Infections in Neurosurgery AIKATERINI PANTELI NEUROSURGEON YEDITEPE UNIVERSITY




















 –")



























 – Lower thoracic")







- Slides: 61
Infections in Neurosurgery AIKATERINI PANTELI NEUROSURGEON YEDITEPE UNIVERSITY DEPARTMENT OF NEUROSURGERY
Antibiotics for neurosurgery • Oral penicillins – Superficial staphylococcal infections – (e. g amoxycillin + clavulanic acid ) • Cephalosporines – 1 st and 3 rd generation • Vancomycin • Chloramphenicol – (excellent CSF penetration)
Prophylaxis principles • antibiotics must be in tissues at time of contamination (give 60 minutes prior to incision) • repeated administration vital in prolonged procedures • typical infecting organisms are usually predictable. Coverage for these organisms is adequate
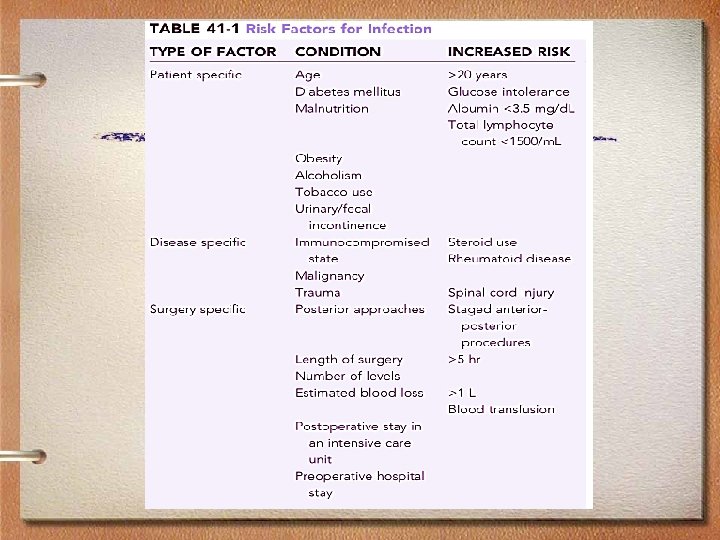
Wound Infections Risk Factors • General – Malnourishment – Anaemia – Coexisting infection – Immunocompromised patients – Diabetes mellitus
Wound Infections Risk Factors • Local – Foreign bodies – Wound drains – Haematoma formation – CSF leakage – Reoperation
Post-op wound infections • 1 -4% • Erythema, oedema, pain, purulent discharge • Patient may be febrile • Antibiotics (broad spectrum) • Complications: – Meningitis – Osteomyelitis – Abcess (epi/subdural, brain)
Osteomyelitis of the skull • Due to prolonged contact of the bone flap to purulent material in the subgaleal or epidural space • Plain X-rays, CT
Postop superficial spinal infection • Rate depends on the presence or absence of instrumentation • Erythema, pain, purulent discharge • Complication : extension to the deep surgical site
Wound infections • After spinal surgery-laminectomy etc. – – Culture Vancomycine + 3. gen cephalosporin Change after cuture results Debridement • Osteomyelitis of the skull – Remove the bone flap – Staphylococci is most common – Antibiotics (vancomycin+3. gen. Cephalosporins)
Shunt infection • Rate of infection 3 -20% • Risk factors – Young age – Length of procedure – Open neural tube defect • Pathogens: Staph epidermidis, S. Aureus, gr ( -) bacilli • Presentation: fever and headache, abdominal signs…
Treatment • • Remove the shunt i. v vancomycin Rifampin may be included Change the treatment after results of culture • İntrathecal treatment
Meningitis • Prodrome of fever, headache are benign until altered consciousness, focal neurologic deficits or seizures appear. – Community- acquired – Post-traumatic – Post- neurosurgical – Recurrent
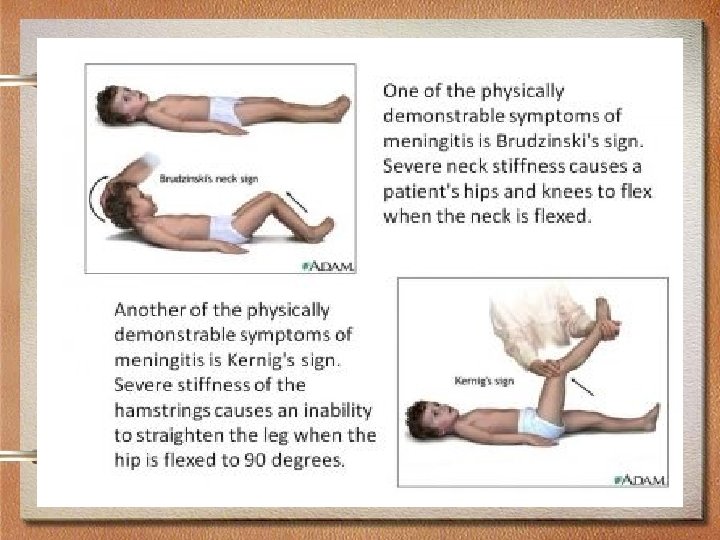
Approach to the patient: • Nuchal rigidity is the pathognomonic sign of meningeal irritation. • Kernigs’ sign • Brudzinski’s sign • Failure of a patient suspected with viral encephalitis to improve should prompt reevaluation.
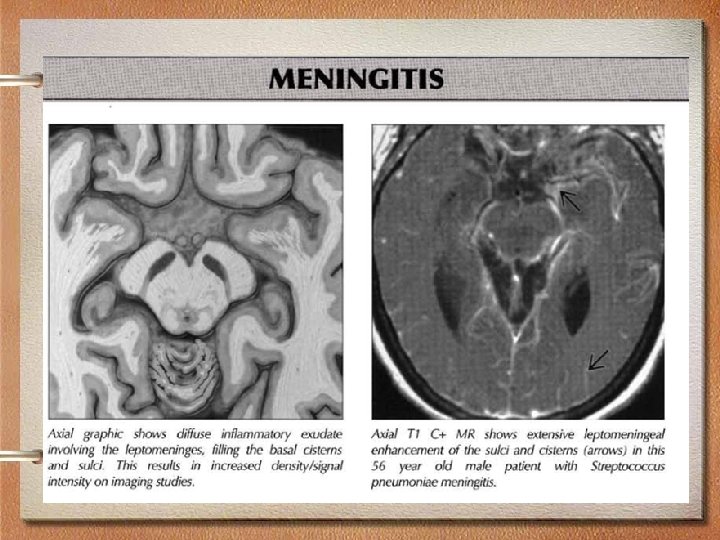
Bacterial meningitis • Bacterial meningitis is an acute purulent infection within the subarachnoid space. • Bacterial meningitis may result to decreased consciousness, seizures, raised ICP and stroke. • Meningoencephalitis – the parenchyma, meninges and subarachnoid suffer
Bacterial meningitis is the most common form of suppurative CNS infection. • S. pneumoniae is the most common cause in adults >20 • N. meningitides is common in ages 2 -20 with petechial and purpuric lesions. • Group B or S. agalactiae predominates in neonates and elderly >50 • Listeria predominates in neonates and pregnant women due to organisms in ready to eat foods • H. influenzae in unvaccinated children • Staph aureus are causes of infection following an invasive neurosurgical procedure
Pathophysiology: • Bacteria are able to avoid phagocytosis because of a polysaccharide capsule. • A critical event in the pathogenesis of bacterial meningitis is the inflammatory reaction induced by the invading bacteria.
Pathophysiology • Lysis of bacteria with the subsequent release of cell wall components into the subarachnoid space • Cytokine response is followed by an increase in CSF protein concentration and leukocytosis. • Much of the pathophysiology of bacterial meningitis is a direct consequence of elevated levels of CSF cytokines and chemokines. – TNF and IL 1 act synergistically to increase the permeability of the blood brain barrier resulting in vasogenic edema and the leakage of serum proteins into the subarachnoid space.
Pathophysiology • During the very early stages of meningitis there is an increase in cerebral blood flow followed by a decrease in blood flow and loss of cerebrovascular autoregulation. • Combination of cytotoxic, vasogenic and interstitial edema lead to increased ICP and coma.
Clinical presentation: • Clinical triad of meningitis: fever, headache and nuchal rigidity. • Focal seizures may be due to focal arterial ischemia, infarction, and cortical venous thrombosis with hemorrhage or focal edema. • Generalized seizures or status epilepticus may be due to hyponatremia and cerebral anoxia. • Raised ICP is an expected complication and is the major cause of obtundation and coma.
Signs of increased ICP are • papilledema, dilated poorly reactive pupils, 6 th nerve palsie, decerebrate posturing and Cushing’s reflex (bradycardia, hypertension, irregular respirations) • Most disastrous complication is cerebral herniation.
Diagnosis: • Examination of CSF • Classic CSF abnormalities: – leukocytosis (>100 cells) – decreased glucose <2. 2 mmol/L or serum glucose of <0. 4 – increased protein concentration >0. 45 g/L – increased opening pressure >180 mm. H 2 O
Tests • CSF latex agglutination test has a specificity of 95 -100% for S. pneumoniae and N. meningitides, so a (+) test is virtually diagnostic of bacterial meningitis. • Limulus amoebocyte lysate assay is a rapid diagnostic test for the detection of gram (–) endotoxin in CSF
Radiology • MRI is preferred than CT because of its superiority in demonstrating areas of cerebral edema and ischemia.
Differential diagnosis: • findings on CSF studies, neuroimaging and EEG distinguishes HSV encephalitis from bacterial meningitis • Viral CSF infections: – lymphocytic pleocytosis with a normal glucose • Bacterial: – PMN pleocytosis and hypoglycorrhachia
Subacutely evolving meningitis • May on occasion be considered as differential diagnosis of acute meningitis. • Principal causes include M. tuberculosis, C. neoformans, H. capsulatum, C. immitis and T. pallidum
Treatment • Treatment: bacterial meningitis is a medical emergency. • Goal is to begin antibiotic therapy within 60 min.
In meningitis following neurosurgical procedures: • vancomycin and ceftazidime • Ceftazidime is the only cephalosporin with adequate activity against CNS infections with P. aeruginosa.
Treatment • • Meropenem is a carbapenem antibiotic that is highly active in vitro against Listeria, P. aeruginosa and penicillin resistant pneumococci. Meningococcal meningitis: Pen G, if resistant Ceftriaxone. Chemoprophylaxis with Rifampicin is CI in pregnant. Pneumococcal meningitis: cephalosporin + vancomycin, MICs > 0. 5 ug/m. L treat with cefotaxime or ceftriaxone, MICs of >1 ug/m. L vancomycin Patients with penicillin and cephalosporin resistant strains of S. pneumoniae who don’t respond to vancomycin may be given intraventricular vancomycin L. monocytogenes meningitis: ampicillin/ gentamicin. In penicillin allergic patients give cotrimoxazole Staphylococcal meningitis: nafcillin, for MRSA use vancomycin Gram – bacillary meningitis: 3 rd gen cephalosporins but with P. aeruginosa use ceftazidime
Adjunctive therapy • Dexamethasone • For increased ICP: elevate head to 3045 degrees, intubation, hyperventilation and mannitol.
Viral • • • Acute Viral Meningitis: fever, headache and meningeal irritation accompanied by arthralgia, malaise and anorexia. Photophobia and pain on moving the eyes. Kernig’s and brudzinski’s sign are absent. Enteroviruses account for 75 -90% of aseptic meningitis. HSV 1 : most common sporadic cause Immunocompromised : HIV CMV Laboratory Diagnosis of CSF: – Lymphocytic pleocytosis and slightly elevated protein concentration with normal glucose. PCR – diagnostic procedure of choice HSV PCR- for recurrent episodes of aseptic meningitis Oligoclonal bands can also be found in noninfectious neurologic diseases. Enterovirus infection can have exanthema, foot and mouth disease, herpangina, pleurodynia, myopericarditis and hemorrhagic conjunctivitis ( stigmata of enterovirus infection)
Post traumatic meningitis • • 1 -20% after moderate-severe trauma Within 2 weeks after trauma 75% have skull base fracture Pathogens: nasal cavity: Gr (+) cocci and Gr (– ) bacilli – Staph hemolyticus, Strep pneumonia – E. coli, Klebsiella Pneumonia
Treatment • Surgical+ antibiotic • İmipenem and ciprofloxacin+ vancomycin
Epidural / Subdural empyema • Supurative infection that occurs in the subdural space • Trauma, thromboflebitis, sinusitis or extension of local infection to the epi/subdural space or both • May progress rapidly!!
Presentation • • • Fever Headache Meningismus Seizures CT or MRI is very helpful in diagnosis
Treatment • Surgical drainage • Antibiotics: like cerebral abcess
Cerebral abcess • Risk factors: – Pulmonary abnormalities: infection, AV fistula – Congenital cyanotic heart disease: TOF – Endocarditis – AIDS – Penetrating head trauma – Sinusitis, ent infections
Pathogens • Streptococcus is the most frequent • Anaerobes like Bacteroides • May be multiple
Presentation • Increased intracranial pressure • Diagnosed by MRI or CT • WBC, CRP, Blood cultures, ESR
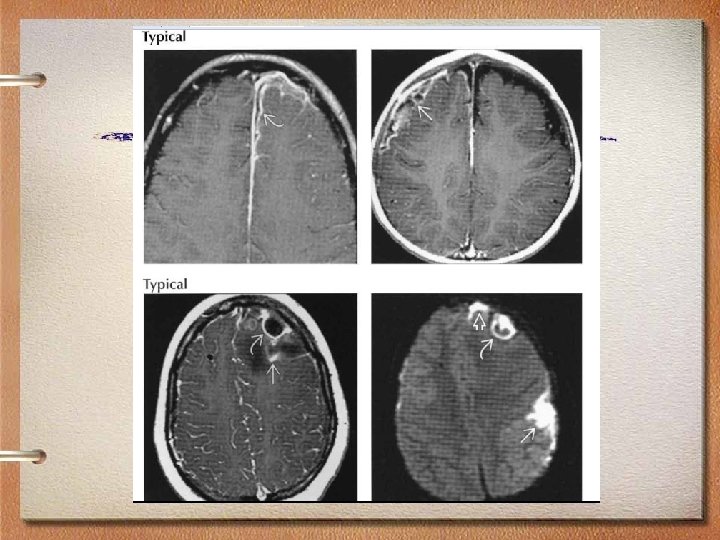
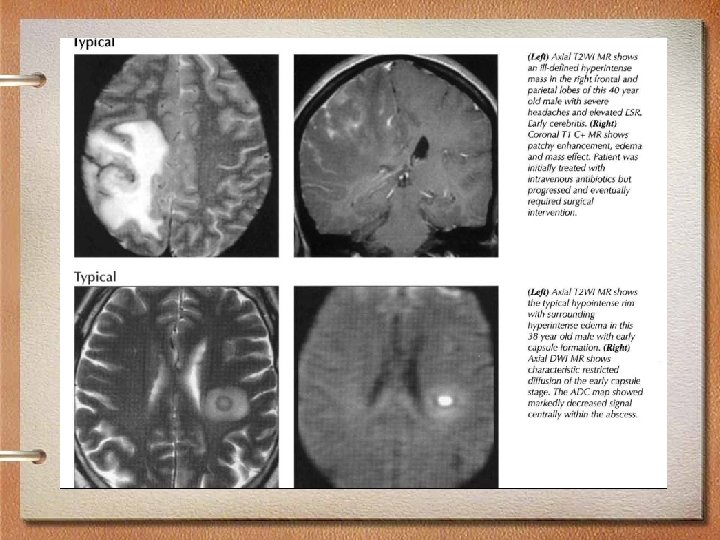
MRI findings • Imaging varies with stage of abscess development • Early capsule: Well-defined, thin-walled enhancing rim • Ring-enhancing lesion with high signal • T 2 hypointense abscess rim with surrounding edema • Typically supratentorial • Frontal and parietal lobes most common, gray-white junction (hematogenous)
Treatment • Surgical drainage • Antibiotics: vancomycine+ 3 gen. cephalosporins + metronidazol or chloramphenicol • Long term treatment by i. v antibiotics for 6 -8 weeks followed by oral antibiotics for 4 -8 weeks
VENTRICULITIS
Ventriculitis • Ventricular ependyma infection related to meningitis, ruptured brain abscess, or ventricular catheter • Common bacterial organisms: Staphylococcus, streptococcus, enterobacter • Ventriculomegaly with debris level, enhancing ependyma, periventricular T 2 hyperintensity • Mortality rate 40 -80%!! • Treat underlying organism, drain/intrathecal antibiotics.
Hydatid cyst • • Echinococcosis granulosis is a dog tapeworm Endemic disease and dogs are the hosts Sheep and man are the intermediate hosts Presentation is by signs of intracranial pressure • Treatment is surgical evacuation • Antibiotic treatment is albendazole
Fungal infections • Candidiasis is the most common • Most common in immunocompromised patients • Treatment: antifungal agents: fluconazole, amphotericin B
Spinal infections • • • Vertebral osteomyelitis Discitis Epidural abcess Subdural empyema Meningitis Spinal cord abcess
Vertebral osteomyelitis • Pyogenic • Nonpyogenic – Tuberculous spondylitis – Brucellosis – Aspergillosis – Blastomycosis – Coccidiomycosis – Candida tropicalis
Vertebral osteomyelitis • Lumbar spine is the most common site • Risk factors – Diabetes – IV drug abuse – Hemodialysis – Immunosupression – Spine surgery
Clinical presentation and diagnosis • • • Pain Fever Paraspinal spasm Elevated: CRP, ESR, WBC MRI and CT is very helpful
Treatment • Staphylococcus is the most common • Tuberculosis (Pott`s disease) – Lower thoracic and upper lumbar levels are most common – Psoas abcess is common – Surgery is required in cord compression or in abcess formation • In staph aureous – Long term antibiotics: 3. Generation cephalosporin+vancomycine for 6 -8 weeks IV+ POrifampin • In TBC 9 months with 3 Anti tbc drugs
Discitis • Infection of the disc space • Presents with pain and limitation of the motion • Fever, paraspinal spasm • MRI demonstrates involvement of the disc space • Treatment is immobilisation and antibiotic therapy
Discitis
Spinal epidural abcess • Often associated with vertebral osteomyelitis • Hematogenous spread is most common and skin infections are most common in etiology • Treatment is by surgical treatment and long term antibiotic treatment
Spinal epidural abcess
Spinal subdural empyema • Spinal subdural empyema is an exceptionally rare and serious condition • Immediate surgery with complete exposure and drainage of the abscess is generally recommended, followed by i. v antibiotics
Coffee break
THANK YOU