Amenorrhoea Dr Khaldoun Khamaiseh MRCP FRCOG Consultant Obstetrician

Amenorrhoea Dr Khaldoun Khamaiseh MRCP FRCOG Consultant Obstetrician & Gynecologist and Reproductive endocrinologist
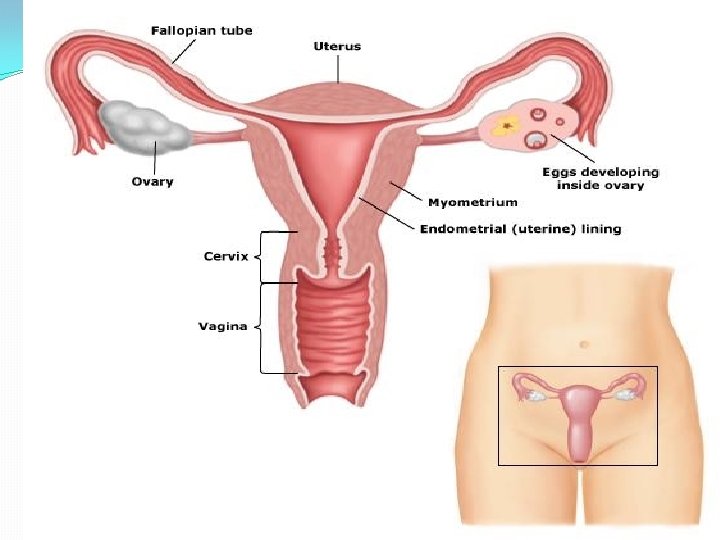
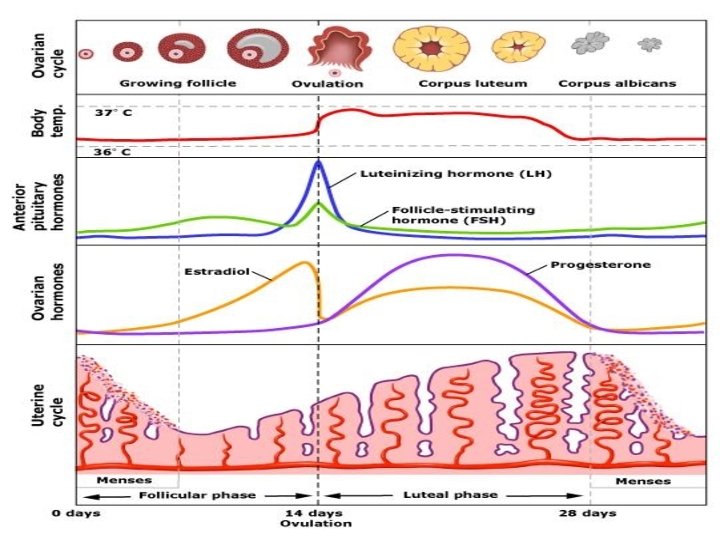

physiology � Menarche occur between 11 -14 years of age � Regular menstruation indicates that the hypothalamo–pituitary–ovarian axis is intact � Cycles between 23 and 35 days indicates ovulation. � The luteal phase is fixed(14 days) and the follicular phase is variable

Primary amenorrhoea � Diagnosed when there is amenorrhoea in girls up to age of 14 years of age who have no secondary sexual characteristics. � Or, when there is amenorrhoea in girls up to age of 16 yrs with normal secondary sexual characteristics.

Secondary amenorrhoea � Defined as absent periods for at least six months in a woman who has previously had regular periods

Primary amenorrhoea � hirsutism � menopausal symptoms � headache or visual disturbance – suggestive of CNS tumor such as craniopharyngioma � anosmia – one of the causes is Kallmans syndrome � chronic systemic illness, chemotherapy, radiotherapy

Causes of primary amenorrhoea � Chromosomal : Turner, fragile X syndrome � Hypothalamic: Kallman’s syndrome � Pituitary: Hypogonadotrohic hypogonadism (Levi Lorraine syndrome) Congenital uterine hypoplasia/Aplasia (Meyer Rokitansky Kuster Hauser Syndrome) � Anorexia nervosa �

� Testicular feminization syndrome: XY male karyotype, normal breast development, short vagina, absent uterus, gonads should be removed agfter puberty to prevent dysgerminoma � Late onset congenital Adrenal hyperplasia: Severe hirsutism and amenorrhoea

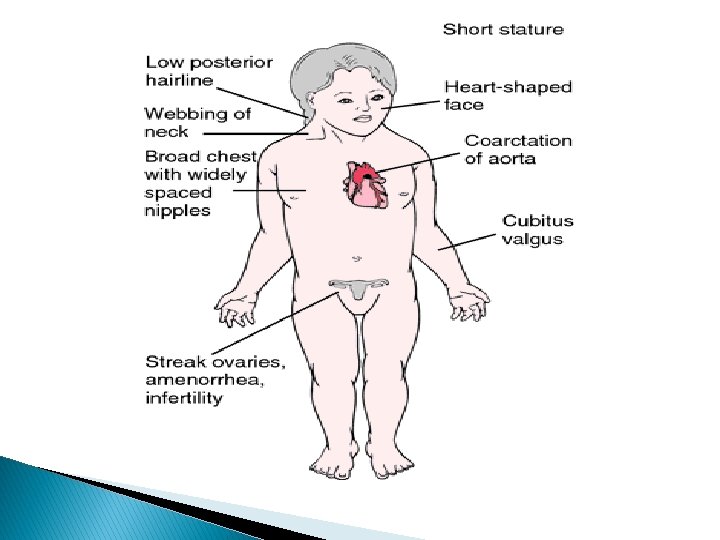
Turner syndrome 45 XO

 Hypothalamic 35% (Hyperprolactinaemia,")
Secondary amenorrhoea/Causes � Ovarian � in origin 40% (PCOS, ovarian failure) Hypothalamic 35% (Hyperprolactinaemia, Sheehan’s, pituitary necrosis due severe PPH) � Uterine in origin. 5% (Asherman’s syndrome) � Iatrogenic � Severe systemic illness: Renal failure, Endocrine

Asherman's syndrome � Secondary amenorrhoea can follow destruction and scarring of the endometrium and/or cervical canal resulting from postpartum curettage. � Typically, multiple synechiae may be seen on hysteroscopy. � Asherman's syndrome has been reported following generalised pelvic infection. Treatment � Hysteroscopic lysis of adhesions. Up to 80% of patients can conceive following treatment but pregnancy is frequently complicated by premature labour, abnormal placentation (accrete/praevia) and postpartum haemorrhage.

Medications � Antipsychotics � Chemotherapy � Radiotherapy � Illicit drug use e. g. cocaine and opiates

Evaluating amenorrhoea � Primary or secondary, � Age of the woman. � take a history, examine then requesting the appropriate investigations � Rule out physiological cause: Pregnancy , Lactation and menopause.

Secondary amenorrhoea � Irregular menstrual cycles – associated with polycystic ovary syndrome � malaise, fatigue, anorexia, weight loss – may be due to chronic illness � headaches – may be suggestive of CNS tumor � galactorrhoea – may be due to prolactinoma

Secondary amenorrhoea � H/O postpartum hemorrhage – may be associated with Sheehans syndrome � H/O dilataion and curretage – may be associated with Ashermans syndrome � Drugs: Contraception, antidepressants and antipsychotics, Chemotherapy

Examination of an adolescent with primary amenorrhoea � General Weight, height, body mass index (BMI) Blood pressure, thyroid, � Dysmorphic signs � Tanner staging: Breast, axillary and pubic hair stages

Examination � The woman's height and weight should be recorded. � Raised BMI is associated with polycystic ovarian syndrome � Reduced BMI with stress, anorexia nervosa.

� Male pattern baldness and features of virilisation may be due to androgen secreting tumors of the ovary. � Assess for galactorrhoea by doing a breast examination. � Look out for features of hypothroidism.

� Abdomen/pelvis � � Mass arising from pelvis Perineum Inspection Under anaesthesia, vaginoscopy, hysteroscope or cystoscope,

Investigations � Pregnancy � FSH & LH. test

� PCOS � TURNER SYNDROME � ovarian failure � Pituitary failure, anorexia

� Prolactin levels � Testosterone levels , DHEA & Androstenodione � Estrogen and progesterone challenge tests. � Ultrasound and MRI � hysteroscopy and laparoscopy � Karyotyping in premature ovarian failure,

Haematocolpos

Treatment according to cause � HRT. Estrogen and progesterone � Dopamine agonists: cabergoline, bromocriptine, � Surgery: Reconstructive, adhesiolysis

Thank you

1 -Menarche is defined as A- first pregnancy in a woman's life. B- Last period in the woman's life C- First period in woman's life D- Painful periods E- Heavy periods

2 - Follicle stimulating hormone is � A- protein � B- Steroid � C- Lipid � D- Glycoprotein � E- Glycolipid

3 - A 32 year old lady P 2+1 has no period for 9 months, she is not pregnant, but has galactorrhoea, most common cause is: A- Ovarian failure B- Addisons disease C- Hyperthyroidism D- Hyperprolactinaemia E- Diabetes

4 - Ovarian failure is associated with A- High estrogen B- Low FSH and LH C- High progesterone D- High FSH and LH E- Non of the above

5 - A 49 -year-old woman approaches you in the clinic as she has been having regular, troublesome hot flushes for past 6 months. Her last period was 2 weeks ago. Which is the most suitable type of HRT to start her on? A- Continuous combined HRT B- Estrogen only HRT - oral tablets C- Estrogen only HRT - patches D- Sequential combined HRT E- Tibolone

6 - Hyperprolactinemia is associated with all except a. chronic renal failure. b. Galactorrhea. c. Cimitidine therapy. d. Methyldopa therapy. e. Adrenogenital syndrome.

7 - Recognised causes of raised FSH a. Polycystic ovarian syndrome b. Anorexia nervosa c. Premature ovarian failure d. Kallman's syndrome e. All of the above

8 - Concerning the menstrual cycle: New endometrial growth starts during menstruation b- Ovulation coincides with LH peak - Menstruation occurs following estrogen withdrawal d- Is not ovualtory if the cycle is short s always prolonged if high prolactin level is present �

9 - Premature ovarian failure a. The incidence is 5% b. It may be associated with hypothyroidism c. Ovarian biopsy is essential to confirm the diagnosis d. Spontaneous pregnancy never occurs e. Primary amenorrhoea occurs in 90% of cases

10 - All the following are features of Turner's syndrome, except a. Cystic hygroma b. Lymphoedema c. Coarctation of the aorta d. Cubitus varus e. kyphoscoliosis

11 - One of the following causes only primary amenorrhoea A- Polycystic ovarian syndrome B- Hyperprolactinaemia C- Mullerian agenesis D- Chemotherapy D-Turner syndrome
 is a cause of primary amenorrhoea, the karyotype")
12 - Testicular fenminization syndrome(Androgen insensitivity) is a cause of primary amenorrhoea, the karyotype is A- XO B- XX C- XY D- XXX E- XXY

13 -Antenatal corticosteroids therapy for fetal pulmonary maturation A- Reduces the incidence of respiratory distress syndrome B- Reduces the incidence of intraventricular hemorrhage C- Used between 26 -34 weeks gestation D- Betamethasone and dexamethasone may be given E- Contraindicated in uncontrolled DM because it causes severe hyperglycemia

14 - In twin to twin transfusion syndrome a. The donar twin develops oligohydramnios and intrauterine growth restriction b. The recipient twin is at more risk of intrauterine fetal death c. Fetal hydrops develops in the donor twin d. Fetoscopic laser ablation is an established treatment e. Should be managed by fetal medicine specialist
- Slides: 42