SALMONELL A Pathogenesis PATHOGENICITY OF SALMONELLAE Clinical syndromes













")
 is about 1 000 to 1 000 bacilli")
 MESENTERIC LYMPHNODES PHAGOCYTOSIS BLOOD STREAM")

















- Slides: 34
SALMONELL A Pathogenesis. .
PATHOGENICITY OF SALMONELLAE Clinical syndromes caused by Salmonellae in human beings: A. Enteric fever B. Gastroenteritis (food poisoning) C. Salmonella septicemia
ENTERIC FEVER The term ENTERIC FEVER includes 1. TYPHOID FEVER – caused by S typhi 2. PARATYPHOID FEVER – caused by S paratyphi A, B & C
CONTD. . Enteric fever is endemic in all over India. With a proportion of TYPHOID to PARATYPHOID A about 10 : 1. Paratyphoid B is rare and Paratyphoid C is very rare.
TYPHOID FEVER Typhoid fever, also known as typhoid Other names: abdominal typhus, infantile remittant fever, slow fever, nervous fever, pythogenic fever, etc.
CONTD. . Typhos in Greek means, smoke and typhus fever got its name from smoke that was believed to cause it. Typhoid means typhus-like and thus the name given to this disease. The term Typhoid was given by Louis (1829) to distinguish it from typhus fever. Eberth described the typhoid bacillus in spleen sections and mesenteric lymph nodes from a patient who died from typhoid and Gaffky isolated it in pure cultures.
SALMONE LLA Electron microscopy
EPIDEMIOLOGY Epidemiological types Endemic Epidemic
WORLD WIDE DISTRIBUTION
CONTD. . Source : Case of Typhoid or carriers in frequent. Infective material : Contaminated food or water. Route of infection : Ingestion of contaminated food or water.
CARRIER STATE. . CARRIERS are more important in the transmission of the disease. Types of carriers: 1. Convalescent carriers 2. Temporary carriers 3. Chronic carriers Convalescent carriers shed bacilli in feces for 3 WEEKS to 3 MONTHS after clinical cure. Temporary carriers shed bacilli for more than 3 MONTHS but less than A YEAR. Chronic carriers shed bacilli for over A YEAR.
CONTD. . 2 -4 % of patients become Chronic carriers, esp. women over 40 yrs. Food handlers or cooks that become carriers are particularly dangerous. The best known example was Mary Mallon, named for nick as TYPHOID MARY. She caused at least 7 outbreaks in 15 yrs affecting over 200 people.
MARY MALLON in a 1909 newspaper illustration
BACILLI PERSIST IN GALL BLADDER OR KIDNEY ARE SHRED OUT Carriers Fecal (Gall bladder) Urinary (Kidney)
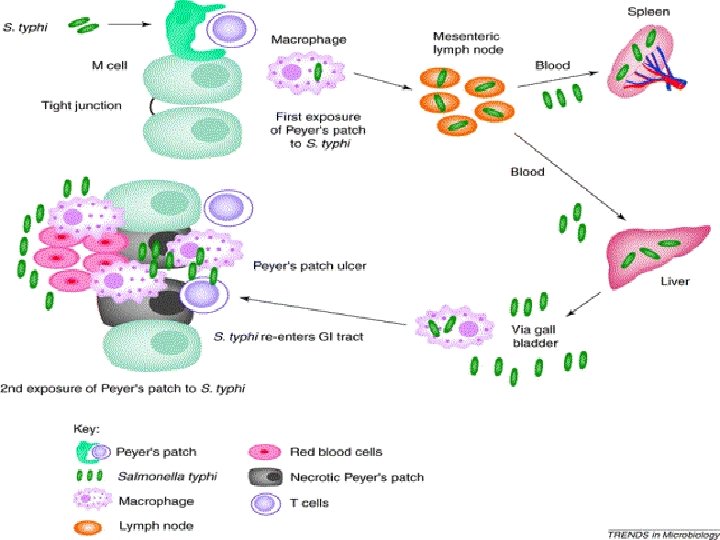
PATHOGENESIS Median Infective Dose (ID 50) is about 1 000 to 1 000 bacilli in human volunteers. The course of organism in the body is as follows.
BACILLI MICRO VILLI OF ILEUM PENETRATION THORACIC DUCT (Multiplication) MESENTERIC LYMPHNODES PHAGOCYTOSIS BLOOD STREAM (Transient Bacteremia) LIVER, G. B. , SPLEEN, B. M. , L. N. , LUNGS. MASSIVE BACTEREMIA
CLINICAL COURSE. . Incubation period is usually 7 -14 days, but may range 3 -56 days according to dose of infection. Clinical course: From Mild Undifferentiated Pyrexia (AMBULANT TYPHOID) Rapidly fatal disease
CLINICAL FEATURES. . Gradual Onset of head ache malaise anorexia Typical features: Step ladder pyrexia Relative bradycardia Toxemia
CONTD. . A soft, palpable spleen is a constant finding Hepatomegaly is also common Rose spots that fade on pressure appear on skin during 2 nd or 3 rd week.
ROSE SPOTS
Bile is a good culture medium for the bacillus, it multiplies abundantly in GALL BLADDER involves the INTESTINES PAYERS PATCHES LYMPHOID FOLLICLES
INFLAMMED PAYERS PATCHES NECROSIS SLOUGH OFF TYPHOID ULCERS
ULCERATION OF BOWEL HEMORRHAGE PERFORATION
Ingestion of organisms CAUSATION Colonization of lower intestine Mucosal invasion Acute inflammation Activation of Adenyl cyclase Fluid production Diarrhea
COMPLICATIONS OF THE DISEASE Intestinal perforation Hemorrhage Circulatory collapse Bronchitis or Bronchopneumonia is always found. Psychoses Meningitis Cholecystitis Arthritis Abscesses
CONTD. . Periostitis Nephritis Hemolytic anemia Venous thromboses Peripheral neuritis Osteomyelitis is rare sequel.
CONVALESCENCE & RELAPSE Convalescence is slow In 5 -10% of cases relapse occurs during convalscence Relapse rate is higher in patients treated early with Chloramphenicol.
PARATYPHOID FEVER Resembles typhoid fever but is generally milder Caused by S. paratyphi A and B, rarely by S. paratyphi C which is often associated with frank septicemia in supporative complications.
SALMONELLA GASTROENTERITIS Food poisoning. Zoonotic disease. Caused by any Salmonella except S. typhi. Pathogenic Species: 1. S typhimurium (most common) 2. S enteritidis
PATHOGENESIS Source: Poultry, Meat, Milk and its products, esp. , Eggs and its products (as the bacteria can enter through the shell if eggs are contaminated and grow inside), uncooked vegetables. Route: Ingestion Gastroenteritis may occur without food poisoning as in cross infection in hospitals.
CLINICALLY. . Short incubation period of 24 hrs or less. Featured by Diarrhea, Vomiting, Abdominal pain, Fever. Diarrhea: May vary from one or more loose stools to an acute Cholera like Usually subsides in 2 -4 days resembles and dysentery.
SALMONELLA SEPTICEMIA Caused by: S choleraesuis Focal supporative lesions: Osteomyelitiss, Deep abscesses, Endocarditis, Pneumonia, Meningitis.