Cirrhosis Dr Gerrard Uy Cirrhosis a histopathologically defined









 –")









 have been shown to improve")













- Slides: 35
Cirrhosis Dr. Gerrard Uy
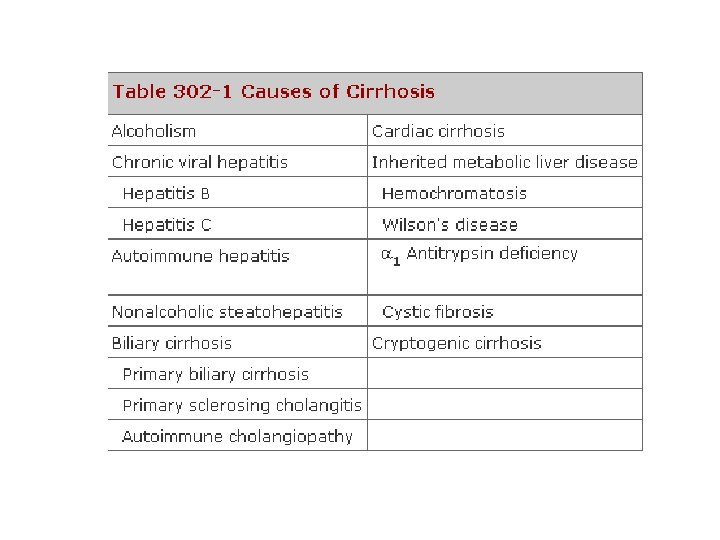
Cirrhosis • a histopathologically defined condition – pathologic features consist of the development of fibrosis to the point that there is architectural distortion with the formation of regenerative nodules • Decreased mass and function
Alcoholic Cirrhosis • Excessive alcohol use can lead to development of: • alcoholic fatty liver • alcoholic hepatitis • alcoholic cirrhosis • Chronic alcohol use can produce fibrosis in the absence of accompanying inflammation
Alcoholic Cirrhosis • Pathogenesis: – Alcohol is the most commonly used drug in US – Ethanol is mainly absorbed by the small intestine – Three enzyme systems account for metabolism of alcohol in the liver – majority of ethanol oxidation occurs via ADH to form acetaldehyde – acetaldehyde-mediated hepatocyte damage – Hepatocyte loss occurs, and with increased collagen production and deposition – liver contracts and shrinks in size
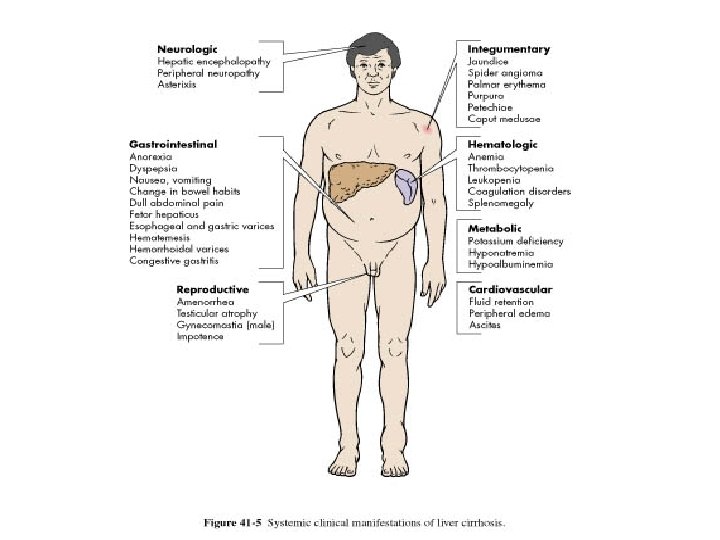
Alcoholic Cirrhosis • Clinical Features: – requires an accurate history regarding both amount and duration of alcohol consumption – nonspecific symptoms such as vague right upper quadrant pain, fever, nausea and vomiting, diarrhea, anorexia, and malaise – more specific complications of chronic liver disease, including ascites, edema, or upper gastrointestinal (GI) hemorrhage – jaundice or encephalopathy
Alcoholic Cirrhosis • Physical Exam: – Hepatomegaly, splenomegaly – scleral icterus, palmar erythema, spider angiomas, parotid gland enlargement, digital clubbing, muscle wasting, or the development of edema and ascites – Men: decreased body hair and gynecomastia – Women: menstrual irregularities
Alcoholic Cirrhosis • Lab tests: – may be completely normal – early cirrhosis – advanced liver disease: • • Anemia Serum total bilirubin can be normal or elevated Prothrombin times are often prolonged aminotransferases (ALT, AST) are typically elevated
Alcoholic Cirrhosis • Diagnosis: – HISTORY AND PE – Liver biopsy can be helpful to confirm a diagnosis but witheld until abstinence has been maintained for at least 6 months
Alcoholic Cirrhosis • Treatment: – ABSTINENCE - cornerstone of therapy – good nutrition and long-term medical supervision – Glucocorticoids – if no infection – Acetaminophen use is often discouraged
Cirrhosis due to Hep B and Hep C • hepatitis C virus (HCV) – approximately 80% develop chronic hepatitis C – and of those, about 20– 30% will develop cirrhosis over 20– 30 years – liver is small and shrunken with characteristic features of a mixed micro- and macronodular cirrhosis – inflammatory infiltrate is found in portal areas
Cirrhosis due to Hep B and Hep C • hepatitis B – about 5% develop chronic hepatitis B – and about 20% of those patients will go on to develop cirrhosis – ENDEMIC in southeast asia • up to 15% of the population may be infected having acquired the infection vertically at the time of birth
Cirrhosis due to Hep B and Hep C • CLINICAL FEATURES – can present with the usual symptoms and signs of chronic liver disease – Fatigue, malaise, vague right upper quadrant pain, and laboratory abnormalities – including quantitative HCV RNA testing and analysis for HCV genotype – hepatitis B serologies to include HBs. Ag, anti-HBs, HBe. Ag (hepatitis B e antigen), anti-HBe, and quantitative HBV DNA levels
Cirrhosis due to Hep B and Hep C • TREATMENT – Management of complications – beneficial effects of antiviral therapy – chr Hep B – Treatment of patients with cirrhosis due to hepatitis C is a little more difficult because the side effects of pegylated interferon and ribavirin – if it is successful, the benefit is great and disease progression is reduced
Biliary Cirrhosis • Depends on the anatomic site of involvement: – Intrahepatic obstruction – Extrahepatic obstruction • Common causes: – Primary biliary cirrhosis – Autoimmune cholangitis – Primary sclerosing cholangitis – Idiopathic adulthood ductopenia
Primary Biliary Cirrhosis • • • 100 -200 individuals per million Strong female preponderance Median age of around 50 years Cause is unknown Characterized by portal inflammation and necrosis of cholangiocytes
Primary Biliary Cirrhosis • Pathology – 4 distinct stages of the disease – Earliest lesion is chronic nonsuppurative destructive cholangitis • Clinical Features – fatigue out of proportion for the severity of the liver disease and age of the patient – Pruritus is seen in 50% of patients
Primary Biliary Cirrhosis • Physical Examination – Jaundice – Complications of chronic liver disease – Features that are unique to PBC • Hyperpigmentation • Xanthelasma • Xanthomata
Primary Biliary Cirrhosis • Laboratory Findings – Elevated GGT and ALP – Mildy elevated SGPT and SGOT – Hyperbilirubinemia – Thrombocytopenia – Anemia – leukopenia
Primary Biliary Cirrhosis • Diagnosis – Considered in middle aged women with chronic cholestatic liver enzyme abnormalities – Liver biopsy is most important
Primary Biliary Cirrhosis • Treatment – Ursodeoxycholic acid (UDCA) have been shown to improve both biochemical and histologic features – 13 -15 mg/kg/day – Frequent naps should be encouraged – Antihistamines for pruritus – Liver transplantation is the treatment of choice
Cardiac Cirrhosis • Definition – long-standing right-sided congestive heart failure may develop chronic liver injury and cardiac cirrhosis
Cardiac Cirrhosis • Pathogenesis: – elevated venous pressure transmitted via the inferior vena cava and hepatic veins to the sinusoids of the liver – become dilated and engorged with blood – liver becomes enlarged and swollen, and with long -term passive congestion and relative ischemia due to poor circulation – become necrotic, leading to pericentral fibrosis
Cardiac Cirrhosis • Diagnosis – diagnosis is usually made in someone with clearcut cardiac disease who has an elevated ALP and an enlarged liver
Other Types of Cirrhosis • Hemochromatosis – Inherited disorder of iron metabolism that results in progressive increase in hepatic iron deposition leading to cirrhosis and hepatocellular carcinoma • Wilson’s Disease – Inherited disorder of copper homeostasis leading to increase deposition of copper in the liver
Major Complications
Portal Hypertension • Defined as elevation of the hepatic venous pressure gradient to >5 mmhg • Pathogenesis – Increased intrahepatic resistance to the passage of blood flow through the liver – Increased splanchnic blood flow secondary to vasodilation
Portal Hypertension • Responsible for 2 major complications of cirrhosis – Variceal hemorrhage – ascites • Subcategorized into prehepatic, intrahepatic, and posthepatic • 3 primary complications – Gastroesophageal varices – Ascites – hypersplenism
Spontaneous Bacterial Peritonitis • SBP is a common and severe complication of ascites • Can occur in up to 30% of individuals with severe cirrhosis and ascites • Bacterial translocation is the presumed mechanism for the development of SBP
Spontaneous Bacterial Peritonitis • Most common organisms: – E. coli – Streptococcus viridans – Staphylococcus aureus – Enterococcus sp. • Diagnosis of SBP is made when the fluid sample has an absolute neutrophil count > 250/mm 3 • Cefotaxime is the most commonly used antibiotic
Hepatorenal syndrome • A form of functional renal failure without renal pathology • Occurs in about 10% of patients with advanced cirrhosis • Diagnosis is made in the presence of a large amount of ascites in patients who have a progressive increase in creatinine • Best therapy is liver transplantation
Hepatic Encephalopathy • Defined as an alteration in mental status and cognitive function occurring in the presence of liver failure • Results from accumulation of gut derived neurotoxins • Ammonia levels are typically elevated
Hepatic Encephalopathy • Clinical Features – Changes in mental status occurs within weeks to months – Brain edema is usually present – Usually precipitated by: • • • Hypokalemia Infection Dehydration Increase dietary protein load Electrolyte imbalance
Hepatic Encephalopathy • Treatment – Hydration and correction of electrolyte imbalance – Mainstay of treatment is lactulose – Zinc supplementation can sometimes be helpful