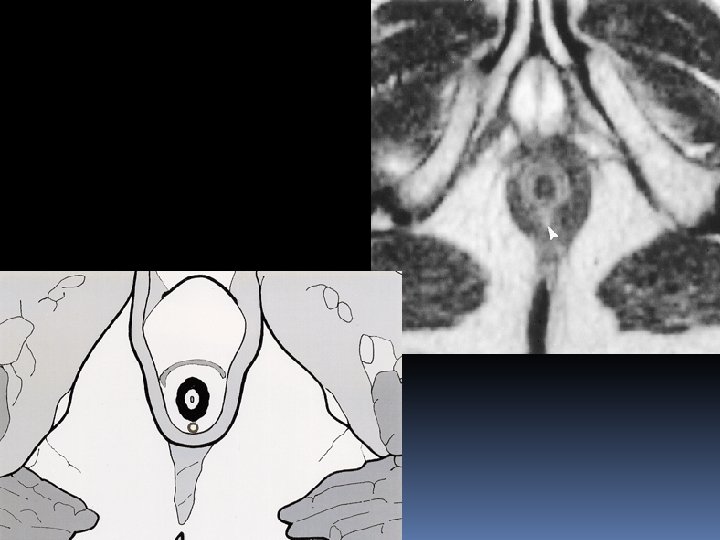
On axial and coronal MR images , the different layers of anal sphincter and the surrounding structures can be displayed perfectly
Coronal Axial
PATHOGENESIS
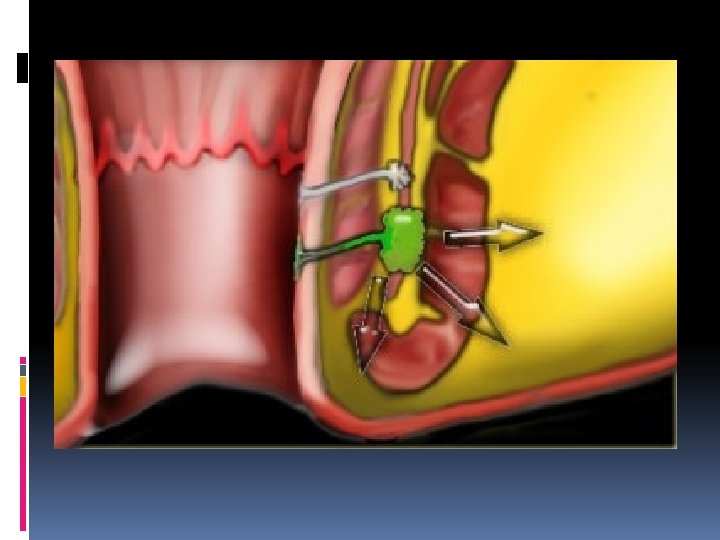
Perianal fistula Abnormal connection between the epithilialised surface of the anal canal and the skin.
Causes 1 ry - obstruction of anal gland which leads to stasis & infection with abscess & fistula formation ( most common cause ) 2 ry - iatrogenic ( post hemorrhoiedal surgury ) - inflammatory bowel dis. ( crohn’s disease ) - infections ( viral , fungal or TB ) - malignancy
IMAGING TECHNIQUES
Imaging techniques Fistulography Endosonography CT MRI
Perianal fistulography
Anal endosonography
CT
MRI protocol T 1 W &T 2 W fse axial and coronal T 2 W with fat sat T 1 W + CM FOV 200
T 2 W ----- anatomy T 2 W with fat sat ---- fistula
The anal clock P: anterior perineum n: natal cleft
The anal clock The surgeon’s view of the perianal region when the patient is in the supine lithotomy position , corresponds to the orientation of axial MRI of the perianal region
Reporting Position of the mucosal opening on axial images using anal clock Distance of mucosal defect to perianal skin on coronal images 2 ry fistulas or abscess
CLASSIFICATION
Classification Parks classification 1 - intersphincteric 2 - transsphincteric 3 - extrasphincterisc 4 -suprasphincteric Intersphincteric & transsphincteric are the most common Intersphincteric --> 70 % Transsphincteric -->20%
St. James university hospital classification MR imaging Grading of perianal fistulas
MRI Grading of perianal fistulas Grade 1 : simple linear intersphincteric fistula Grade 2 : intersphincteric fistula with abscess or 2 ry track Grade 3 : transsphincteric fistula Grade 4: transsphinteric fistula with abscess or 2 ry track within ischeorectal fossa Grade 5 : supralevator & translevator fistula
Grade 1 : simple linear intersphincteric fistula
Intersphincteric fistula Axial T 2 W with and without fat saturation The intersphincteric fistula located at 6 o’clock
Intersphincteric fistula
Perianal fistula with an abscess
Grade 2 : intersphincteric fistula with abscess or 2 ry track
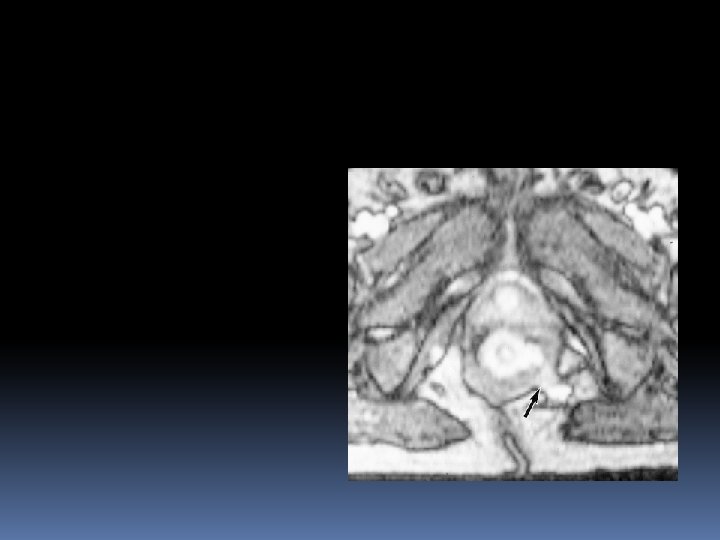
Grade 3 : transspincteric fistula
Transsphincteric fistula The defect through internal & external sphincter at 6 o’clock is clearly visible
Transsphincteric fistula at 11 o’clock
Grade 4: transsphinteric fistula with abscess or 2 ry track within ischeorectal fossa
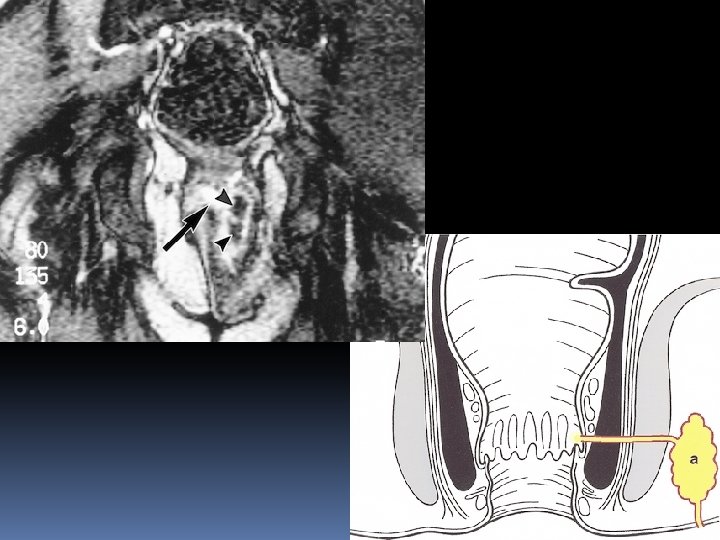
Grade 5 : supralevator & translevator fistula
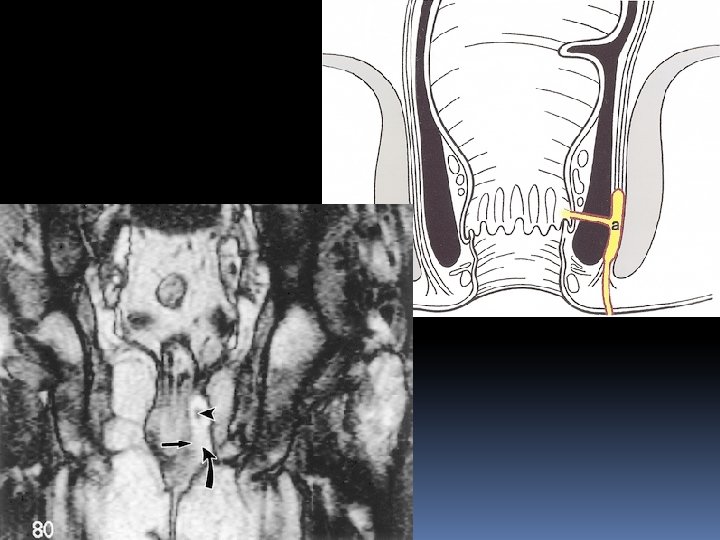
Suprasphincteric fistula Two tracts in ischeorectal region The right sided tract runs over the puborectal muscle (asterisc) & the mucosal opening lies at the level of dentate line (black arrow)
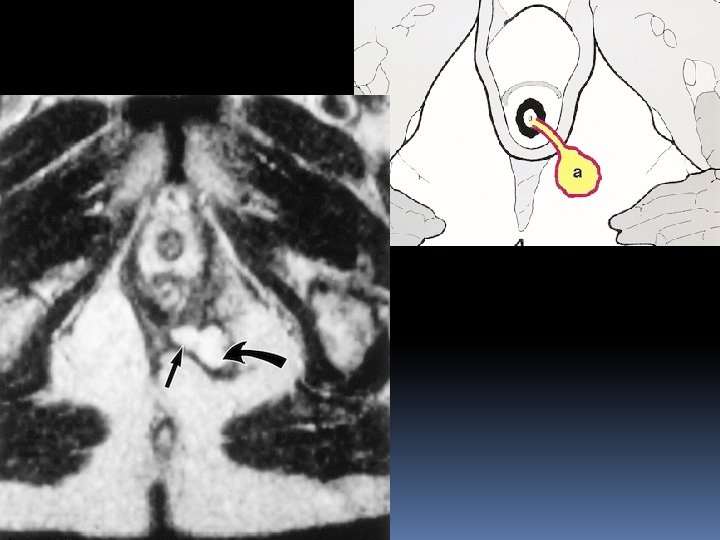
Extrasphincteric fistula A small abscess in left ischeoanal fossa , the fistula runs through levator ani , it is therefore above the sphincter complex and extrasphincteric
Complex fistula 2 tracts in left buttock form single tract The fistula breaks through the external sphincter In intersphincteric space it divides again into 2 tracts One ends blindly in the intersphincteric space The other breaks through the internal sphincter with mucosal defect at 1 o’clock
Differential diagnosis
Pielonidal sinus Small abscess just above the nates No relation with sphincter complex
Proctitis No fistula was seen Diffuse thickening of rectal mucosa due to proctitis
Ischiorectal space abscess An abscess in ischiorectal space with no connection to the sphincter complex
REFERENCES
Goodsall DH, Miles WE. Diseases of the anus and rectum. London, England: Longmans, Green, 1900. ↵ Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. Br J Surg 1976; 63: 1 -12. ↵ Halligan S. Imaging fistula-in-ano. Clin Radiol 1998; 53: 8595. ↵ Kuijpers HC, Schulpen T. Fistulography for fistula-in-ano: is it useful? Dis Colon Rectum 1985; 28: 103 -104. ↵ Weisman RI, Orsay CP, Pearl RK, et al. The role of fistulography in fistula-in-ano: report of 5 cases. Dis Colon Rectum 1991; 34: 181 -184. ↵ Choen S, Burnett S, Bartram CI, Nicholls RJ. Comparison between anal endosonography and digital examination in the evaluation of anal fistulae. Br J Surg 1991; 78: 445 -447.
↵ Guillaumin E, Jeffrey RB, Shea WJ, et al. Perirectal inflammatory disease: CT findings. Radiology 1986; 161: 153 -157. ↵ Yousem DM, Fishman EK, Jones B. Crohn disease: perirectal and perianal findings at CT. Radiology 1988; 167: 331 -334. ↵ Barker PG, Lunniss PJ, Armstrong P, Reznek RH, Cottam K, Phillips RK. Magnetic resonance imaging of fistula-in-ano: technique, interpretation, and accuracy. Clin Radiol 1994; 49: 7 -13. ↵ Spencer JA, Ward J, Beckingham IJ, Adams C, Ambrose NS. Dynamic contrast-enhanced MR imaging of perianal fistulas. AJR Am J Roentgenol 1996; 167: 735 -741. ↵ Haggett PJ, Moore NM, Shearman JD, Travis SPL, Jewell DP, Mortensen NJ. Pelvic and perianal complications of Crohn's disease: assessment using magnetic resonance imaging. Gut 1995; 36: 407410.
Koelbel G, Schmeidl U, Majer MC, et al. Diagnosis of fistulae and sinus tracts in patients with Crohn's disease: value of MR imaging. AJR Am J Roentgenol 1989; 152: 999 -1003. Myhr GE, Myrvold HE, Nilsen G, Thoresen JE, Rinck PA. Perianal fistulas: use of MR imaging for diagnosis. Radiology 1994; 191: 545 -549. ↵ Hussain SM, Stoker J, Schouten WR, Hop WCJ, Lameris JS. Fistula-inano: endoanal sonography versus endoanal MR imaging in classification. Radiology 1996; 200: 475 -481. ↵ Halligan S, Bartram CI. MR imaging of fistula-in-ano: are endoanal coils the gold standard? AJR Am J Roentgenol 1998; 171: 407 -412. ↵ Spencer JA, Chapple K, Wilson D, Ward J, Windsor ACJ, Ambrose NS. Outcome after surgery for perianal fistula: predictive value of MR imaging. AJR Am J Roentgenol 1998;