Futuristic strategies for asthma management Jaideep A Gogtay


















-salbutamol , (S)salbutamol , (R, S)-salbutamol and placebo on FEV")






-isomer 2. 5 -1 2 (S)-salbutamol *p<0. 001")








- Slides: 37
Futuristic strategies for asthma management Jaideep A Gogtay MD Cipla Ltd Mumbai, India
Why do we need new weapons? • No cure • Current therapy effective, but asthma control is inadequate in majority of patients • Compliance poor with inhaled therapy • Fear about inhaled steroids • In 5% of patients current therapies do not work • Different asthma phenotypes ? ?
Strategies for new therapies • Improved understanding of the disease process – Development of novel compounds • Improvement of existing classes of drugs • Enhancing outcomes with current therapies
Novel compounds
Inhibitor Transcription factor NFk. B Antisense oligonucleotide m. RNA Monoclonal antibody Cytokine Soluble cytokine receptor Cytokine receptor Kinase inhibitor Signal transduction Antagonist
Inhibition of pro-inflammatory cytokines • IL-5 antibody – Mepolizumab reduces circulating and sputum eosinophils, but no effect on AHR • Soluble IL-4 receptors – improved asrhma control; no further effects seen • TNF inhibitors – etanercept, infliximab produce remarkable responses in patients unresponsive to steroids
Ig. E - Omalizumab • Recombinant Humanised Monoclonal anti-Ig. E antibody • Decreases response to both early and late allergen challenge • Reduces exacerbations and improved quality of life • Indicated in allergic asthma and allergic rhinitis • Steroid sparing • 10, 000 $/year
PHOSPHODIESTERASE 4 INHIBITORS ? CD 8+ lymphocyte PDE 4 IL-8, LTB 4 PDE 4 INHIBITORS Alveolar macrophage (eg cilomilast, roflumilast) Neutrophil PROTEASES Alveolar wall destruction (Emphysema) Neutrophil elastase Cathepsins Matrix metalloproteinases Mucus hypersecretion (Chronic bronchitis)
Improvement of existing classes of drugs New Steroids New bronchodilators
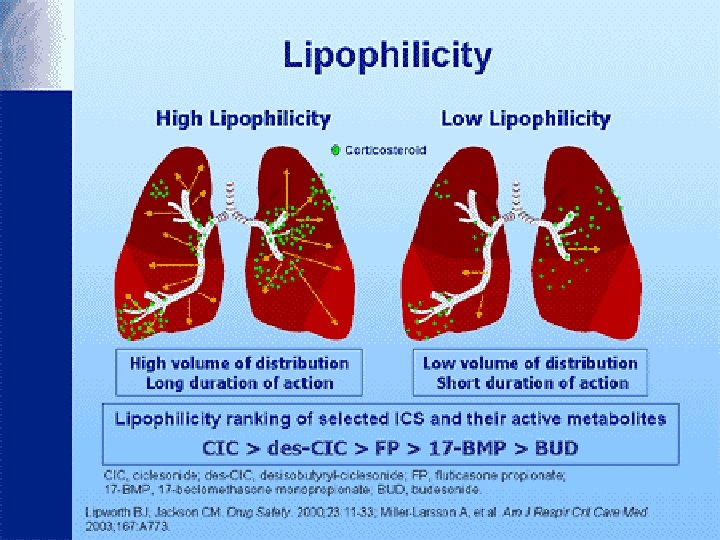
Inhaled steroids • • • Beclomethasone/Triamcinolone Budesonide Fluticasone Mometasone Ciclesonide
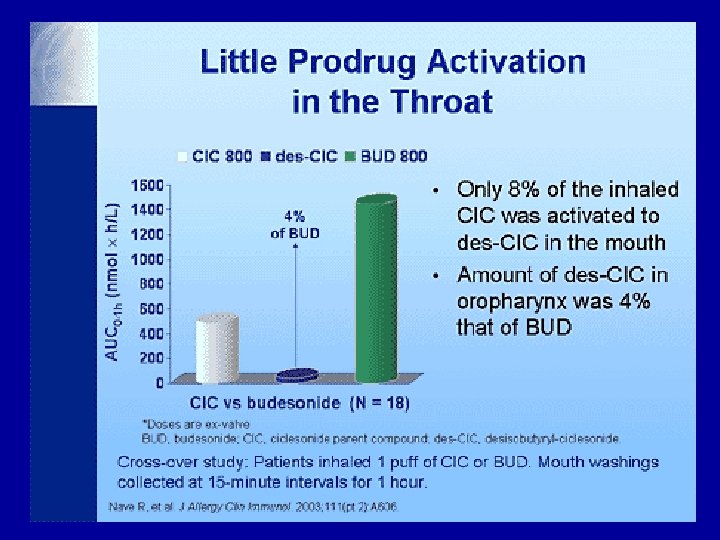
Improvements in steroids Ciclesonide Inactive compound Lungs Activated by esterases to Desisobutyrl ciclesonide Systemic circulation Inactive
Dissociated steroids Steroids Transactivation Transrepression The different effects of steroids have been attributed to binding at different domains of the receptor
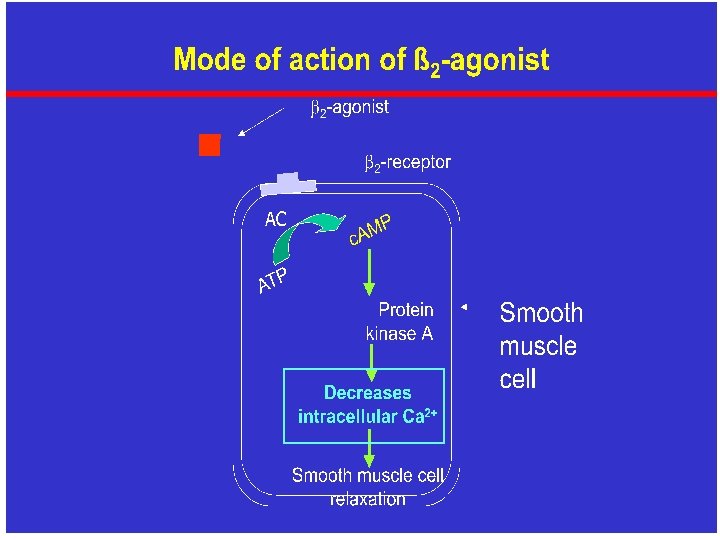
New bonchodilators • New long acting bronchodilators used once daily – under development • Chiral separation of isomers of bronchodilators viz. levosalbutamol, R, R -formoterol
Salbutamol isomers are enantiomers Mirror images that are non-superimposable upon one another
Salbutamol exhibits chirality Levosalbutamol S-Salbutamol CH 3 C NH OH C* C* CH 3 NH C CH 3 HO HO CH 3 OH OH *Chiral carbon atom OH CH 3
Fundamental Biochemistry and chiral science • The biological messenger molecules and cell surface receptors that medicinal chemists try to target are chiral, so drug molecules must match their stereochemistry. • The building blocks of nucleic acids, proteins and carbohydrates are single isomers
Thalidomide tragedy was due to the presence of the R isomer
Epinephrine – Natural bronchodilator Endogenous epinephrine produced by the adrenal glands responsible for bronchodilation is a single isomer – (R)-epinephrine • However all beta- agonist drugs including salbutamol, developed on the basis of epinephrine are racemates
Mean effect of inhaled (R)-salbutamol , (S)salbutamol , (R, S)-salbutamol and placebo on FEV 1 3. 4 FEV 1(L) 3. 2 (R)-Salbutamol (R, S)-Salbutamol (S)-Salbutamol 3. 0 Placebo 2. 8 2. 6 2. 4 (R)-/(S)-Salbutamol: Pre 6. 25 12. 5 (R, S)-Salbutamol: Dose 12. 5 25 50 Dose 50 100 200 400 800 1600 3200
Airway hyperresponsiveness Change in PD 20 of methacholine * * *p<0. 05 Vs placebo & (S)
Effect of S and R salbutamol on intracellular calcium in bovine tracheal smooth muscle cells Mol Pharmacol 1998; 53: 347 - 54
Effect of R and S salbutamol on various inflammatory mediators Control R 10 -8 + S 10 -8 R 10 -8 + S 10 -6 JACI, 2002; 109: 449 -54
Effect of enantiomers with steroid on GM-CSF production by human airway smooth muscle cells JACI 2004; 113 (2): 159
Recognized by US FDA “S-salbutamol not only fails to relax airway smooth muscle but under certain circumstances (absence of R isomer; activated cells) may augment bronchial constriction…increased intracellular calcium and BHR…. ” FDA Medical Reviewer, 1999
Pharmacokinetic data obtained in plasma after administration of a 4 mg tablet to healthy volunteers S-salbutamol R-salbutamol 3. 2 AUC 0 -6 h ng. m. L– 1. hr Cmax ng. m. L– 1 26. 5 7. 2 1. 0
Repeated Inhalations lead to accumulation of (S)-isomer 2. 5 -1 2 (S)-salbutamol *p<0. 001 * (R)-salbutamol 1. 5 1 0. 5 Plasma concentration ng. m. L 0 3 hours 6 hours Time after inhalation (hrs. ) 9 hours
Mean % change in FEV 1 after the first dose in a subgroup of patients with pretreatment FEV 1 of < 60% of predicted Mean changes in FEV 1 (%) Day 0 (Week 0) 55 50 45 40 35 30 25 20 15 10 5 0 Lev 1. 25 (n=36) Lev 0. 63 (n=32) Rac 2. 5 (n=38) Rac 1. 25 (n=26) PBO (n=37) R-salbutamol 1. 25 – 52% Racemic salbutamol 2. 5 – 37% Pre 0 Nelson et al, JACI, 1998 1 2 3 4 Time (hrs) 5 6 7 8
Change in mean glucose Change in mean heart rate Change in mean K+
Superior therapeutic index
Changes in FEV 1 in the emergency department Am J Emerg Med 2004; 22 (1): 29 -36
Levosalbutamol Vs Salbutamol nebulization N=338, 4 -11 years J Allergy Clin Immunol 2001; 108: 938 -45
Mean change in heart rate 30 mins after dosing *# *#+ *# *# *# * p<0. 001 vs plac; #p< 0. 02 vs lev 0. 31; +p<0. 002 vs rac 2. 5 J Allergy Clin Immunol 2001; 108: 938 -45
Enhancing outcomes with current therapies • Inhaled steroids + LABAs • Montelukast • Treatment must be taken regularly even if there are no symptoms • Inhaler technique must be correct
Conclusion Improve on current steroids and bronchodilators Understanding asthma phenotypes Future management Novel compounds Easier to use devices Compliance