Le allergie alimentari multiple Giampaolo Ricci Universit di




")







. The no allergic disease. The estimated")


 MONO-PANALLERGEN Bet v 1 MULTI-PANALLERGEN Pru p 3 NO")










- Slides: 45
Le allergie alimentari multiple Giampaolo Ricci Università di Bologna
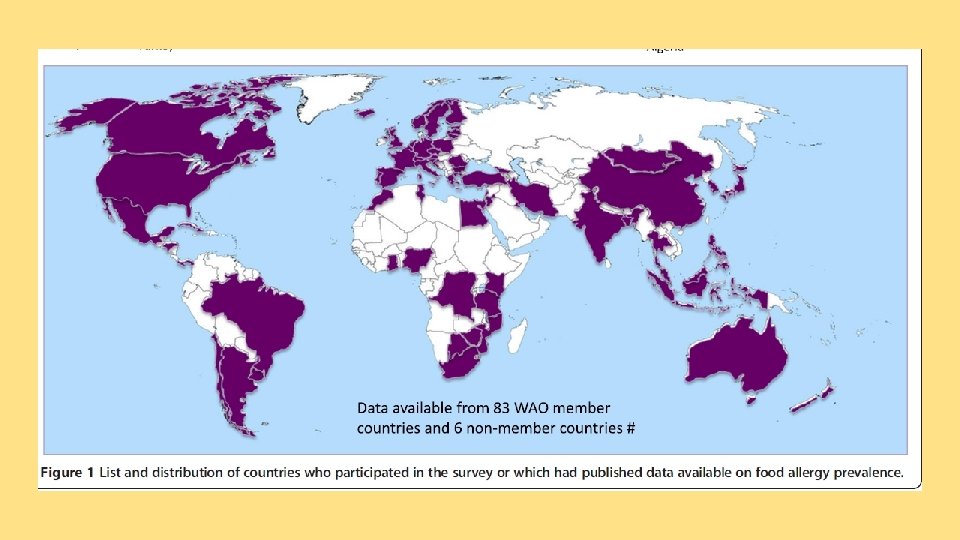
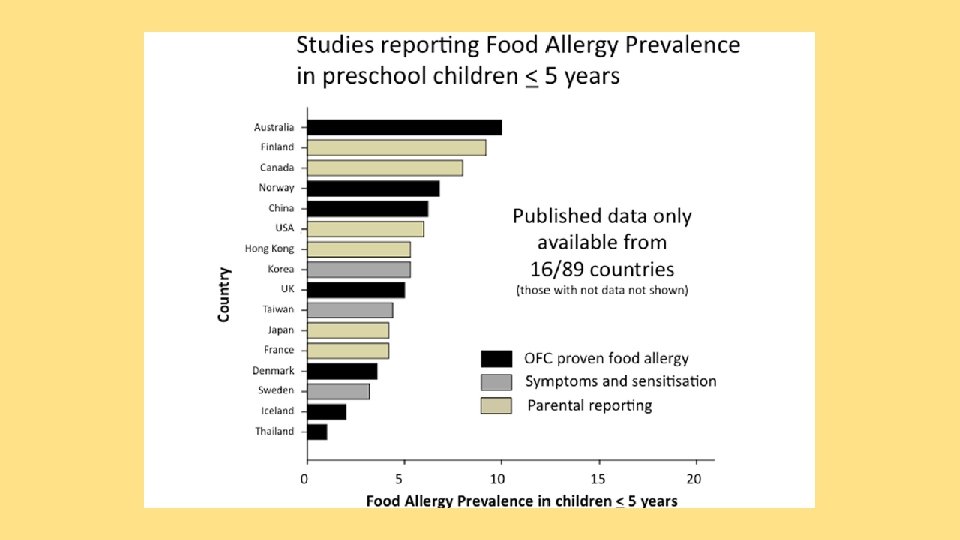
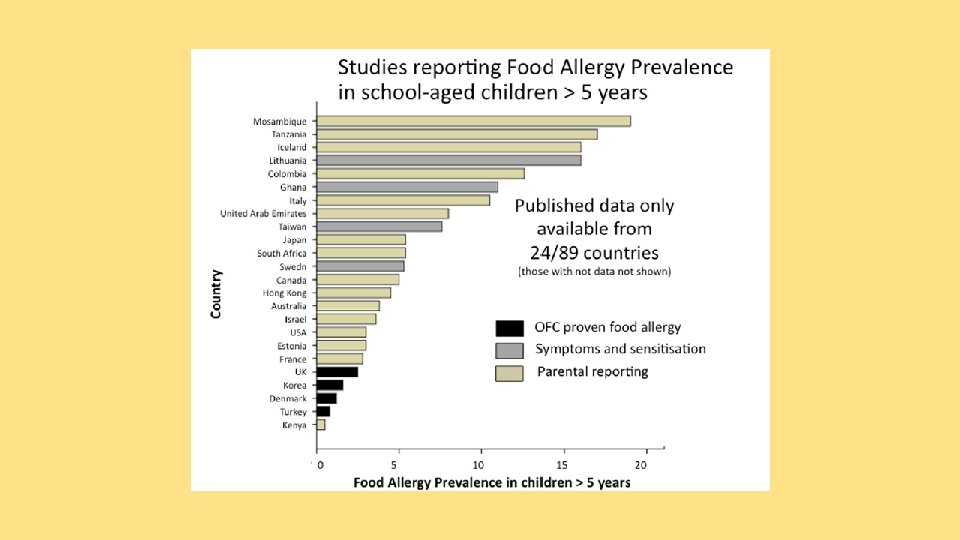
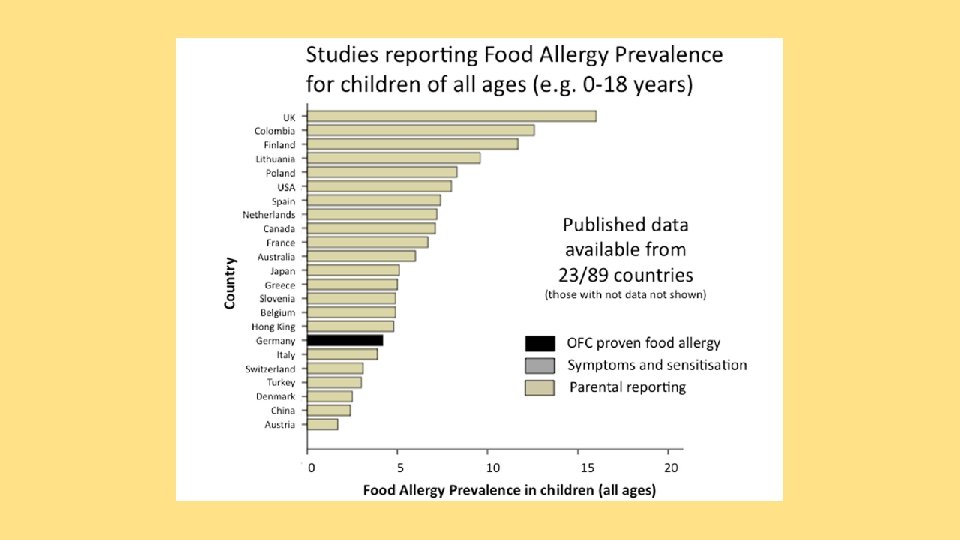
Allergie alimentari multiple q Definizione -epidemiologia q Quadri clinici q Quali rischi q Problemi nutrizionali
The natural history of cow's milk protein allergy/intolerance. Høst A 1, Jacobsen HP, Halken S, Holmenlund D. Associated adverse reactions to other foods, especially egg, soy, peanut and citrus develop in about 41 -54% Eur J Clin Nutr. 1995 Sep; 49 Suppl 1: S 13 -8.
……almost 50% non Ig. E mediated CMA react to soy …….
Nella real life pediatrica 78% hanno allergie alimentari multiple (3, 4/persona)
Allergie alimentari multiple q Definizione -epidemiologia q Quadri clinici q Quali rischi q Problemi nutrizionali
Clinical features of food protein-induced enterocolitis syndrome Chronic Signs and symptoms Acute Repetitive vomiting every 10 to 15 minutes, onset one to three hours after ingestion Intermittent, chronic vomiting (>90%) Chronic, watery diarrhea with blood/mucus Diarrhea, onset approximately five hours Lethargy after ingestion (<50%) Pallor Lethargy (70%) Dehydration Pallor (70%) Abdominal distension Dehydration Weight loss Hypotension (15%) Failure to thrive Hypothermia (25%) Abdominal distension
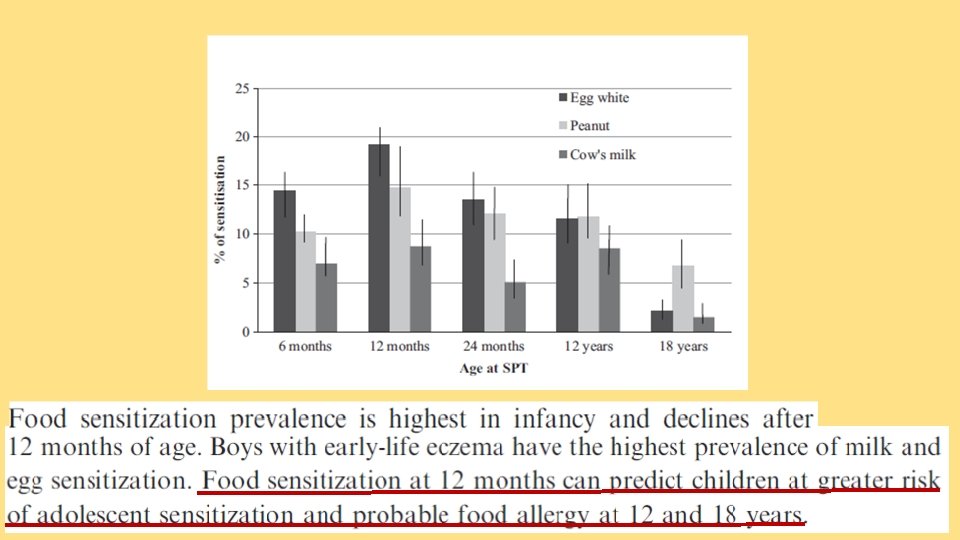
10% poly food sensitization at 6 months 15% poly food sensitization at 12 months
11% poly food sensitization at 24 months 18% poly food sensitization during the first 2 years of life
Early-life SPT to common food Altough a small proportion of allergens can provide valuable children may develop late-onset information in predicting the risk of food sensitization, it is unlikely sensibilization and food allergy into to be clinically relevant. adolescence in individuals at high risk
‘Health. Nuts’, a population-based, longitudinal food allergy study in Melbourne, 5276 infants aged 11– 15 months were recruited through 131 council-run immunization sessions from September 2007 to August 2011.
Diversi fenotipi/endotipi Class 1: No allergic disease (70%). The no allergic disease. The estimated prevalence of an episode of wheeze was 17%. Class 2: Non-food-sensitized eczema (16%). late-onset (≥ 4 months) eczema (60%), prevalence of wheeze was 24%. Class 3: Single egg allergy (9%). Half the infants had eczema (27% early-onset and 23% late-onset ) and 15% had wheeze. Class 4: Multiple food allergies (predominantly peanut) (3%). Approximately half (56%) were also allergic to egg, the prevalence of eczema was 72%, with early-onset eczema being more common (42%), whilst 23% had a history of wheezing. Class 5: Multiple food allergies (predominantly egg) (2%). egg ( prevalence 91%), sesame (50%) and peanut (39%). Early-onset eczema had the highest prevalence (58%), and an additional 31% were estimated to have reported lateonset eczema. The estimated prevalence of the history of wheeze was 14%.
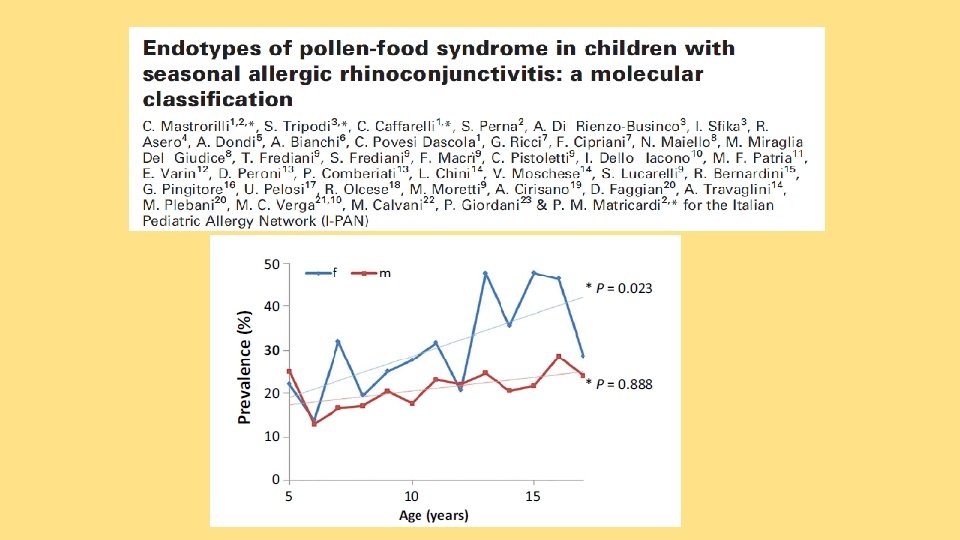
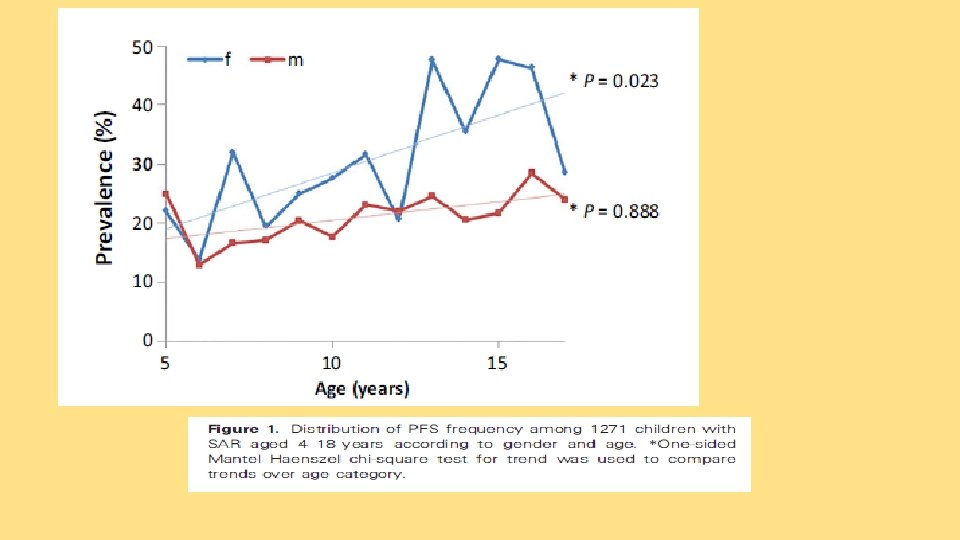
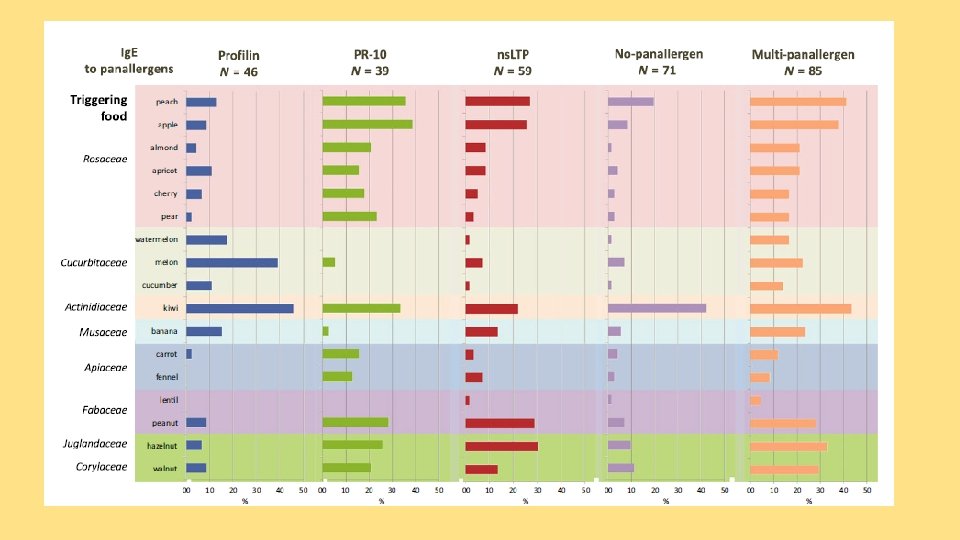
POLLEN FOOD SYNDROME Patients are sensitized to pollen allergenic molecules highly cross-reacting with their homologues in the offending foods Labial and oropharyngeal pruritus, paresthesia and angioedema of the oral mucosa, tongue, lips, palate and oropharynx, or laryngeal tightness (oral allergy syndrome) • Gastrointestinal symptoms and, rarely, life-threatening wheezing and anaphylaxis OAS can also be the clinical expression of primary sensitization to genuine and/or cross-reacting food allergens and it is frequently the first symptom of an allergic reaction in cases followed by systemic symptoms
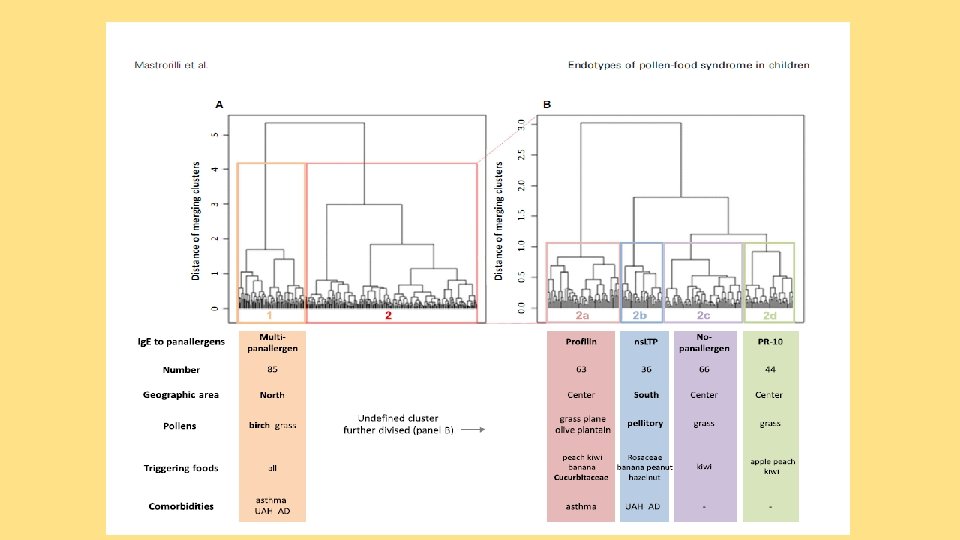
POLLEN FOOD SYNDROME ( endotypes) MONO-PANALLERGEN Bet v 1 MULTI-PANALLERGEN Pru p 3 NO PANALLERGEN Phl p 12 Mastrorilli C et al, Allergy 2016
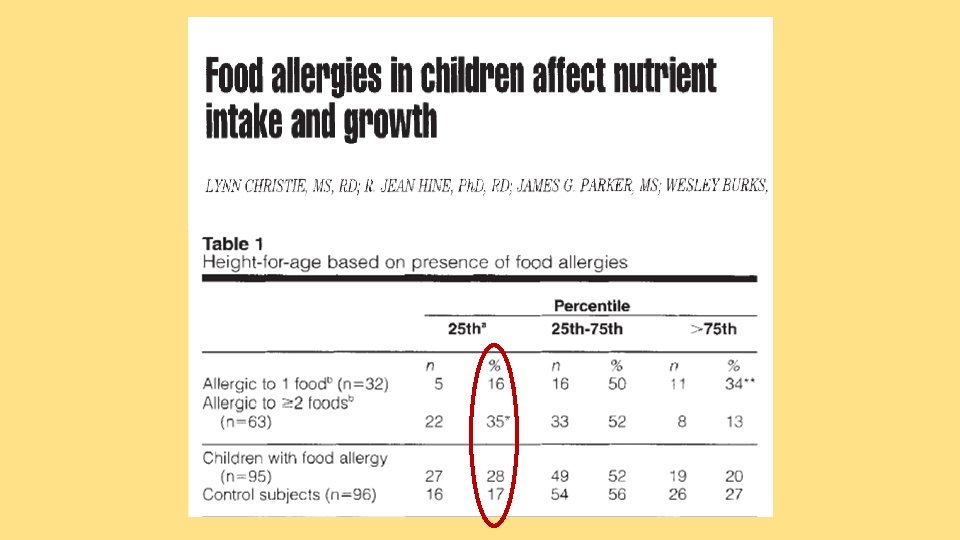
Allergie alimentari multiple q Definizione -epidemiologia q Quadri clinici q Quali rischi q Problemi nutrizionali
Aumenta il rischio di severità della allergia alimentare
Aumenta il rischio di comorbidità allergiche
Aumenta il rischio di asma
Aumenta il rischio di asma
Individuals with increased diversity of Ig. E against multiple components or epitopes may be more likely to experience severe reactions, but such diagnostic tools are not routinely available.
Allergie alimentari multiple q Definizione -epidemiologia q Quadri clinici q Quali rischi q Problemi nutrizionali
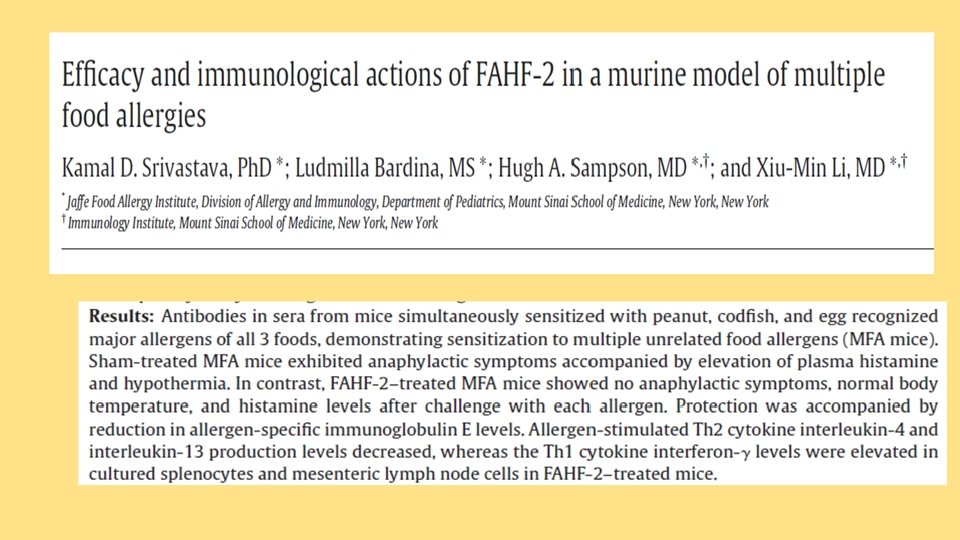
Speranze ?
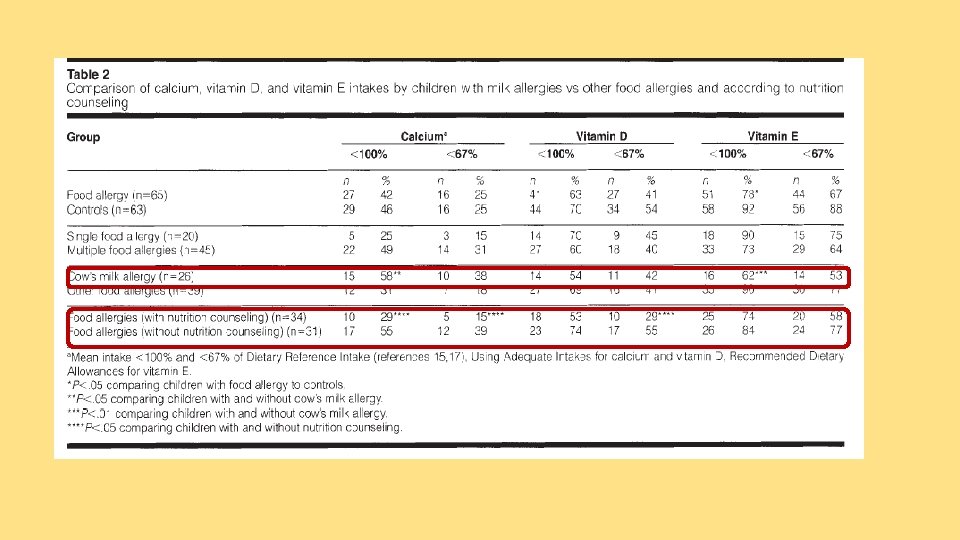
Le allergie alimentari multiple: sintesi finale • Condizione frequente • Quadri clinici molto diversi con età di esordio differente • Patogenesi Ig. E e non Ig. E-mediata • Si associano ad una maggiore severità clinica • Attenti ai problemi nutrizionali
Grazie