Antepartum Fetal Health Assessment Associate Professor Dr Atiwut


 Contraction stress test (CST) Fetal")




 Hypoxemia DFIU Uterine")



 Principle Indication/ Method Interpretation Contraindication FHR depend on the 1.")
 2. Variability 3. Abnormal pattern")









 Principle Uterine contraction hypoxemia FHR Indication/ Method Contraindication Nonreactive NST")


 CST")
 CST")








")







 • Ratio >3 at GA > 37")






- Slides: 67
Antepartum Fetal Health Assessment Associate Professor Dr Atiwut Kamudhamas Department of Obstetrics and Gynecology Faculty of Medicine Thammasat University
Definition Fetal health assessment during the viable period before true labor pain
Assessment methods Fetal movement count Non stress test (NST) Contraction stress test (CST) Fetal biophysical profile Doppler flow measurement Hormonal assay: Estriol, h. PL
Fetal movement count
Fetal movement count Principle Indication/ Contraindication All patients in 3 rd trimester of pregnancy Method Interpretation Movement 1. Daily fetal See a doctor when alarming signal movement< 10 record times/ day Decrease fetal movement 24 hr 2. Cardiff count-to then stop -10 No contraindication movement 8 hr before death
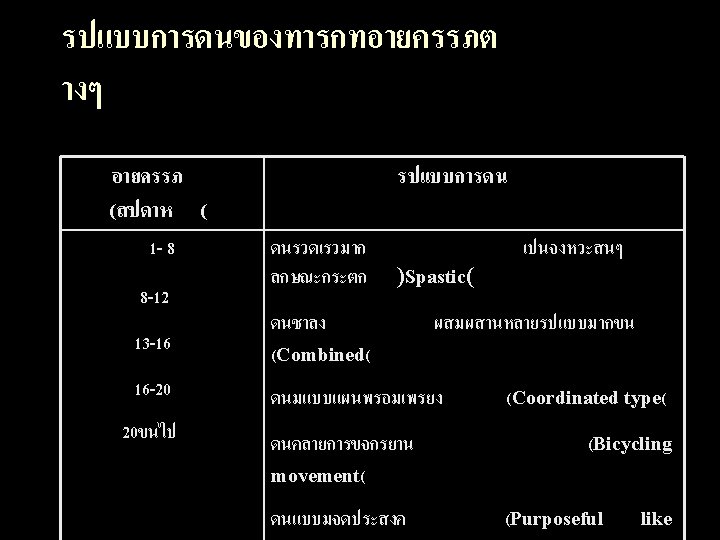
Fetal behavioral states – – State 1 F : quiet sleep State 2 F : active sleep (rapid eye movement) State 3 F : quiet awake State 4 F : active awake (FHR acceleration + vigorous body movement + REM)
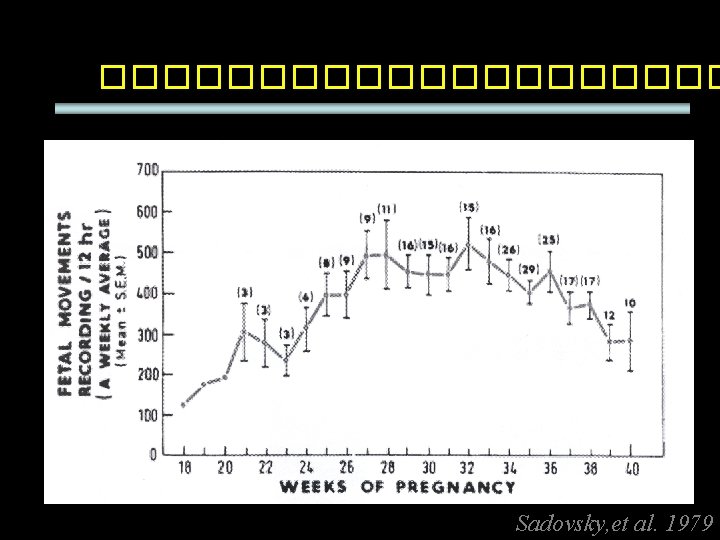
Factor affecting fetal movement GA Sleep awake cycle (20 -40 min) Hypoxemia DFIU Uterine contraction Induction of labor Drug (alcohol, smoking, steroid) Chromosome abnormalities External stimuli Level of plasma glucose
Factor affecting perception of movement Placental site Amniotic fluid volume GA Obesity Anxiety
Management NST
Non stress test
Non stress test (NST) Principle Indication/ Method Interpretation Contraindication FHR depend on the 1. Abnormal fetal balance between movement count sympathetic and 2. U/D (DM, HT, parasympathetic thyrotoxicosis) activity 3. Postterm Movement 4. IUGR Sympathetic FHR 5. PROM Hypoxia 6. Twins Parasym FHR 7. Preeclampsia Electronic fetal cardiotocography Semi-fowler (beware complication from supine hypotensive syndrome) 1. Reactive 2. Non reactive
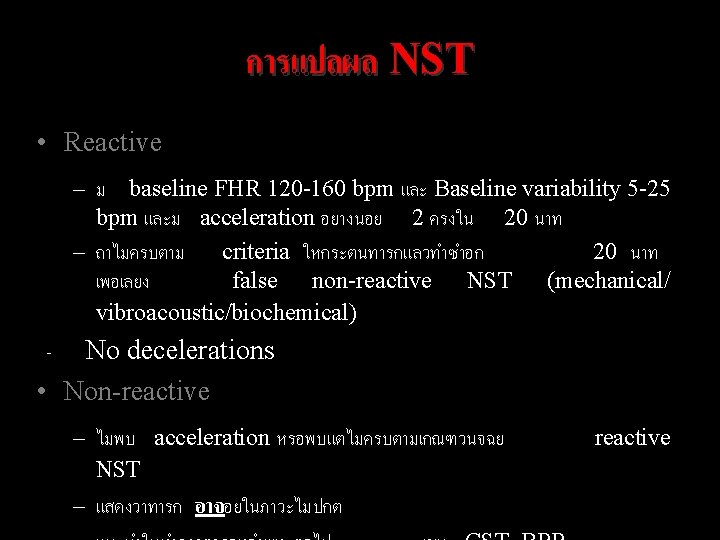
Reading NST Findings: 1. Baseline FHR (120 -160 bpm) 2. Variability 3. Abnormal pattern 4. Periodic change 4. 1 Acceleration 4. 2 Deceleration 5. Uterine contraction
Fetal heart rate acceleration Increase FHR ≥ 15 beats per min and Persist > 15 sec 32>wks' : >10 bpm above baseline for 10<sec 32<wks' : >15 bpm above baseline for 15 <sec
Reactive NST
Non-reactive NST
Reactive NST
Non-reactive NST with spontaneus deceleration
Non-reactive NST
Management Reactive F/U q 1 wk F/U 2 -3 times/wk in DM type B-H, postterm, IUGR Nonreactive CST, BPP
Efficacy and effectiveness High false positive Low positive predictive value High negative predictive value False negative NST 3. 7% False positive NST 50% Negative predictive valve 92% Positive predictive valve 22%
Contraction stress test
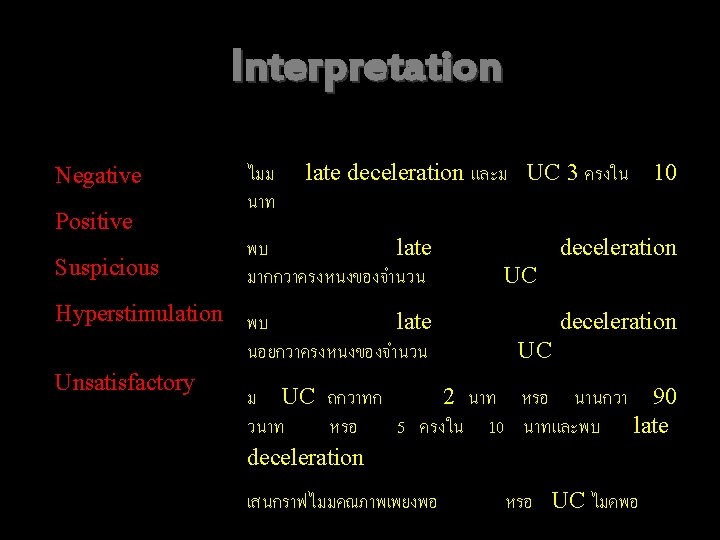
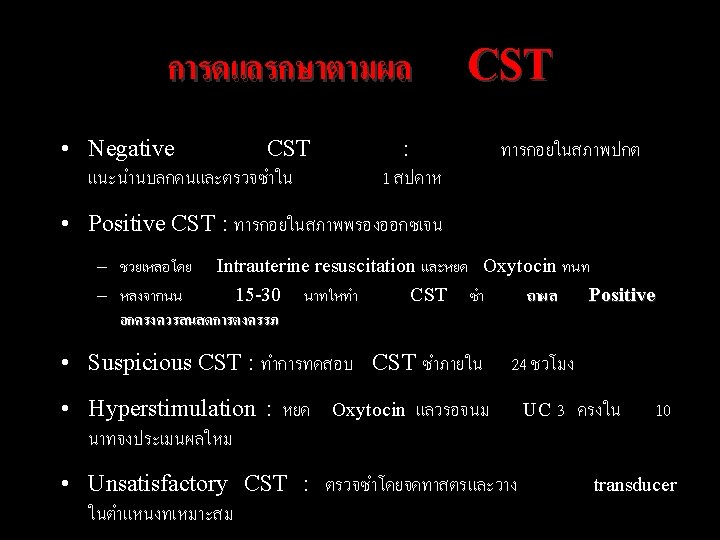
Contraction stress test (CST) Principle Uterine contraction hypoxemia FHR Indication/ Method Contraindication Nonreactive NST 1. OCT 2. Nipple Contraindication stimulation test (See next slide) Interpretation 1. Negative 2. Positive 3. Suspicious 4. Hyperstimulation 5. Unsatisfactory
Contraindications 1. Previous premature labour 2. Previous uterine surgery 3. Previous classical C/S 4. PROM 5. Placenta previa 6. Hydramnios 7. Incompetent cervix 8. Multiple gestation
Methods 1. oxytocin infusion – Start: 0. 5 m. U / min – Titrate: increase 1 m. U every 15 min . 2 Nipple Stimulation Goal: 3 contractions in 10 min Duration 40 -60 sec
Negative (reactive) CST
Negative (reactive) CST
Negative reactive CST
Negative nonreactive CST
Positive nonreactive CST
Hyperstimulation CST
Negative CST
Unsatisfactory CST
Unsatisfactory CST
Efficacy False negative CST 0. 1% False positive CST 50%
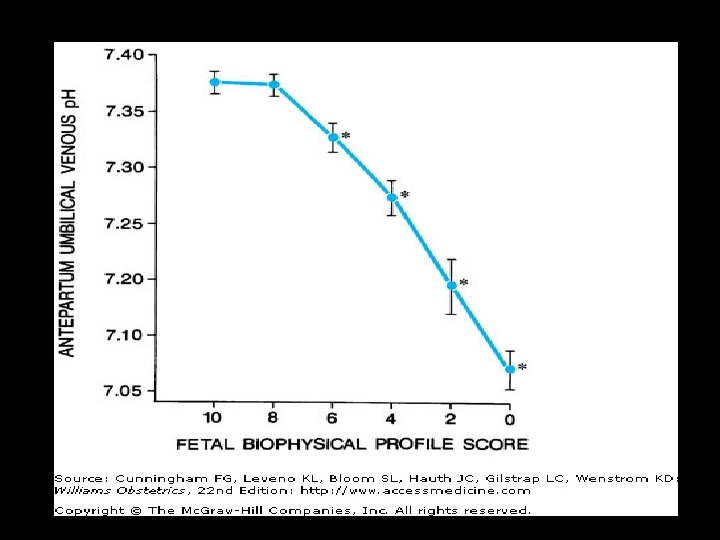
Fetal biophysical profile (BPP)
BPP Principle Indication/ Method Contraindication US + NST Nonreactive NST 1. NST with contraindication of 2. Real time US CST Back up surveillance Interpretation American College of Obstetricians and Gynecologists (1999)
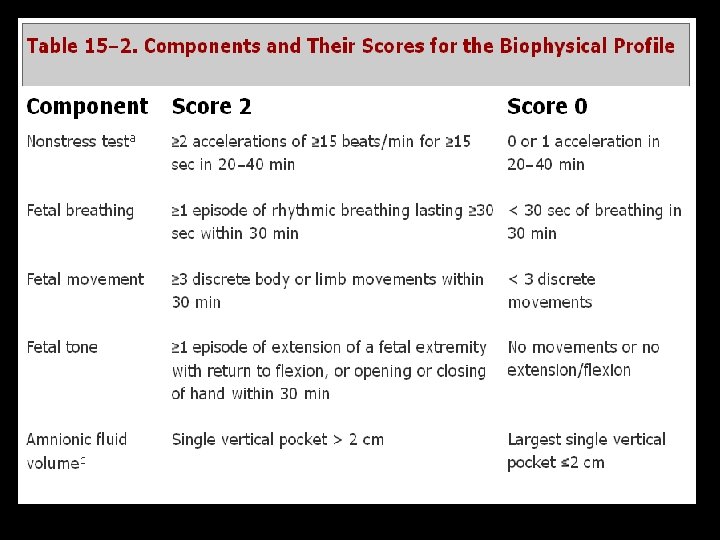
BPP scoring
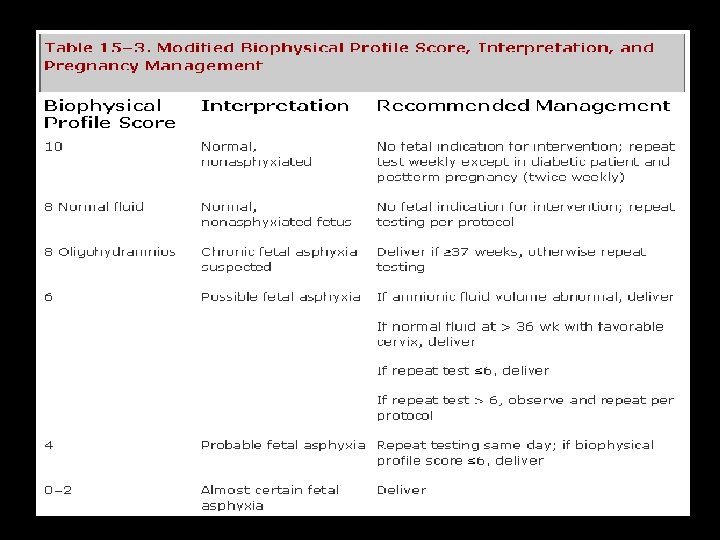
Interpretation and management
Efficacy • False negative BPP 0. 007% • False positive BPP 1%
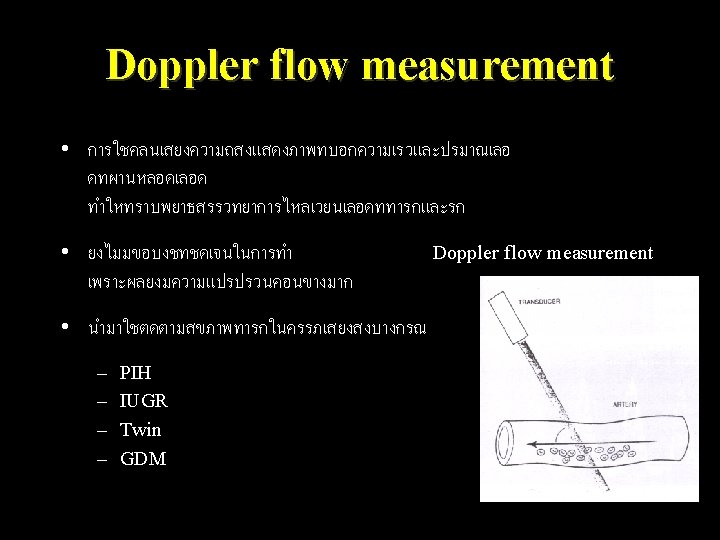
Color Doppler measurement
Vessels • • Umbilical artery Renal artery Uterine artery Middle cerebral artery
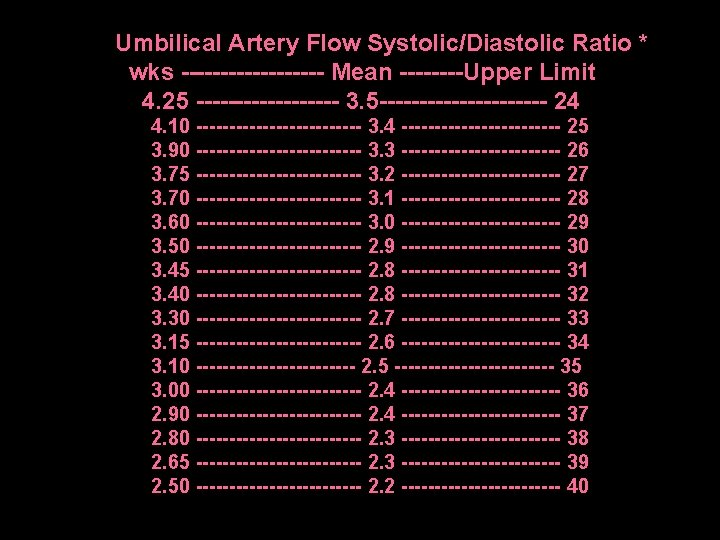
Systolic/Diastolic ratio = A/B Resistance index = A-B/A Pulsatility index = A-B/mean
Interpretation • Umbilical systolic-diastolic ratio (S/D ratio) • Ratio >3 at GA > 37 weeks = abnormal • More severe – Absent end-diastolic flow – Reversed end-diastolic flow UPI ↓ ������� ↓ ����� Diastolic↓
Normal
Absent end diastolic flow
Reverse diastolic flow
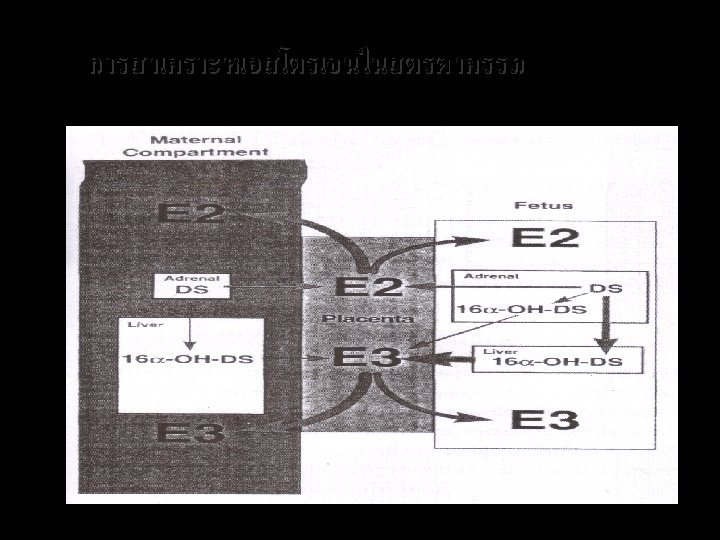
Hormonal assay
End of the session Thank you for your attention