Acute Pulmonary Oedema David Lightfoot 07 00 at







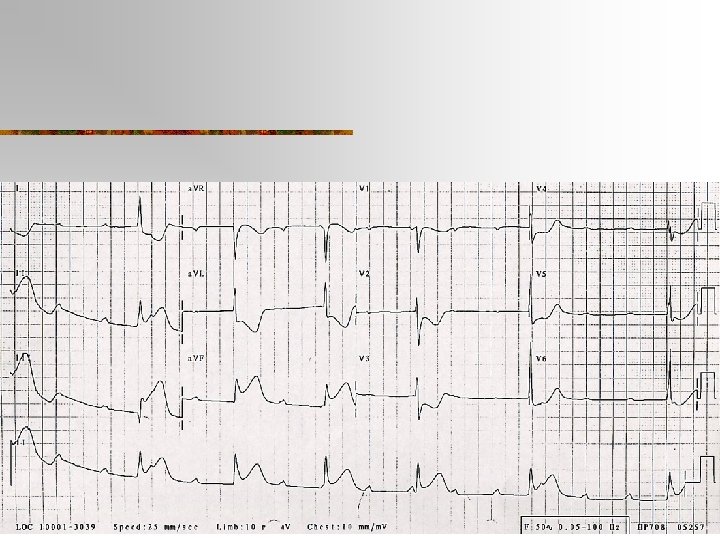
 n n n Myocardial ischaemia/infarction Acute")


 NT-pro BNP(N-terminal pro-BNP) AHF – BNP")













 n n Levosimendan n n Maybe Serelaxin")










- Slides: 39
Acute Pulmonary Oedema David Lightfoot
07. 00 at a Monash. Health ED near you when…. .
Its the bat phone!!!! n n n Hello St Elsewhere’s, Ambulance here. How are you this fine morning? ……. MICA 16 ETA 33 seconds 87 ♂ Extreme dyspnoea HR 100, BP 200/120
What do you get ready? n n n A Frusemide in big doses B Tezosentan- The Rep has just visited C Morphine- Everyone knows it’s great for APO D The Bi. PAP machine E The ETT F Your bag, as it’s almost home time
My suggestions n n n A No Frusemide B GTN C More GTN D The CPAP machine E Aspirin F Your bag as it’s almost home time
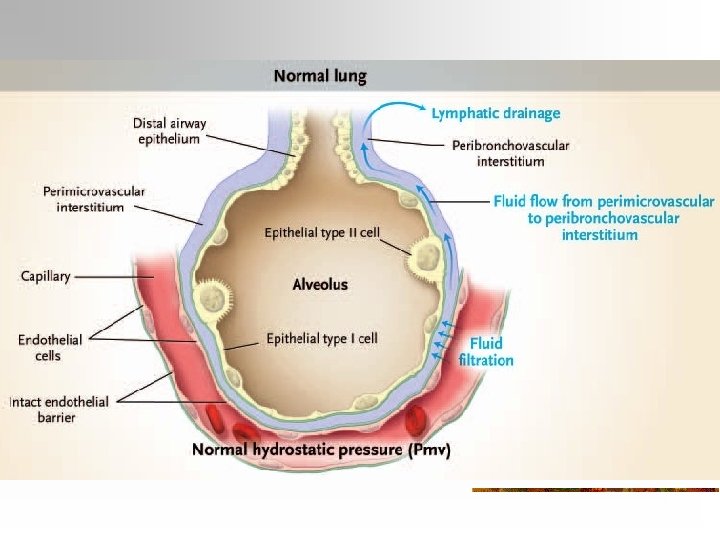
Drowning on dry land! n n Elderly Fluid filled alveolar spaces Lung dysfunction Results in… n n n SOB++ frothy sputum hypoxia diaphoresis often hypertensive
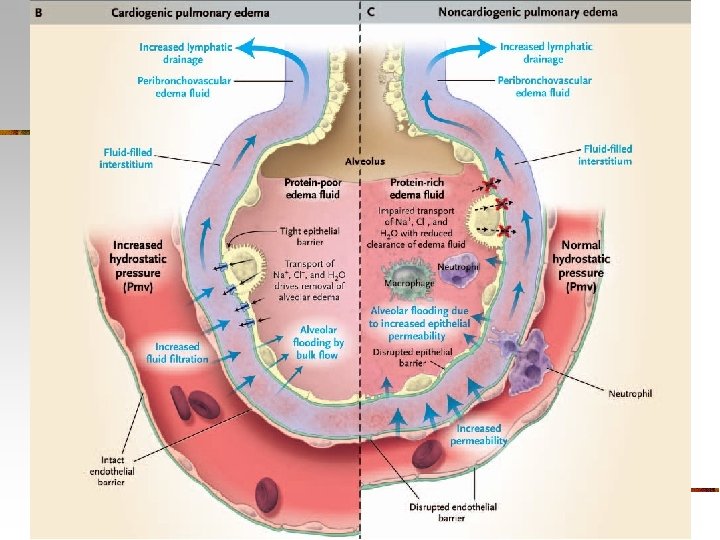
Pathophysiology n n n pulmonary capillary pressure plasma oncotic pressure pulmonary capillary permeability
Causes of Cardiogenic APO (acute decompensated heart failure) n n n Myocardial ischaemia/infarction Acute valvular dysfunction Anaemia Arrhythmias Medication non-compliance Dietary, physical or emotional excess Fluid overload- may be iatrogenic Medication adverse effect (neg inotropy of CCB, BB) Myocarditis Pulmonary embolus Progression congestive cardiac failure
Causes of Non-cardiogenic APO n n n n Airway obstruction Asthma Eclampsia Head Injury, Intracerebral haemorrhage Hyperbaric oxygen treatment Inhalation injury Lung re-expansion. E. g. after treatment of a pneumothorax Near drowning/ cold water immersion Opiates and opiate antagonists (Naloxone and Naltrexone) Pancreatitis Pulmonary embolism (thrombus, fat, amniotic fluid, other) Rapid ascent to high altitude, SCUBA diving Renal/Hepatic failure Sepsis, DIC Shock Toxins
Evaluation n ABC n History n Examination n Investigations
Natriuretic peptides n n BNP (B-type natriuretic peptide) NT-pro BNP(N-terminal pro-BNP) AHF – BNP >500 pg/m. L, or NT-pro. BNP >450/900/1800 Other causes if BNP<100 or NT-pro. BNP<450
BNP - Issues n n n Expense Intermediate values False Positives n n PE, Sepsis, renal failure, elderly, CHF False Negatives n Early in APO, Obesity, valvular or pericardial dis
Radiology n n Upper Lobe diversion Basilar and hilar infiltrates Kerley B Lines Loss of vascular delineation and widespread consolidation
Radiology n Kerley B Lines
Ultrasound
Ultrasound
Ultrasound
Ultrasound
Ultrasound
Management - General n n Remove from causative environment Maintain oxygenation Maintain cardiac output Treat underlying cause
Normotensive/Hypertensive Patient n Maximise oxygenation n n Preload and afterload reduction n n NIV Nitrates (ACEI), Frusemide Others Treat reversible causes
Nitrates n n n Relax smooth muscle Preload at low dose Afterload at higher dose Coronary effects Win n n limits Delivery- IV/SL/Top
Other drugs n n Other Vasodilators-SNP ACE Inhibitors n n n Afterload reduction improves CO Aspirin
Other drugs n Frusemide n n n Venodilator Diuretic Morphine n n Sympatholysis and anxiolysis ADHERE database - ^ ETT, ICU, mortality Not for routine use If required, use small doses!
Other drugs n Vasodilators n Nesiritide (BNP) n n Levosimendan n n Maybe Serelaxin n n No Nicorandil n n Arterial and venodilator but NOT recommended Maybe Endothelin receptor anatagonists- Tezosentan n No
Ventilatory support n n n High flow Oxygen to all ETT NIV- CPAP and Bi. PAP
NIV n n Oxygen delivery Pulmonary effects Cardiovascular effects Issues n n Tight mask PTX
NIV n Use in APO n CPAP Vs Bi. PAP
NIV Intubation
NIV Death
Hypotensive Patient n n Most severe RSI-ETT n n PEEP Invasive monitoring Inotropes - dobutamine Reperfusion therapy
Essentials High morbidity and mortality n Pathophysiological state n n n Maldistribution of fluid. Most patients are not fluid overloaded Maintain oxygenation and cardiac output. n Correct reversible causes. n In hypotensive patients. n In normotensive and hypertensive patients n n upright, oxygen, nitrates and CPAP. Nitrates reverse the cause n NIV is safe and effective n
Controversies n. Nitrate dosages n. Bi-PAP n. Frusemide, Morphine n. The role of new agents.
What do you get ready? n n n A Frusemide in big doses B Tezosentan- The Rep has just visited C Morphine. Everyone knows it’s great for APO D The Bi. PAP machine E The ETT F Your bag, as it’s almost home time
My suggestions n n n A No Frusemide B GTN C More GTN D The CPAP machine E Aspirin F Your bag as it’s almost home time