PILOT Background PILOT Pulmonary Fibrosis Identification Lessons for
")
PILOT: Background • PILOT (Pulmonary Fibrosis Identification: Lessons for Optimizing • • • Treatment) is a national education initiative driven by The France Foundation, an ACCME-accredited provider Education focuses on the early and accurate diagnosis of IPF, while also addressing critical issues related to optimizing disease intervention and management Led by experts in the IPF field, PILOT has attained a level of recognition and credibility across practitioner and patient communities that places it as one of the primary sources for timely and innovative education on IPF In the 10+ years since its launch, PILOT has had over 13 million hits to its educational Web site, www. PILOTfor. IPF. org.

PILOT: Steering Committee
 A Collaborator in this Regional Activity The PFF was founded")
Pulmonary Fibrosis Foundation (PFF) A Collaborator in this Regional Activity The PFF was founded in 2000 by brothers Albert Rose and Michael Rosenzweig, Ph. D after the brothers experienced firsthand the devastating effects of PF when their sister Claire passed away from the disease. Both brothers were also diagnosed with PF, and it was their vision and dedication that led to the creation of the Foundation. The mission of the PFF is to serve as the trusted resource for the pulmonary fibrosis community by raising awareness, providing disease education, and funding research.

Learning Objectives: Diagnosis • Recognize the importance of early diagnosis of IPF in collaboration with an • interdisciplinary team according to the 2011 ATS/ERS diagnostic criteria Explain key facets of the 2011 ATS/ERS criteria that support accurate, early, and definitive IPF diagnosis

Diagnosis David Lederer, MD, MS Columbia University Medical Center New York Presbyterian Hospital Amy L. Olson, MD, MSPH National Jewish Health
 IIPs Known cause, eg, drugs, collagen vascular disease IPF Granulomatous")
Interstitial Lung Disease (ILD) IIPs Known cause, eg, drugs, collagen vascular disease IPF Granulomatous eg, sarcoidosis Other forms (LAM, HX, etc) IIP other than IPF DIP RB-ILD AIP COP Idiopathic NSIP LIP Unclassifiable PPFE Rare Travis WD, et al, and the ATS/ERS Committee on IIPs. Am J Respir Crit Care Med. 2013; 188(6): 733 -748.

Where Does IPF Fit in the Context of the ILDs? • IPF is the most common of the Idiopathic Interstitial Pneumonias (IIPs) • Definition of IPF: – Specific form of chronic, progressive fibrosing interstitial pneumonia of unknown cause – Occurring primarily in older adults – Limited to the lungs ATS/ERS/JRS/ALAT consensus statement. Am J Respir Crit Care Med. 2011; 183: 788 -824.

Prevalence of IPF is Increasing Medicare Beneficiaries Age ≥ 65 Years • Prevalence was 0. 5% in 2011! • Median survival = 3. 8 years • Factors associated with lower survival – Age, index year, male sex Raghu G, et al. Lancet Respir Med. 2014; 2(7): 566 -572.
 Nathan SD, et al.")
IPF: Survival in the 2000 -2009 Era (Transplant Recipients Excluded) Nathan SD, et al. Chest. 2011; 140(1): 221 -229.

Case 1: Joanne History/Presentation • 62 -year-old woman with 7 years of gradually worsening exertional dyspnea and dry cough • Cannot climb more than 1 flight of stairs and is limited in her heavy ADLs • On supplemental O 2 • Joint pains of hands and some mild GERD, but no other symptoms of a CTD • Lifetime non-smoker • Joanne had a few birds in her home over the years, removed about 6 months ago

Physical Exam & Labs • BMI 31. 8 • Sp. O 2 95% on 4 L/min O 2 • Lungs: bilateral crackles and occasional inspiratory squeaks at the bases • Heart: S 1 normal, S 2 normal • Extremities: significant digital clubbing, +1 bilateral LE edema Labs: • HP panel: – + for pigeon serum – + for pigeon droppings • CTD panel performed – ANA + 1: 64 – All other serologies negative

Serological Evaluation • Should be performed before a biopsy • Minimum: ANA, RF, CCP antibody (ATS/ERS guidelines) • Based on history & physical exam, consider: – – – – Extractable nuclear antigen (ENA) autoantibody panel Anti-centromere antibody ESR & CRP MPO/PR 3 (ANCA) antibodies Anticardiolipin antibodies, lupus anticoagulant Creatine kinase, aldolase Hypersensitivity pneumonitis panel


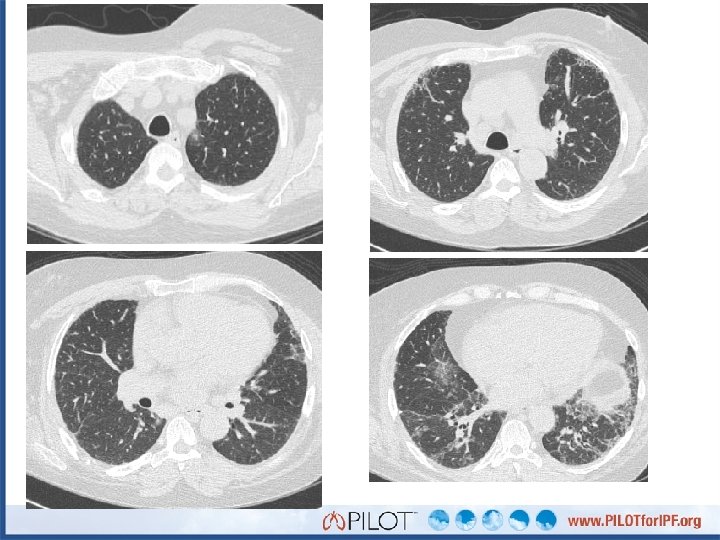
Point of Discussion: What is the most prominent feature of these images? A. B. C. D. E. Traction bronchiectasis Tumor nodules Peripheral honeycombing Air trapping Ground glass opacities

HRCT Criteria for UIP Pattern Possible UIP Pattern Subpleural, basal predominance + + Reticular abnormality + + + - + + Honeycombing (+/- traction bronchiectasis) Absence of “inconsistent” features Raghu G, et al, and the ATS/ERS/JRS/ALAT Committee on IPF. Am J Respir Crit Care Med. 2011; 183: 788 -824.

Point of Discussion: What is your diagnosis? A. B. C. D. E. F. Chronic hypersensitivity pneumonitis IPF NSIP Undifferentiated ILD CTD-ILD Rheumatoid lung

Point of Discussion: What is the next step for Joanne? A. B. C. D. E. Initiate steroids Initiate pirfenidone or nintedanib Refer for lung transplantation evaluation Obtain a surgical lung biopsy Refer for pulmonary rehab

Surgical Lung Biopsy Performed Fibrosis and honeycombing

Fibroblast Focus

Deeper Cuts Focus of OP Poorly formed granulomas

Now what is your diagnosis? A. B. C. D. E. F. Chronic hypersensitivity pneumonitis IPF NSIP Undifferentiated ILD CTD-ILD Rheumatoid lung

Now what is your diagnosis? A. B. C. D. E. F. Chronic hypersensitivity pneumonitis IPF NSIP Undifferentiated ILD CTD-ILD Rheumatoid lung

What are the Key Points in Joanne’s Case? • History and physical examination are critically important in developing a differential diagnosis • Serological evaluation is an important component of the ILD evaluation • Surgical lung biopsy should be considered if the diagnosis is not confirmed after history, physical examination, serological testing, and HRCT

Case 2: Marshal History/Presentation • Marshal is a 52 -year-old man – 18 months ago he developed exertional dyspnea with stairs • No cough, chest pain, or edema • Few years of bilateral hand, knee, and shoulder pain treated with NSAIDs • Never-smoker • No amiodarone, chemotherapy, radiation therapy, Raynaud’s, heartburn, or mold exposure • No family history of ILD, oxygen use, or CTD

Physical Exam • • • BMI 36. 4 Sp. O 2 89% on room air Lungs: bilateral crackles at the bases Heart: S 1 normal, S 2 normal Walks with a cane Extremities – Bilateral puffy proximal digits and MCP swelling – No wrist swelling – + Acrocyanosis

Point of Discussion: What is the next step for Marshal? A. B. C. D. E. Surgical lung biopsy Refer to a rheumatologist Empiric trial of prednisone Order autoimmune/CTD serologies Bronchoscopy

CTD Panel Results Test Marshal’s Result Normal Range ANA 1: 80 < 1: 40 CRP 70 < 10 mg/L ESR 64 0 -20 mm/hr RF 296 < 60 U/m. L CCP 101 < 20 EU/m. L

Point of Discussion: What is your diagnosis? A. B. C. D. E. F. Chronic hypersensitivity pneumonitis IPF NSIP Undifferentiated ILD CTD-ILD Rheumatoid lung

Point of Discussion: What is the next step for Marshal? A. B. C. D. E. Surgical lung biopsy Refer to a rheumatologist Empiric trial of prednisone Order autoimmune/CTD serologies Bronchoscopy

What are the key points in Marshal’s case? • History and physical examination are critical • A non-diagnostic HRCT should be followed by serological evaluation before a biopsy is performed

Case 3: Alex 71 -year-old Male with cough & dyspnea • Referred for evaluation of ILD • 6 months ago he developed productive cough, chills • Eventually hospitalized, treated with antibiotics and steroids • Prednisone tapered from 60 mg/day to 10 mg/day • Dyspnea with ADLs, working with physical therapy • Requires continuous oxygen therapy • Attests to frequent heartburn • Reports poor sleep, snoring, and daytime fatigue

Case 3: Alex 71 -year-old Male with cough & dyspnea Past Medical/Family/Social History • • + HTN, hyperlipidemia Family history of CAD Former 30 pack-year smoker Worked as a farmer Exam • • In wheelchair with supplemental oxygen 140/66, 86, 22, Sp. O 2 90% at rest on RA Bibasilar inspiratory crackles, no wheeze No edema or signs of CHF

71 -year-old Male with cough & dyspnea February 15 FEV 1 FVC FEV 1/FVC DLCO 2. 42 (84%) 2. 80 (64%) 0. 86 8. 75 (34%)

Point of Discussion: What is the most prominent HRCT feature? A. B. C. D. E. Traction bronchiectasis Tumor nodules Peripheral honeycombing Air trapping Ground glass opacities

Point of Discussion: What is your diagnosis? A. B. C. D. E. F. Chronic hypersensitivity pneumonitis IPF NSIP Undifferentiated ILD CTD-ILD Rheumatoid lung

Point of Discussion: The next step would be: A. Surgical lung biopsy B. Start the patient on N-acetylcysteine, azathioprine and prednisone C. Discuss risks and benefits of nintedanib and pirfenidone with Alex D. Recommend lung transplantation

Diagnostic Algorithm for IPF Suspected IPF Identifiable causes for ILD? No HRCT Possible UIP Inconsistent w/UIP Surgical Lung Biopsy UIP Probable UIP Non-classifiable fibrosis MDD IPF/Not IPF Raghu G, et al. Am J Respir Crit Care Med. 2011; 183: 788 -824. Not IPF

HRCT Criteria for UIP Pattern Possible UIP Pattern Subpleural, basal predominance + + Reticular abnormality + + + - + + Honeycombing (+/- traction bronchiectasis) Absence of “inconsistent” features Raghu G, et al. Am J Respir Crit Care Med. 2011; 183: 788 -824.

Point of Discussion: Would you get a VATS biopsy? A. B. C. D. E. Yes No No, a TBNA biopsy would be better Call a pulmonologist friend Ask the patient

Idiopathic Pulmonary Fibrosis Normal Lung Usual Interstitial Pneumonia

Idiopathic Pulmonary Fibrosis Normal Lung Fibroblastic Focus in Usual Interstitial Pneumonia

Interstitial Lung Disease Diagnostic Team Clinician Radiologist Pathologist Communication among multidisciplinary team is essential to an accurate diagnosis

Diagnosis Matters! IPF/UIP Confers a Poor Prognosis Cumulative Proportion Surviving Parameter IPF Dx Time (years) HR (95% CI) 28. 46 (5. 5, 147) Age 0. 99 (0. 95, 1. 03) Female sex 0. 31 (0. 13, 0. 72) Smoker 0. 30 (0. 13, 0. 72) Physio CRP 1. 06 (1. 01, 1. 11) Onset Sx (yrs) 1. 02 (0. 93, 1. 12) CT-fib score ≥ 2 0. 77 (0. 29, 2. 04) Correct diagnosis appropriate management Flaherty KR, et al. Eur Respir J. 2002; 19: 275 -283.

Delayed Care Associated with Higher Mortality P for trend = 0. 04 Lamas et al. Am J Respir Crit Care Med. 2011; 184: 842 -847.

What are the Key Points in Alex’s case? • The diagnosis of IPF can be made without a surgical lung biopsy in the right clinical setting • Empiric trials of prednisone should be discouraged

Key Messages: Presentation/Diagnosis • Differential diagnosis requires integration of clinical, serologic, history, and imaging data – A multidisciplinary approach should be taken for diagnosis of ILDs • Early and accurate diagnosis is critical

Conclusions: Diagnosing IPF • IPF is a fibrotic ILD • No identifiable cause for fibrosis – Exposure/CTD are absent • Either… – Characteristic HRCT pattern – UIP-pattern on surgical lung biopsy • Multidisciplinary approach enables an accurate diagnosis
- Slides: 49