Management of Asthma asthma management plan Presented by

Management of Asthma, asthma management plan • Presented by: Dr. Eman Fadhel • • PGY 4 Family Medicine Supervised by Dr. Hassan Yousef • 2/10/2019

Objectives - Reduce asthma morbidity and mortality - Improve quality management of asthma - Standardize the management of asthma - Reduce hospital admission due asthma exacerbation

Updates - GINA guideline no longer recommends treatment with SABA alone 1 - Does not protect from severe exacerbations 2 - Frequent use of SABA increase risk of exacerbation 3 - provides short term relief only
 is associated with increase risk of severe")
Updates - overuse of SABA (>=3 canisters/year) is associated with increase risk of severe exacerbations. - Dispensing >=12 canisters/year is associated with increased risk of asthma related death

Updates - All Adults/Adolescents with asthma should receive daily low dose ICS treatment to reduce risk of exacerbation.

• ICS markedly reduces the frequency and severity of asthma symptoms. • Reduce the risk of exacerbation or dying from asthma

- For mild asthma: as needed low dose ICSformoterol, or low dose ICS taken whenever SABA is taken - Maintenance and reliever treatment with ICSformoterol with low dose budesonide-formoterol

Symptoms -Wheezing -SOB -Chest tightness -Cough Symptoms vary in intensity

Factors May Trigger or Worsen Asthma • • • Viral or bacterial infections Allergens (dust mite, pollens, cockroach's) Smoking Exercise Stress Drugs: beta blockers, aspirin, NSAIDs

- GINA recommends that every adult and adolescent with asthma should receive ICS containing controller medication to reduce their risk of serious exacerbations, even in patients with infrequent symptoms. Every patient with asthma should have a reliever inhaler. - Treat modifiable risk factors and comorbidities - Use non pharmacological therapies and strategies as appropriate

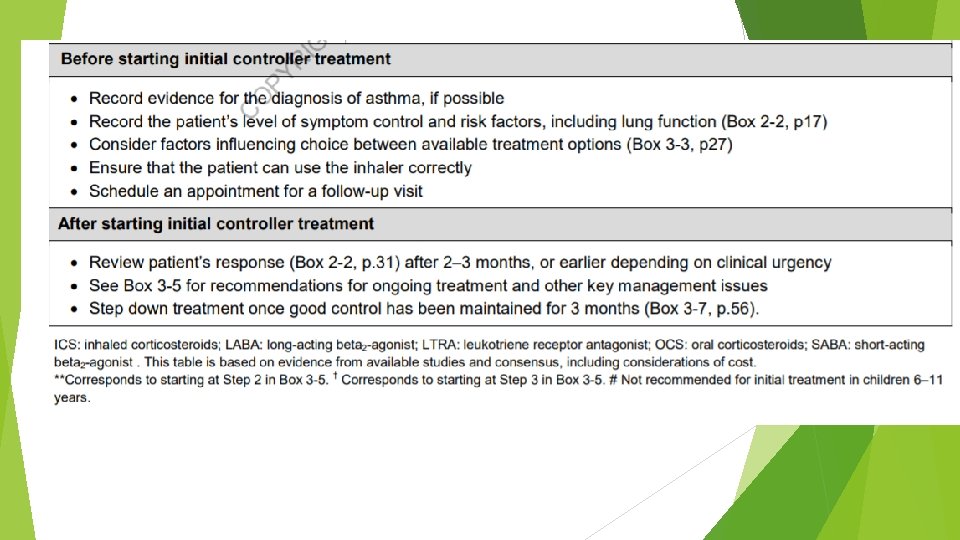
starting treatment - For best outcomes, ICS containing treatment should be initiated as soon as possible after the diagnosis of asthma is made - Low dose of ICS reduces asthma hospitalizations and death.

Low dose ICS is very effective in: - Preventing severe exacerbations. Reducing symptoms. Improving lung function. Preventing exercise induced bronchoconstriction. even in patients with mild asthma

- Early treatment with low dose ICS leads to better lung function than if symptoms have been present for more than 2 -4 years. - Patients not taking ICS who experience a severe exacerbation have lower long term lung function.

Occupational Asthma Early removal from exposure and early treatment increase the probability of recovery

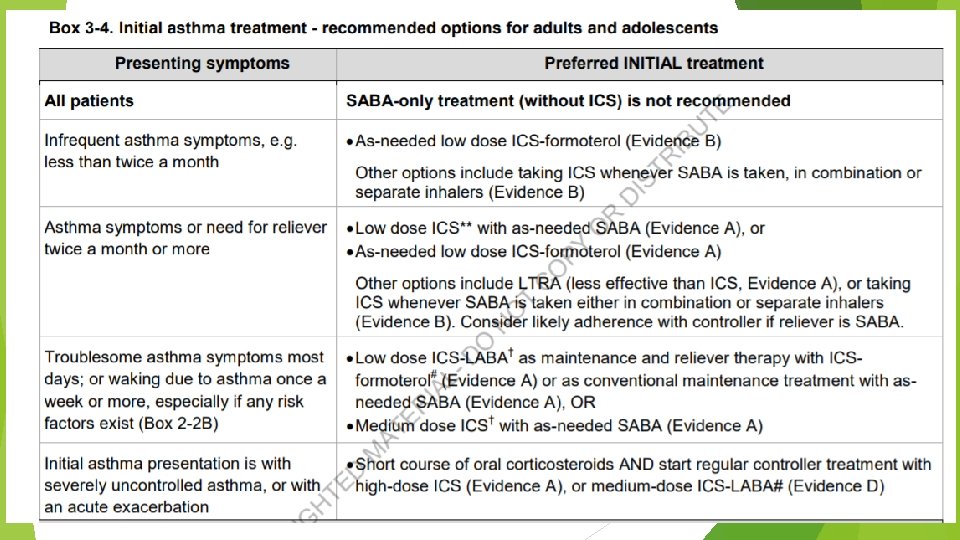
- For most asthma patients, controller treatment can be started with either as needed low dose ICS- formoterol, or low dose ICS whenever SABA is taken, or with regular daily low dose ICS

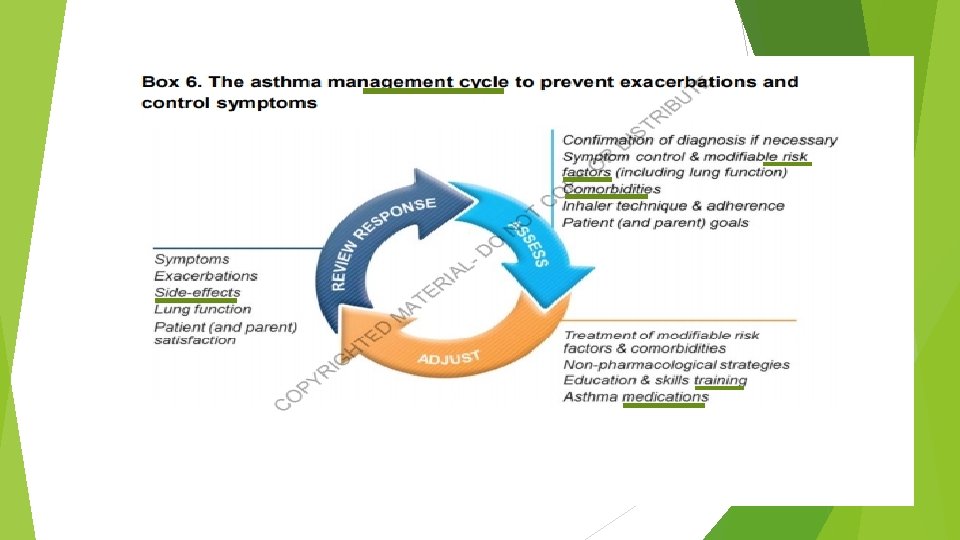
Adults & adolescents 12+ years Confirmation of diagnosis if necessary Symptom control & modifiable risk factors (including lung function) Comorbidities Inhaler technique & adherence Patient goals Personalized asthma management: Assess, Adjust, Review response Symptoms Exacerbations Side-effects Lung function Patient satisfaction Treatment of modifiable risk factors & comorbidities Non-pharmacological strategies Education & skills training Asthma medications STEP 4 Asthma medication options: Adjust treatment up and down for individual patient needs STEP 2 PREFERRED CONTROLLER STEP 1 to prevent exacerbations and control symptoms As-needed low dose ICS-formoterol * Other controller options PREFERRED RELIEVER Other reliever option STEP 3 Low dose ICS taken whenever SABA is taken † Daily low dose inhaled corticosteroid (ICS), or as-needed low dose ICS-formoterol * Leukotriene receptor antagonist (LTRA), or low dose ICS taken whenever SABA taken † As-needed low dose ICS-formoterol * Low dose ICS-LABA Medium dose ICS-LABA STEP 5 High dose ICS-LABA Refer for phenotypic assessment ± add-on therapy, e. g. tiotropium, anti-Ig. E, anti-IL 5/5 R, anti-IL 4 R Add low dose High dose Medium dose OCS, but ICS, add-on ICS, or low consider tiotropium, or dose add-on LTRA # side-effects ICS+LTRA # As-needed low dose ICS-formoterol ‡ As-needed short-acting β 2 -agonist (SABA) * Off-label; data only with budesonide-formoterol (bud-form) † Off-label; separate or combination ICS and SABA inhalers ‡ Low-dose ICS-form is the reliever for patients prescribed bud-form or BDP-form maintenance and reliever therapy # Consider adding HDM SLIT for sensitized patients with allergic rhinitis and 1 FEV >70% predicted

Step 1 is for patients with symptoms less than twice a month, and with no exacerbation risk factors As-needed low dose ICS-formoterol Evidence Indirect evidence from as needed low dose budesonide-formoterol of large reduction in severe exacerbations vs SABA-only treatment in patients eligible for Step 2 therapy Values and preferences High importance given to reducing exacerbations High importance given to poor adherence with regular ICS in patients with infrequent symptoms, which would expose them to risks of SABA-only treatment.

Low dose ICS taken whenever SABA is taken Values and preferences High importance given to preventing severe exacerbations Small differences in symptom control and the inconvenience of needing to carry two inhalers Combination ICS-SABA inhalers are available in some countries, but approved only for maintenance use Daily ICS is no longer listed as a Step 1 option This was included in GINA 2014, but with high probability of poor adherence Now replaced by more feasible as-needed controller options for Step 1

Adults & adolescents 12+ years Confirmation of diagnosis if necessary Symptom control & modifiable risk factors (including lung function) Comorbidities Inhaler technique & adherence Patient goals Personalized asthma management: Assess, Adjust, Review response Symptoms Exacerbations Side-effects Lung function Patient satisfaction Treatment of modifiable risk factors & comorbidities Non-pharmacological strategies Education & skills training Asthma medications STEP 4 Asthma medication options: Adjust treatment up and down for individual patient needs STEP 2 PREFERRED CONTROLLER STEP 1 to prevent exacerbations and control symptoms As-needed low dose ICS-formoterol * Other controller options PREFERRED RELIEVER Other reliever option STEP 3 Low dose ICS taken whenever SABA is taken † Daily low dose inhaled corticosteroid (ICS), or as-needed low dose ICS-formoterol * Leukotriene receptor antagonist (LTRA), or low dose ICS taken whenever SABA taken † As-needed low dose ICS-formoterol * Low dose ICS-LABA Medium dose ICS-LABA STEP 5 High dose ICS-LABA Refer for phenotypic assessment ± add-on therapy, e. g. tiotropium, anti-Ig. E, anti-IL 5/5 R, anti-IL 4 R Add low dose High dose Medium dose OCS, but ICS, add-on ICS, or low consider tiotropium, or dose add-on LTRA # side-effects ICS+LTRA # As-needed low dose ICS-formoterol ‡ As-needed short-acting β 2 -agonist (SABA) * Off-label; data only with budesonide-formoterol (bud-form) † Off-label; separate or combination ICS and SABA inhalers ‡ Low-dose ICS-form is the reliever for patients prescribed bud-form or BDP-form maintenance and reliever therapy # Consider adding HDM SLIT for sensitized patients with allergic rhinitis and 1 FEV >70% predicted
 Regular low dose ICS with as-needed SABA Evidence Studies showed that")
Step 2 1) Regular low dose ICS with as-needed SABA Evidence Studies showed that low dose ICS substantially reduces risks of severe exacerbations, hospitalizations and death Serious exacerbations halved even in patients with symptoms 0 -1 days per week Improved symptom control and reduced exercise-induced bronchoconstriction Values and preferences Preventing asthma deaths and severe exacerbations. However, poor adherence is common in mild asthma in the community, and that this would expose patients to the risks of SABA-only treatment
 As-needed low dose ICS-formoterol (off-label; all evidence with budesonide-formoterol) Evidence severe exacerbations vs")
2) As-needed low dose ICS-formoterol (off-label; all evidence with budesonide-formoterol) Evidence severe exacerbations vs daily low dose ICS + as-needed SABA 64% reduction in severe exacerbations vs SABA-only treatment Symptoms reduced; one study showed reduced exercise-induced bronchoconstriction Values and preferences High importance was given to preventing severe exacerbations, avoiding need for daily ICS in patients with mild or infrequent symptoms, and safety of as-needed ICS-formoterol in maintenance and reliever therapy, with no new safety signals Lower importance given to small non-cumulative differences in symptom control and lung function compared with daily ICS Makes use of normal patient behaviour (seeking symptom relief) to deliver controller

Adults & adolescents 12+ years Confirmation of diagnosis if necessary Symptom control & modifiable risk factors (including lung function) Comorbidities Inhaler technique & adherence Patient goals Personalized asthma management: Assess, Adjust, Review response Symptoms Exacerbations Side-effects Lung function Patient satisfaction Treatment of modifiable risk factors & comorbidities Non-pharmacological strategies Education & skills training Asthma medications STEP 4 Asthma medication options: Adjust treatment up and down for individual patient needs STEP 2 PREFERRED CONTROLLER STEP 1 to prevent exacerbations and control symptoms As-needed low dose ICS-formoterol * Other controller options PREFERRED RELIEVER Other reliever option STEP 3 Low dose ICS taken whenever SABA is taken † Daily low dose inhaled corticosteroid (ICS), or as-needed low dose ICS-formoterol * Leukotriene receptor antagonist (LTRA), or low dose ICS taken whenever SABA taken † As-needed low dose ICS-formoterol * Low dose ICS-LABA Medium dose ICS-LABA STEP 5 High dose ICS-LABA Refer for phenotypic assessment ± add-on therapy, e. g. tiotropium, anti-Ig. E, anti-IL 5/5 R, anti-IL 4 R Add low dose High dose Medium dose OCS, but ICS, add-on ICS, or low consider tiotropium, or dose add-on LTRA # side-effects ICS+LTRA # As-needed low dose ICS-formoterol ‡ As-needed short-acting β 2 -agonist (SABA) * Off-label; data only with budesonide-formoterol (bud-form) † Off-label; separate or combination ICS and SABA inhalers ‡ Low-dose ICS-form is the reliever for patients prescribed bud-form or BDP-form maintenance and reliever therapy # Consider adding HDM SLIT for sensitized patients with allergic rhinitis and 1 FEV >70% predicted
 Evidence reduced")
Low dose ICS taken whenever SABA taken (off-label, separate or combination inhalers) Evidence reduced exacerbations compared with SABA-only treatment in adults, with combination ICS-SABA in children/adolescents, with separate inhalers fewer exacerbations compared with maintenance ICS Values and preferences High importance given to preventing severe exacerbations Lower importance given to small differences in symptom control and the inconvenience of needing to carry two inhalers Combination ICS-SABA inhalers are available in some countries, but approved only for maintenance use Another option: leukotriene receptor antagonist (less effective for exacerbations)

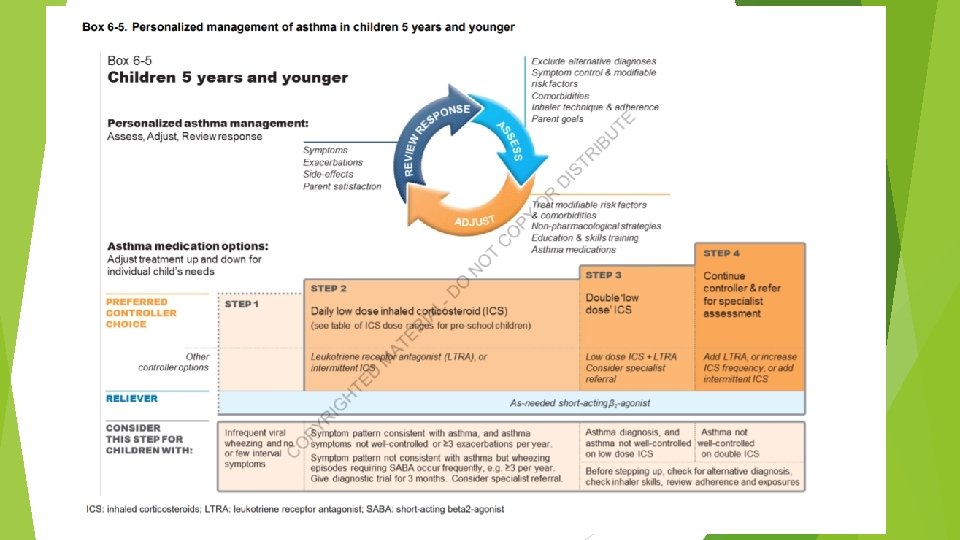
Children 6 -11 years Confirmation of diagnosis if necessary Symptom control & modifiable risk factors (including lung function) Comorbidities Inhaler technique & adherence Child and parent goals Personalized asthma management: Assess, Adjust, Review response Symptoms Exacerbations Side-effects Lung function Child and parent satisfaction Treatment of modifiable risk factors & comorbidities Non-pharmacological strategies Education & skills training Asthma medications STEP 4 Asthma medication options: Adjust treatment up and down for individual child’s needs STEP 3 STEP 2 PREFERRED CONTROLLER to prevent exacerbations and control symptoms Other controller options RELIEVER STEP 1 Low dose ICS taken whenever SABA taken*; or daily low dose ICS Daily low dose inhaled corticosteroid (ICS) (see table of ICS dose ranges for children) Low dose ICS-LABA, or medium dose ICS Leukotriene receptor antagonist (LTRA), or low dose ICS taken whenever SABA taken* Low dose ICS+LTRA As-needed short-acting β 2 -agonist (SABA) * Off-label; separate ICS and SABA inhalers; only one study in children Medium dose ICS-LABA Refer for expert advice High dose ICSLABA, or addon tiotropium, or add-on LTRA STEP 5 Refer for phenotypic assessment ± add-on therapy, e. g. anti-Ig. E Add-on anti-IL 5, or add-on low dose OCS, but consider side-effects

Step 1 Low dose ICS whenever SABA taken, or daily low dose ICS Step 2 Preferred controller is daily low dose ICS Other controller options include as-needed low dose ICS taken whenever SABA is taken maintenance and reliever therapy with low dose budesonide-formoterol in children 4 -11 years reduced exacerbations by 70 -79% compared with ICS and ICS-LABA Step 3 Low dose ICS-LABA or medium dose ICS are ‘preferred’ controller treatments Step 4 Medium dose ICS-LABA, but refer for expert advice
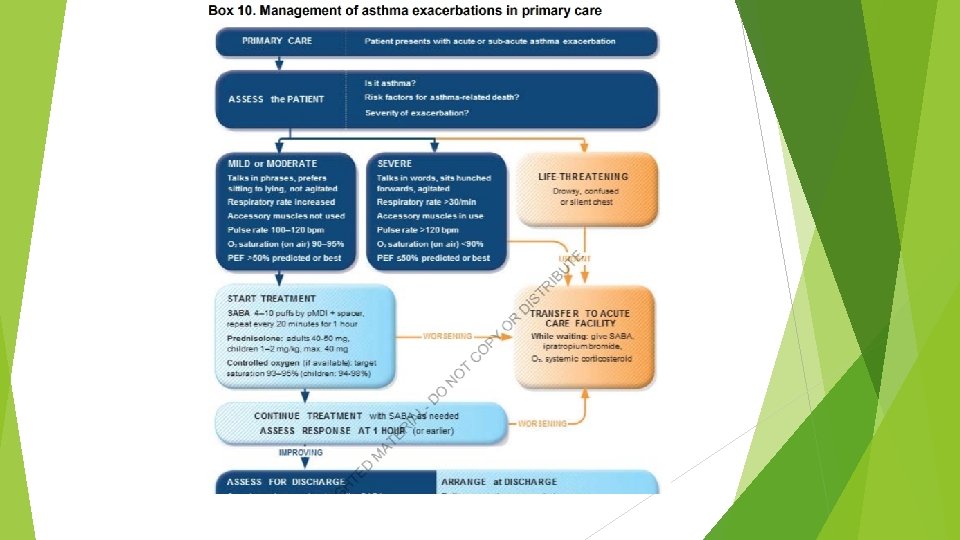

A 32 -year-old man with a long history of asthma came to the emergency department 2 hours ago with an acute asthma exacerbation. He was given a dose of intravenous methylprednisolone and received continuous albuterol nebulizer treatments. The patient explains that he is recovering from an upper respiratory infection. His past medical history is otherwise insignificant. He is afebrile, blood pressure is 110/70 mm Hg, pulse is 120/min, and respirations are 28/min. The patient is using accessory muscles of respiration and appears anxious and restless. Examination shows markedly diminished breath sounds bilaterally with minimal wheezing. He is unable to lie supine. Chest x-ray reveals hyperinflated lungs and no infiltrates. Complete blood count shows a total white blood cell count of 11, 000/µL. Results of arterial blood gas analysis on 3 L/min oxygen are as follows: Which of the following is the best next step in management of this patient? p. H 7. 32 65 p. O 2 mm Hg 50 p. CO mm 2 Hg
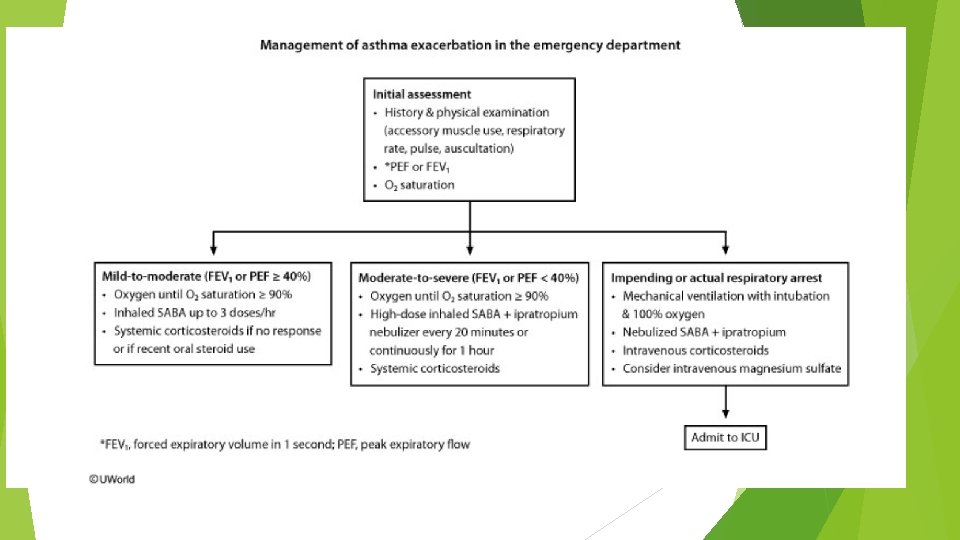

In patients with acute asthma exacerbation, an elevated/normal arterial partial pressure of carbon dioxide suggests decreased respiratory drive (likely due to respiratory muscle fatigue) and impending respiratory failure. In these patients, treatment involves endotracheal intubation and mechanical ventilation

• A 25 -year-old woman with a history of asthma comes to the emergency department with sudden-onset, severe shortness of breath and wheezing. She recently had a minor respiratory infection. On examination, she is using accessory muscles of respiration but is able to speak in full sentences. The patient is treated with continuous albuterol nebulization and intravenous methylprednisolone. Her condition improves within 6 hours. The next morning, she describes her shortness of breath as "mild" but complains of muscle weakness. On examination, she has difficulty lifting her arms over head and mild hand tremors. Her vital signs are stable. • Which of the following is the best next step in management of this patient?

• Chext x ray • Peak expiratory flow rate • Serum electrolyte panel • Serum TSH

• Inhaled albuterol and systemic steroids are appropriate treatments for acute asthma attacks. Patients on high doses of beta-2 agonists may develop hypokalemia, which may present with muscle weakness, arrhythmias, and electrocardiogram abnormalities. Other common side effects of beta-2 agonists include tremor, palpitations, and headache.
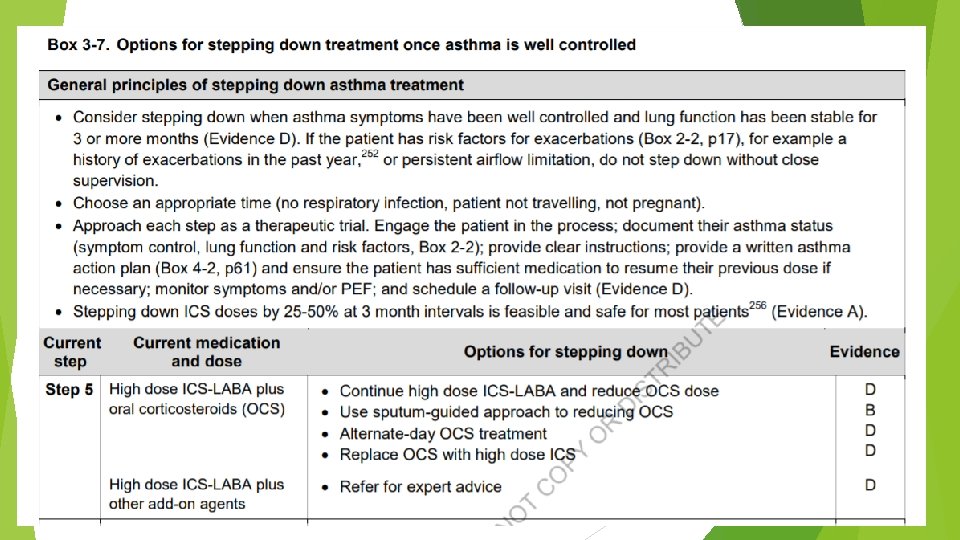
- Slides: 40