GYNECOLOGICAL INFECTIONS AND PELVIC INFLAMMATORY DISEASE Khaldoun Khamaiseh






 seen on microscopy (")






— gonorrhea and chlamydia—are the main � Two causes of")







- Slides: 22
GYNECOLOGICAL INFECTIONS AND PELVIC INFLAMMATORY DISEASE Khaldoun Khamaiseh FRCOG MRCP Consultant Obstetrician & Gynecologist
Vulvovaginal infections � Candidiasis � Trichomonas vaginalis � Bacterial vaginosis � Viral disease : Herpes and HPV � Syphilis: very rare now
Clinical approach � History : � physical examination � Investigations
History � Discharge : amount , consistency, colour , Odour � Itching � Vulvovaginal soreness � Vaginal bleeding � Sexual history
Candidiasis risk factors � Pregnancy � Estrogen � Diabetes � Immune treatment deficiency
candidiasis � Presents with severe pruritis � Vulval Soreness � Whitish thick discharge may form a plaque � Painful sexual intercourse
Candidiasis diagnosis � Microscopy � Candida albicans � Yeast (fungus) seen on microscopy ( gram positive) � Can be clutured
Candidiasis/ treatment � Clotrimazole vaginal single dose 500 mg or daily 200 mg for 3 days � Miconazole days � Fluconazole vaginal supp and cream for three 150 mg single dose orally
Trichomoniasis � Caused by protozoa Trichomonas vaginalis: sexually transmitted � causes frothy offensive discharge, � strawbery cervix. � Diagnosed by microscopy see the typical protozoa with flagellum � Metronidazole 500 mg TID for one week
Bacterial vaginosis � Bacterial vaginosis: Thin discharge , sfishy odour, metronidazole 50 mg BD for 1 week or clindamycin oral (30 mg BD for 7 days) or vaginal cream
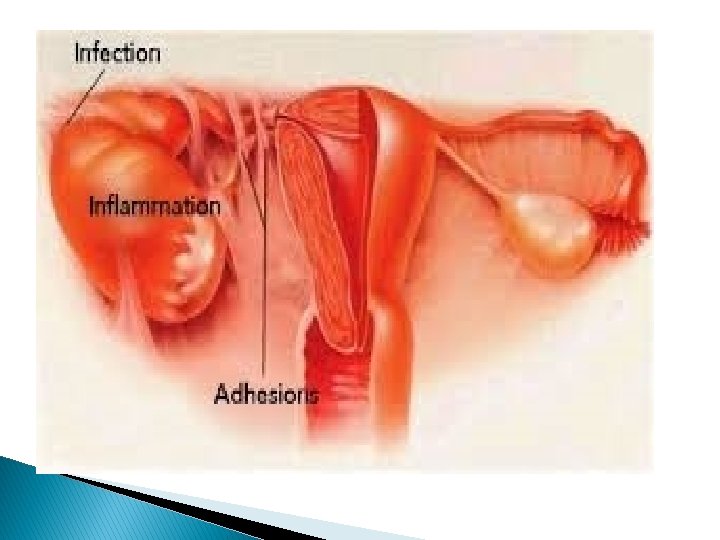
Pelvic inflammatory disease � Ascending: Mostly � Descending rarely � Ascending : Starts as cervicitis , endometrirtis, salpingitis and oophoritis � Usually sexually transmitted , however can be introduced through gyne uterine procedures � Descending : Intra-abdminal sepsis, TB
Causes sexually transmitted infections (STIs)— gonorrhea and chlamydia—are the main � Two causes of PID. � Untreatd it takes from a few days to a few weeks before she developing PID. � PID can be caused by bacterial vaginosis (BV). E coli, anaerobes, mycoplasma. polymicrobial �
presentation � Pelvic pain and abdominal pain � Vaginal discharge � Pyrexia � Painful intercourse � Vaginal bleeding � Acute PID if untreated adequately may progress to chronic PID � Adhesions: Fitz hugh curtiz syndrome
examination � Pyrexia � Tachcardia � Pelvic tenderness � Cervical motion tenderness
Investigations � Swab cervical microscopy and culture, Antigen detection by PCR, Serology � MSU � CRP � CBC � Blood cultures � Imaging: USS, MRI: see mass � Laparoscopy: Hyperemia swollen tubes, abscess, free fluid
treatment � Antibiotics oral vs systemic: Combination � Doxycycline, eryhtromycin for 14 days for chlamydia � Third generation cephalosporin or a penicillin for gonorrhoea: single dose ceftriaxone, cefoxitin � Metronidazole for bacterial vaginosis � Screen and treat partner � Surgery to drain absecss � Rarely salpingo-opherectomy
Long term problems � Infertility � Chronic pelvic pain � Ectopic pregnancy � Hydrosalpinx
Thank you