Management of Peritoneal Carcinomatosis in Colorectal Cancer Dr

 ¡ High incidence with significant morbidity and mortality ¡ Metastasis on")
 ¡ “Death sentence” ¡ Median survival: 6 – 9 months ¡")




 Peritoneal Cancer Index (PCI) Completeness")

 ¡ Summary of lesion size and distribution of lesions ¡")




 ¡ Intraoperative/ early postoperative – no")








 average survival from 32.")
: 97 -102,")









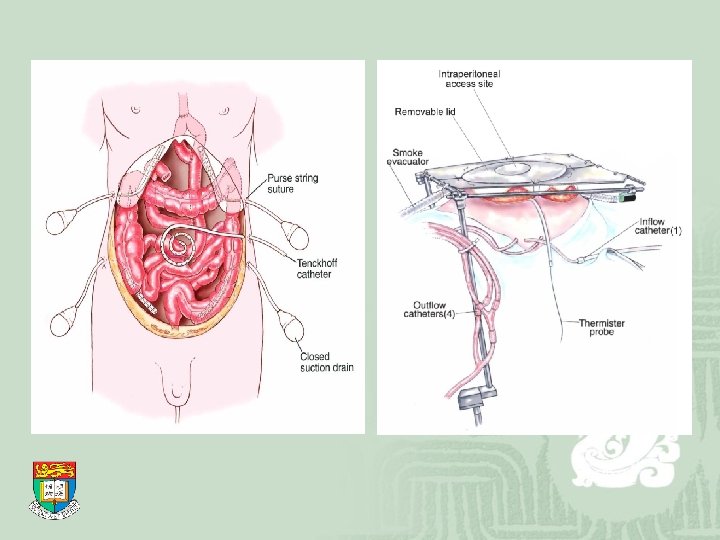
 ¡ Setting up: After completion of cytoreductive surgery Catheters are")



- Slides: 39
Management of Peritoneal Carcinomatosis in Colorectal Cancer Dr. Chan Kwan Kit Queen Mary Hospital
Colorectal Cancer (CRC) ¡ High incidence with significant morbidity and mortality ¡ Metastasis on presentation or as recurrent disease commonly encountered ¡ Liver and peritoneal surface are the most frequent sites of metastasis ¡ Treatment of colorectal liver metastases well established
Peritoneal Carcinomatosis (PC) ¡ “Death sentence” ¡ Median survival: 6 – 9 months ¡ Treatment of palliative intent systemic chemotherapy symptomatic relief emergency operation for complications e. g. intestinal obstruction/ perforation Chu DZ et al. Cancer 1989; 63: 364– 7 Sadeghi B et al. Cancer 2000; 88: 358 -63 Jayne DG et al. British Journal of Surgery 2002; 89: 1545– 50
Pathophysiology of PC ¡ Consequence of full thickness invasion of bowel wall by invasive carcinoma ¡ “Iatrogenic” during primary surgery dissected lymphatics/ bowel lumen blood spillage from the surgical field
Breakthrough? ¡ Jayne et al. : 58% of all patients with synchronous PC had no other systemic metastasis ¡ Sugarbaker et al. : peritoneal cavity is the only metastatic site in 25% of patients with recurrent CRC Hypothesis: PC as a locoregional disease still susceptible to treatment of curative intent
Dr Paul H Sugarbaker ¡ Washington Hospital Centre ¡ Pioneer of the combined treatment ¡ “Sugarbaker’s protocol” Cytoreductive surgery Perioperative intraperitoneal chemotherapy
Cytoreductive Surgery ¡ Removal of macroscopic tumour on visceral and parietal peritoneum ¡ Significant involvement of visceral peritoneum may necessitate organ resections ¡ Significant involvement of parietal peritoneum may necessitate formal peritonectomy procedures
Cytoreductive Surgery ¡ Prognostic indicators: Prior Surgical Score (PSS) Peritoneal Cancer Index (PCI) Completeness of cytoreduction score (CCS)
Prior Surgical Score ¡ PSS-0: biopsy only ¡ PSS-1: 1 region ¡ PSS-2: 2 -5 regions ¡ PSS-3: >5 regions Higher PSS associated with reduced survival
Peritoneal Cancer Index (PCI) ¡ Summary of lesion size and distribution of lesions ¡ Correlates with outcome for peritoneal metastases in CRC
0 -39 Sugarbaker et al. Cancer therapeutics 1998; 1: 213 -325
Peritoneal Cancer Index ¡ Sugarbaker in 1999: PCI < 10: 50% five-year survival PCI 11 -20: 20% five-year survival PCI > 20: 0% five-year survival Pestieau SR, Sugerbaker PH. Dis Colon Rectum 2000; 43: 1341– 1348 ¡ Not applicable when tumour deposit at crucial anatomical site not amenable for resection
Completeness of Cytoreduction Score ¡ Size of persisting tumour after cytoreduction CCS-0: no visible tumour CCS-1: tumours <2. 5 mm CCS-2: tumours 2. 5 mm - 2. 5 cm CCS-3: tumours >2. 5 cm Principle prognostic indicator – helps intraoperative decision making
Role of diagnostic laparoscopy ¡ Allows more accurate “staging” with minimal surgical trauma ¡ Reliable prediction of cytoreduction index
Perioperative Intraperitoneal Chemotherapy ¡ Hyperthermic intraperitoneal chemotherapy (HIPEC) ¡ Intraoperative/ early postoperative – no standard protocol as yet ¡ Aim: eradication of microscopic residual disease for curative intent
HIPEC - advantages ¡ Intraperitoneal Increases exposure of tumour to pharmacologically active molecules ¡ Hyperthermia enhances cytotoxicity improves drug penetration heat has anti-tumour effect itself
HIPEC - advantages ¡ Large volume removes tissue debris and blood products ¡ Diminishes the promotion of tumour growth associated with wound healing process through elimination of platelets/ neutrophils/ monocytes
Surgeon manipulates all viscera to minimize adherence of peritoneal surfaces and allow uniform distribution of drugs
¡ Duration: 30 -90 minutes ¡ Continuous irrigation ¡ Temperature monitoring at inflow catheters and within peritoneal cavity maintained at 42. 5ºC
Chemotherapeutic agent ¡ Varies with centres e. g. mitomycin C, oxaliplatin ¡ Mitomycin C being the commonest choice – large molecular weight substance confining to peritoneal cavity for long time periods
Results – the risks ¡ Mortality 2 -10% and morbidity 25 -45%, predominantly determined by surgeryrelated factors extent of surgery number of anastomoses volume of blood loss
Results – the risks ¡ Common complication: bowel perforation anastomotic leakage prolonged ileus/ bowel fistulation/ intraabdominal bleeding/ pancreatitis/ haematological toxicity
Results - survival benefit? ¡ Glehen et al. : multi-institutional retrospective study median survival 19. 2 months, irrespective of cytoreduction extent 19% 5 -year survival Glehen et al. J Clin Oncol 2004; 22: 3284 -92 ¡ Elias et al. & Verwaal VJ et al. : the only two randomized, prospective studies Elias: 60% survival at two years Verwaal: median survival 22. 2 months Elias et al. Ann Surg Oncol 2004; 11: 518 -21 Verwaal VJ et al. Ann Surg Oncol 2005; 12: 65 -71
Results - survival benefit? ¡ With complete macroscopic cytoreduction (CCS-0) average survival from 32. 4 – 60 months Glehen et al. J Clin Oncol 2004; 22: 3284 -92 Elias et al. Ann Surg Oncol 2004; 11: 518 -21 Verwaal VJ et al. Ann Surg Oncol 2005; 12: 65 -71 Sugarbaker PH. Tech Coloproctol 2005; 9: 95 -103
Gomez Patilla A. et al. Rev Esp Enferm Dig 2009 Feb; 101(2): 97 -102, 103 -6
Patient selection ¡ No survival benefit for patients with synchronous metastases to other organs ¡ Aggressive treatment of large volume, high grade cancer is unlikely to translate into long -term benefit
Prognostic factors ¡ Peritoneal cancer index ¡ Completeness of cytoreduction ¡ Presence of lymph node involvement ¡ Age and performance status
Validation? ¡ Reported trials are of significant heterogeneity ¡ No standard protocol e. g. timing of chemotherapy/ use of hyperthermia ¡ Only two randomized trials published – relatively small scale
Conclusion ¡ Peritoneal carcinomatosis from colorectal origin carries dismal prognosis with conventional treatment ¡ “Combined treatment” - cytoreductive surgery with intraperitoneal chemotherapy may represent a new option of care in peritoneal-only metastatic disease
Conclusion ¡ Significant procedural morbidity/ mortality mandates careful selection ¡ Large scale, randomized, prospective studies needed for clarification of the role of this aggressive approach
HIPEC ¡ Disadvantages Removal of white cells due to chemotherapy and heat leaves the patient vulnerable to intraabdominal infection limited tissue penetration 3 -5 mm
Postoperative care ¡ Expected prolonged bowel rest prolonged ileus due to extensive surgery allowing more time for healing total parenteral nutrition
Peritonectomy ¡ Peritoneum divided into 6 parts greater omentectomy and splenectomy left upper quadrant peritonectomy right upper quadrant peritonectomy lesser omentectomy and cholecystectomy pelvic peritonectomy and resection of rectosigmoid colon antrectomy/ gastrectomy
Hyperthermic intraperitoneal chemotherapy (HIPEC) ¡ Setting up: After completion of cytoreductive surgery Catheters are inserted to dependent positions Temperatures at the inflow/ outflow/ intraperitoneal cavity continuously monitored Temporary abdominal skin closure Intraperitoneal temperature maintained 42. 5℃
Intraoperative chemotherapy ¡ Reconstructive part of surgery follows ¡ No anastomosis is constructed until after the intraoperative chemotherapy perfusion is completed
Early postoperative intraperitoneal chemotherapy ¡ 5 -fluorouracil is utilized usually ¡ Commenced on day 1 after operation Infusion via Tenckhoff catheter Chemotherapy agent dwells in the abdomen for 23 hours and drain for 1 hour Duration: 4 -5 days
Counter-argument ¡ Peritoneal carcinomatosis with low PCI and CCS may represent more favourable tumour biology ¡ Opinions vary widely and no consensus could be reached ¡ Genetics study? Molecular features of tumour?