Imaging of Cirrhosis Portal Hypertension dr Harry Galuh







 Chronic infections hepatitis C, B, B+D brucellosis, syphilis Chr.")






 • Computed Tomography Scan ( CT Scan)")


 Coarse parenchyma and innumerable tiny, hyperechoic nodules.")
 sagittal image showing an enormous caudate lobe")
. Gray-scale image of hepatic vein shows a tapered luminal narrowing")


 Definition: it is an increase in portal venous pressure. Portal vein")

 Scarring narrows and")















- Slides: 51
Imaging of Cirrhosis & Portal Hypertension dr. Harry Galuh Nugraha, Sp. Rad Department of Radiology-Faculty of Medicine Padjadjaran University/Hasan Sadikin Hospital
Introduction v. Cirrhosis is derived from Greek word kirros=orange or tawny and osis=condition v. Term was 1 st coined by Laennec in 1826 v. Many definitions but common theme is injury, repair, regeneration and scarring
v. Primary histologic features: 1. Marked fibrosis 2. Destruction of vascular & biliary elements 3. Regeneration 4. Nodule formation
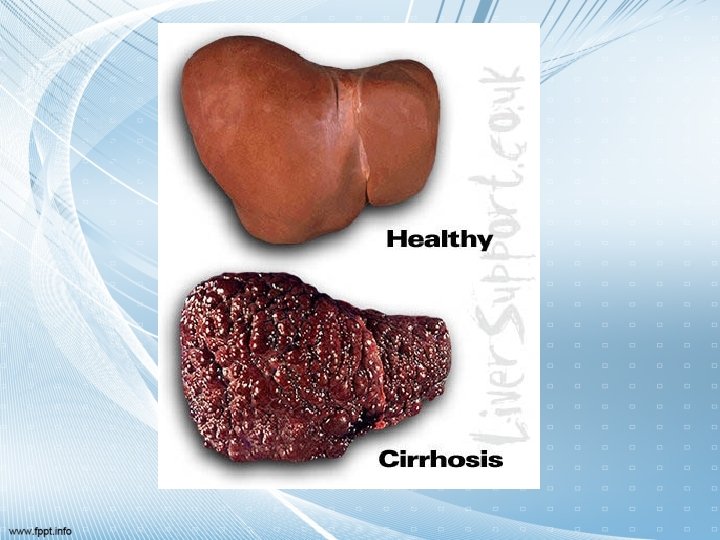
Definition • Cirrhosis is a pathological diagnosis. It is characterized by widespread fibrosis with nodular regeneration. Its presence implies previous or continuing hepatic cell damage
• WHO definition : a diffuse process characterized by liver necrosis and fibrosis and conversion of normal liver architechture into structurally abnormal nodules that lack normal lobular organization.
• Cirrhosis is common end result of many chronic liver disorders. • Diffuse scarring of liver – follows hepatocellular necrosis of hepatitis. • Inflammation – healing with fibrosis Regeneration of remaining hepatocytes form regenerating nodules. • Loss of normal architecture & function.
Etiology v v Alcohol (>70%) Chronic infections hepatitis C, B, B+D brucellosis, syphilis Chr. biliary obstruction Stricture, stones, cystic fibrosis, cong. b. atresia, ~cysts Autoimmune v v v Cardiovascular heart failure, pericarditis, Budd-Chiary-sy Metabolic/genetic errors Fe, Cu, α 1 -AT, lipids, Drugs and chemicals NASH Cryptogenic Combined
Anatomy
Pathophysiology Primary event is injury to hepatocellular elements Initiates inflammatory response with cytokine release->toxic substances Destruction of hepatocytes, bile duct cells, vascular endothelial cells Repair thru cellular proliferation and regeneration Formation of fibrous scar
Classification of Cirrhosis • WHO divided cirrhosis into 3 categories based on morphological characteristics of the hepatic nodules 1. Micronodular 2. Macronodular 3. Mixed
Micronodular Cirrhosis Nodules are <3 mm in diameter Relatively uniform in size Distributed throughout the liver Rarely contain portal tracts or efferent veins Liver is of uniform size or mildly enlarged Reflect relatively early disease
Macronodular & Mixed Cirrhosis • Nodules are >3 mm in diameter and vary considerably in size • Usually contain portal tracts and efferent veins • Liver is usually normal or reduced in size • Mixed pattern if both type of nodules are present in equal proportions
Multimodality imaging • Ultrasonography ( US ) • Computed Tomography Scan ( CT Scan) / Magnetic Resonance Imaging ( MRI )
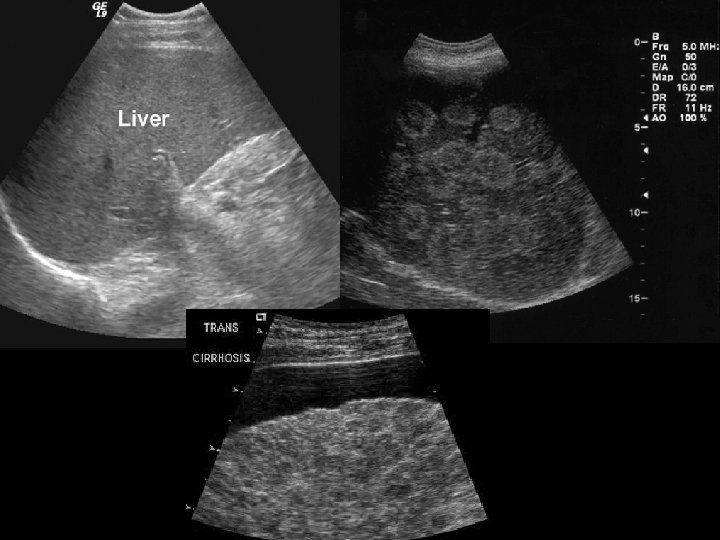
US FEATURES Volume redistibution Coarse echotexture Noduler surface Nodules regenerative and dysplastic Portal Hypertension ascites, splenomegaly and varices
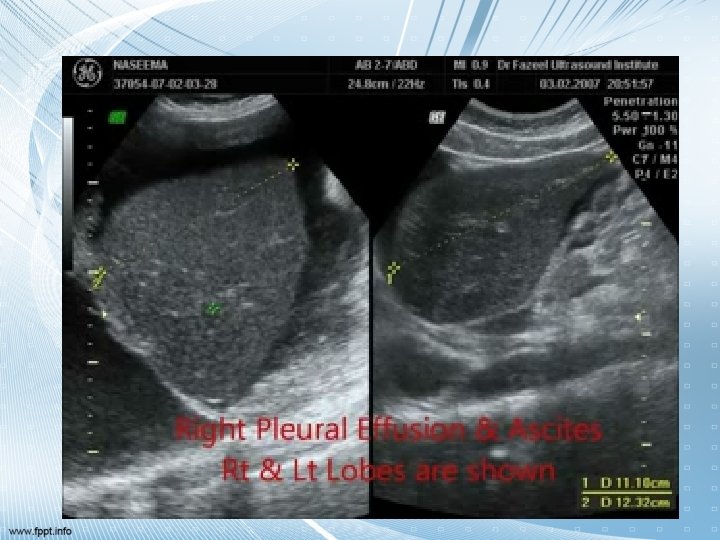
US SIGN OF LIVER CIRRHOSIS ARE • Increase echogenicity of liver parenchyma (due to associated fatty infiltration) • Irregular liver surface • Loss of normal liver architecture, i. e loss of visibility of hepatic blood vessels • Enlarged spleen • Enlarged posrtal vein>13 mm • Decreased or reversed portal vein flow on Doppler studies • Varices may be seen in the spelnic hilum and around the head of the pancreas, and the recanalized umbilical vein may be seen in the falciform ligament • Ascites
a b c Cirrhosis-spectrum of appearance: (a) Coarse parenchyma and innumerable tiny, hyperechoic nodules. (b) coarse parenchyma and innumerable, tiny hypoechoic nodules. (c) coarse parenchyma and surface nodularity.
d e f Cirrhosis-spectrum of appearance: (d) sagittal image showing an enormous caudate lobe (e) transverse sonogram shows that the right lobe is small and there is enlargement of the left lateral segment (f) subcostal oblique view showing a tiny right lobe (g to i) of the liver, which is separated from the large left lobe by the main lobar fissure (arrows).
Hepatic vein strictures-cirrhosis: (a). Gray-scale image of hepatic vein shows a tapered luminal narrowing (b) Color Doppler image shows appropriately directed flow toward the inferior vena cava in blue. There is color aliasing from the rapid velocity flow through the points of narrowing
Congestive-cirrhosis: The liver still has a normal parenchymal echo pattern, but note the curved, bulging inferior border and the tiny breaks in the capsule (arrows). A=ascites
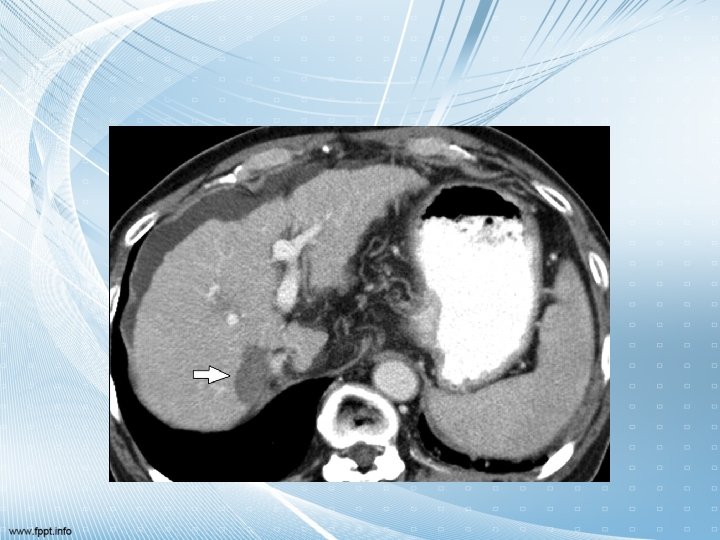
CT SIGN OF LIVER CIRRHOSIS INCLUDE • Irregular contour • Decreased density with fatty changed or increased density with haemochromatosis • Enlarged caudate lobe • Enlarged spleen • Varices: discrete round or tubular structures that enhance with contrast • Ascites
Portal Hypertension (PH) Definition: it is an increase in portal venous pressure. Portal vein pressure above the normal range of 5 to 8 mm Hg Portal vein - Hepatic vein pressure gradient greater than 5 mm Hg (>12 clinically significant) Represents an increase of the hydrostatic pressure within the portal vein or its tributaries
CT Liver Cirrhosis with portal hypertension
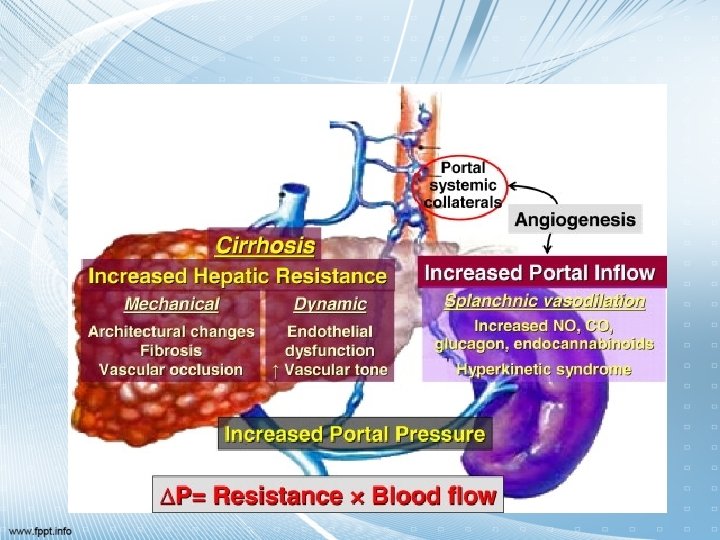
Pathophysiology of PH Cirrhosis results in scarring (perisinusoidal zdeposition of collagen) Scarring narrows and compresses hepatic sinusoids (fibrosis) Progressive increase in resistance to portal venous blood flow results in PH Portal vein thrombosis, or hepatic venous obstruction also cause PH by increasing the resistance to portal blood flow
Pathophysiology of PH As pressure increases, blood flow decreases and the pressure in the portal system is transmitted to its branches Results in dilation of venous tributaries Increased blood flow through collaterals and subsequently increased venous return cause an increase in cardiac output and total blood volume and a decrease in systemic vascular resistance With progression of disease, blood pressure usually falls
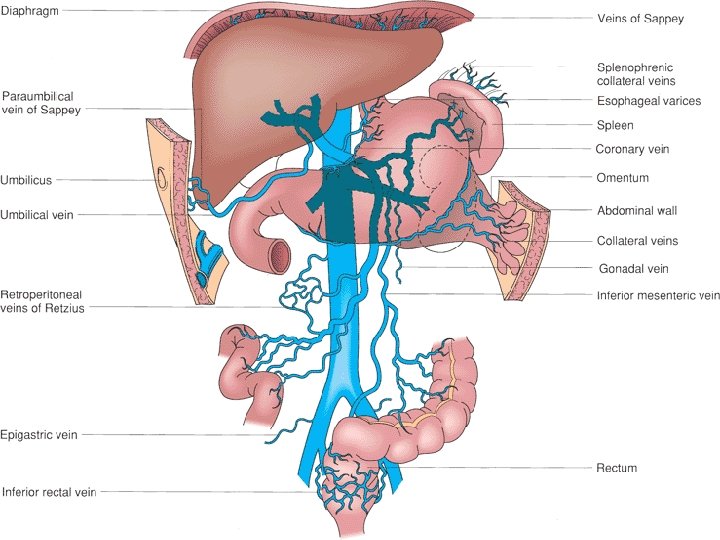
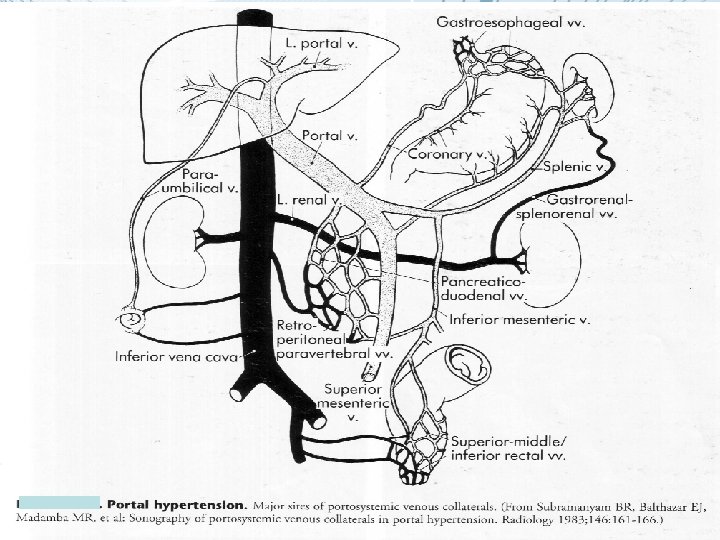
Portal Vein Collaterals Coronary vein and short gastric veins -> veins of the lesser curve of the stomach and the esophagus, leading to the formation of varices Inferior mesenteric vein -> rectal branches which, when distended, form hemorrhoids Umbilical vein ->epigastric venous system around the umbilicus (caput medusae) Retroperitoneal collaterals ->gastrointestinal veins through the bare areas of the liver
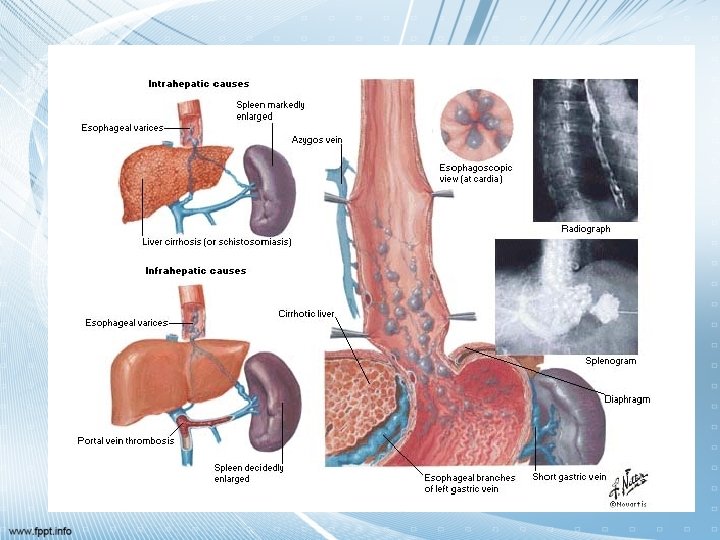
Etiology of PH Causes of PH can be divided into 1. Pre-hepatic 2. Intra-hepatic 3. Post-hepatic
Pre-hepatic PH Caused by obstruction to blood flow at the level of portal vein Examples: congenital atresia, extrinsic compression, schistosomiasis, portal, superior mesenteric, or splenic vein thrombosis
Post-hepatic Caused by obstruction to blood flow at the level of hepatic vein Examples: Budd-Chiari syndrome, chronic heart failure, constrictive pericarditis, vena cava webs
Complications of PH GI bleeding due to gastric and esophageal varices Ascites Hepatic encephalopathy
Varices Most life threatening complication is bleeding from esophageal varices Distal 5 cm of esophagus Usually the portal vein-hepatic vein pressure gradient >12 mm Hg Bleeding occurs in 25 -35% of pts. With varices and risk is highest in 1 st yr.
US finding of PH • Secondary signs of splenomegaly, ascites, and portosystemic-venous collateral • Five major sites of portosystemic venous collaterals are visualized by US: – – – Gastroesophageal junction Paraumbilical vein Splenorenal dan gastrorenal veins Intestinal-retroperitoneal anastomoses Hemorrhoidal veins
Portal Hypertension a d b e c f a. Recanalized paraumbilical vein b. Enlarged coronary vein c. Extensive varices d. Extensive varices e. Sphlenic hilar varices f. Sphlenic hilar varices
Portal hypertension: Recanalized paraumbilical vein
Portal Hypertension: Enlarged coronary vein
Portal Hypertension: Extensive varices
Portal Hypertension: Sphlenic hilar varices
Conclusion Ultrasound the first investigation Liver cirrhosis commonly leads to a shrunken irregular liver with splenomegaly and ascites CT/MRI more sensitive than US in detecting HCC in patients with cirrhosis CT & MRI superior to US, both in lession detection and characterization
Thank U