PULMONARY TUBERCULOSIS Definition Chronic inflammatory response of prolonged

PULMONARY TUBERCULOSIS
 provoked by the persistence")
Definition Chronic inflammatory response of prolonged duration (weeks, months, years) provoked by the persistence of the causative organism Mycobacterium tuberculosis accompanied by tissue destruction and repair of lung tissue.
 is a")
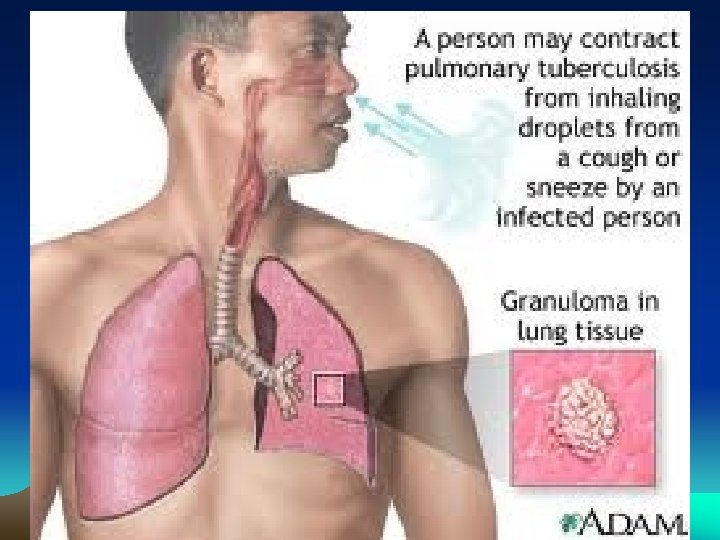
Pulmonary Tuberculosis • Tuberculosis (abbreviated as TB for tubercle bacillus or Tuberculosis) is a common and often deadly infectious disease caused by mycobacteria, mainly Mycobacterium tuberculosis. Tuberculosis usually attacks the lungs (as pulmonary TB).

TB Transmission What is TB? a. TB is a disease caused by infection with a bacteria called Mycobacterium tuberculosis.

Causative organism: Mycobacterium tuberculosis Morphology : • • • Slender Aerobic Weakly Gram + Rod Grows in straight or branching chains Unique waxy cell wall Acid Fast due to MYCOLIC ACID in the cell wall
 in sputum")
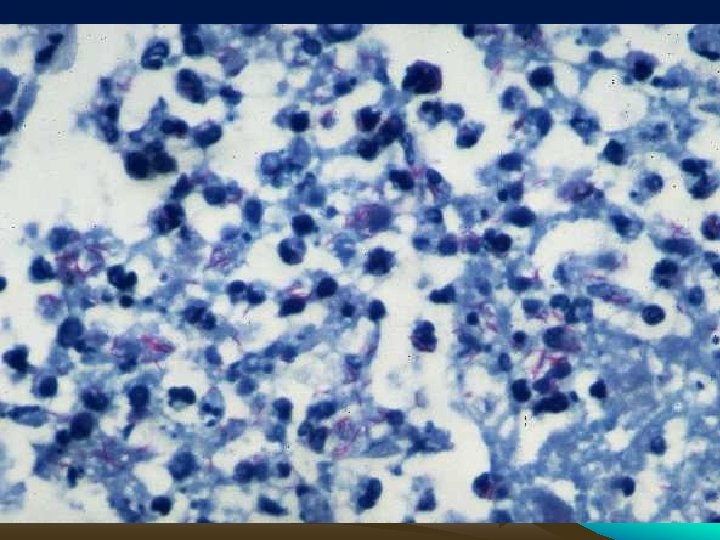
AFB smear Mycobacterium tuberculosis (stained red) in sputum

Pulmonary Tuberculosis • Scanning electron micrograph of Mycobacterium tuberculosis

Characteristics of Mycobacterial infection • Infiltration of mononuclear cells • Tissue destruction • Healing with scar formation and fibrosis

Other Characteristics: • Mode of transmission – Person to person by air born organisms • Reservoir – Humans with active disease of the lung • Primary infection – Usually asymptomatic • Secondary infection - Reactivation of primary focus • Tissue destruction by inflammatory cells • Attempts at repair with granuloma formation and fibrosis

TB Transmission How can you catch TB? a. TB is spread through tiny drops sprayed into the air when an infected person coughs, sneezes, or speaks, or another person breathes the air into their lungs containing the TB bacteria.

Epidemiology of Tuberculosis • • Affect 1. 7 billion people worldwide 8 -10 million new cases every year 1. 6 million deaths every year Over 10 million people infected with both HIV and M. tuberculosis • 14000 new cases in USA every year

Predisposing factors • Poverty • Overcrowding • Any chronic debilitating illness • Certain disease states: - Diabetes mellitus - Hodgkins lymphoma - Chronic lung disease (esp. silicosis) - Chronic renal failure

Other predisposing conditions: • Malnutrition • Alcoholism • Immunosupression

TB - Infection & Disease Categories of TB - Latent & Active a. TB disease varies with age and the ability of your body to fight off bacteria. a. HIV is the strongest risk factor for the progression of Latent TB to Active TB infection.

Immunology • Delayed hypersensitivity reaction • Mantoux Test : - Intradermal inj. of PPD - Visible/palpable induration >10 mm after 72 hrs - Signifies T-cell mediated immunity to mycobacterial antigen

Diagnostics • Inject intradermally 0. 1 ml of 5 TU PPD tuberculin • Produce wheal 6 mm to 10 mm in diameter • Represent DTH (delayed type hypersensitivity)

Reading of Mantoux test • Read reaction 48 -72 hours after injection • Measure only induration • Record reaction in mm

Even if a Skin Test is Negative…. . Coughing up Blood Chills Chiclls Fatigue Difficulty in Breathing THINK TB! FFever Anorexia Loss of Appetite Night sweats

• False negative; certain viral inf. , sarcoidosis, malnutrition, hodgkins lymphoma, immunosupression, miliary tuberculosis. • False positive; atypical mycobacterial inf. , BCG vaccination
 • Macrophages – Scattered all over (microglia,")
Pathogenesis : The Players (mononuclear phagocyte system) • Macrophages – Scattered all over (microglia, Kupffer cells, sinus histiocytes, alveolar macrophages, etc. ) – Circulate as monocytes and reach site of injury within 24 – 48 hrs and transform – Become activated by T cell-derived cytokines, endotoxins, and other products of inflammation

Macrophages serve to eliminate injurious agents and initiate repairhowever, they are as well responsible for much of the tissue injury that occurs Tissue macrophage Activated T cell or NK cell Non Immune activation: Endotoxins, fibronectin, chemical mediators IFN-g Activated macrophage Fibrosis (Scaring) Tissue injury Toxic oxygen metabolites Metallo-proteases Coagulation factors AA metabolites and NO Growth factors involved in fibroblast proliferation (PDGF, TGFb, FGF) Angiogenesis factors (FGF, VEGF) Collagen deposition (IL-13 and TGFb)
")
The Players…. • T and B lymphocytes – Antigen-activated (via macrophages and dendritic cells) – Release macrophage-activating cytokines (in turn, macrophages release lymphocyteactivating cytokines until inflammatory stimulus is removed) • Plasma cells – Terminally differentiated B cells – Produce antibodies

The dominant cellular player in pulmonary tuberculosis is the tissue macrophage Blood monocyte Tissue macrophage (RES) migrate into tissue Kupffer cell within 48 hours (liver) after injury Microglia (CNS) Histiocytes (spleen) and differentiate It is joined by lymphocytes and plasma cells, Alveolar macs (lung) however mast cells and eosinophils are as well involved in chronic allergic diseases Lymphocyte Plasma cell

Pathogenesis
: inhalation of Mycobacteria---enter alveolar macrophages---replication in")
Pathogenesis • A-Primary Pulmonary Tuberculosis (0 -3 weeks): inhalation of Mycobacteria---enter alveolar macrophages---replication in phagosome--bacteremia---seeding of multiple sites
: Alveolar macrophages---IL-2 ---T Cells--- Thelper cells---Activated")
Pathogenesis • B -Primary pulmonary tuberculosis (>3 weeks): Alveolar macrophages---IL-2 ---T Cells--- Thelper cells---Activated macrophages (i)--- TNF, Chemokines—Hypersensitivity (epith. granulomas) and (ii)---Nitric oxide, reactive O 2 sp. ---Immunity (bactericidal activity)
 asymptomatic; Infection contained •")
Primary Tuberculosis • Develops in unexposed, unsensitized persons • Mostly(95%) asymptomatic; Infection contained • In 5 % symptomatic; Primary progressive tuberculosis • Source of organism; Exogenous • Difficult to diagnose

Primary Tuberculosis Presentation : • Lung consolidation; Lower and middle lobes • Hilar lymphadenopathy • Pleural effusion • In majority organism remain dormant • In severe immunosupression - TB Meningitis - Miliary Tuberculosis

Secondary Tuberculosis • Arises in previously sensitized host • Many years after primary infection • Reactivation of latent infection or overwhelming exogenous infection • Involves apex of upper lobes • Cavitation more prominant

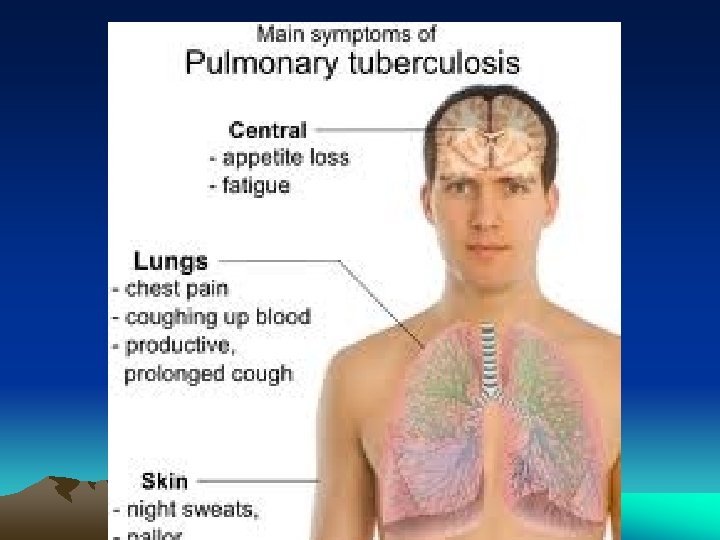
Secondary Tuberculosis • In majority symptomatic; insidious onset of malaise, anorexia, weightloss, fever, productive cough (mucoid, purulent, hemoptysis) , pleuritic pain. • Extrapulmonary manifestations • May be asymptomatic when localised

TB Infection & Disease There are 2 Categories of TB: Latent & Active a. TB infection of the lungs can fall into 2 categories of disease: Latent TB or Active TB. a. Latent TB means a person is infected by TB bacteria, but cannot infect others, and is not coughing or appearing sick. a. Latent TB means the body’s immune system has contained the infection.

TB - Infection & Disease Categories of TB - Latent a. Persons with latent TB are identified by a positive skin test (PPD). a. Persons who are not infected with Mycobacterium tuberculosis have a negative skin test (PPD).

In Pulmonary Tuberculosis macrophage accumulation persists by different mechanisms: • Continued recruitment of monocytes from the circulation • Local proliferation • Prolonged survival and immobilization

Outcome of Tuberculous infection • Ulcers • Fistulas • Granulomatous diseases • Fibrotic diseases • and combinations of the above



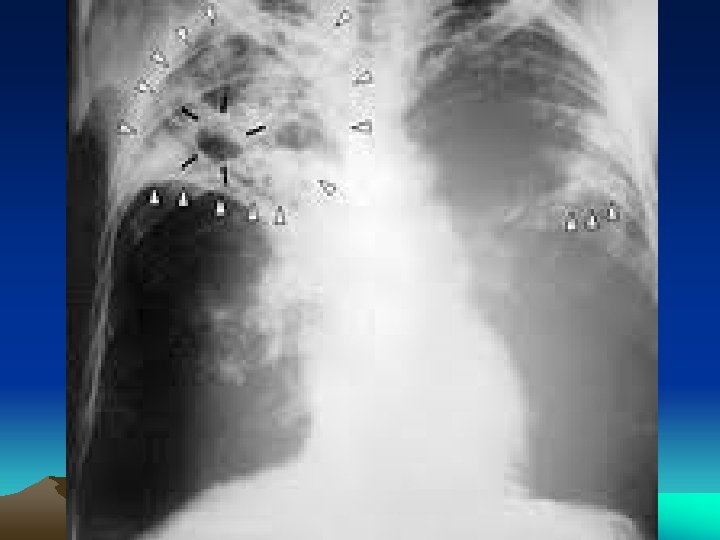
Diagnosis • History • Physical examination • X-Rays ; Consolidation/ cavitation in lung apices • Sputum for AFB : - Z. N Stain - > 10000 organisms in clinical specimen

Diagnosis • Sputum Culture : - conventional ---upto 10 weeks - liquid --- within 2 weeks • P. C. R : - 10 org. in clinical specimen

Chest radiography • No chest X-ray pattern is absolutely typical of TB • 10 -15% of culture-positive TB patients not diagnosed by X-ray • 40% of patients diagnosed as having TB on the basis of x-ray alone do not have active TB

Number of sputum samples required • overall diagnostic yield for sputum examination related to – the quantity of sputum (at least 5 m. L) – the quality of sputum – multiple samples obtained at different times to the laboratory for processing • 3 samples obtained at least eight hours apart with at least one sample obtained in the early morning

Cultures

Morphology A-Primary Tuberculosis : • Ghon complex - subpleural parenchymal lesion (lower part of upper lobe) - hilar lymphadenopathy • Progressive fibrosis • Calcification



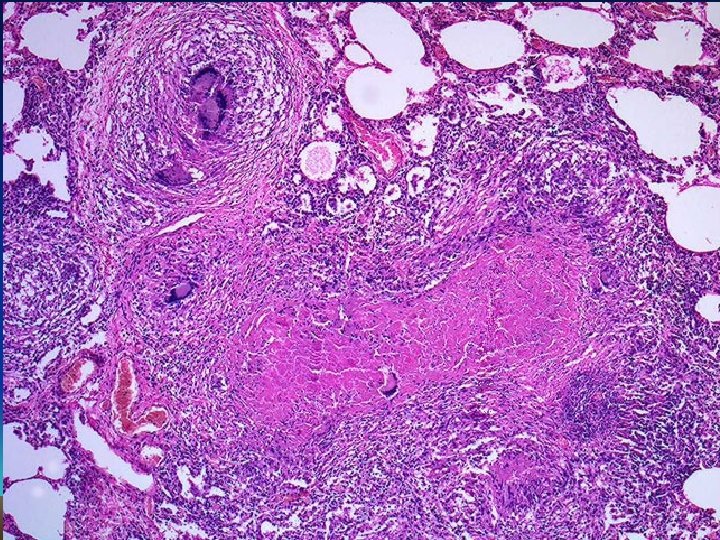
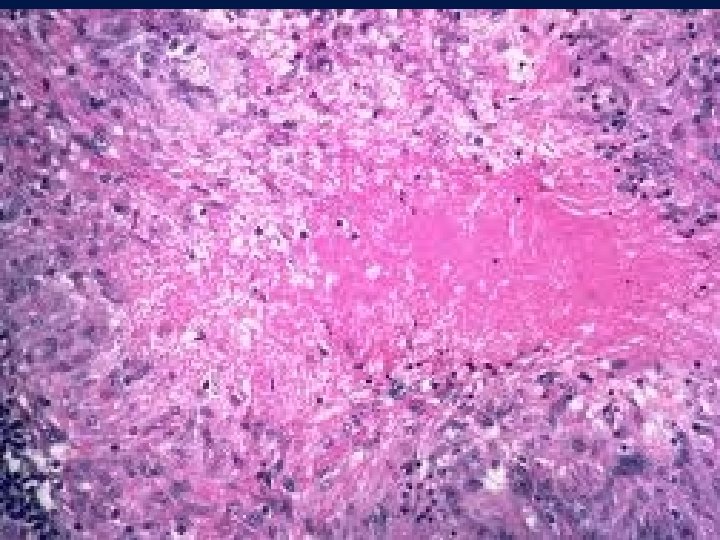
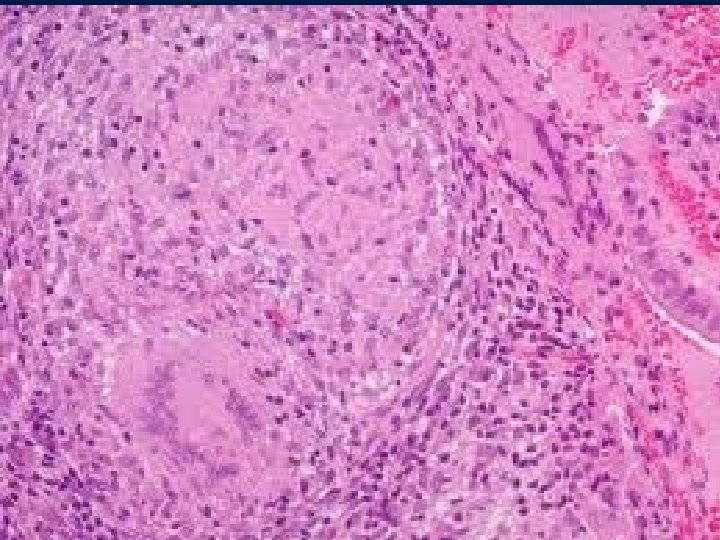
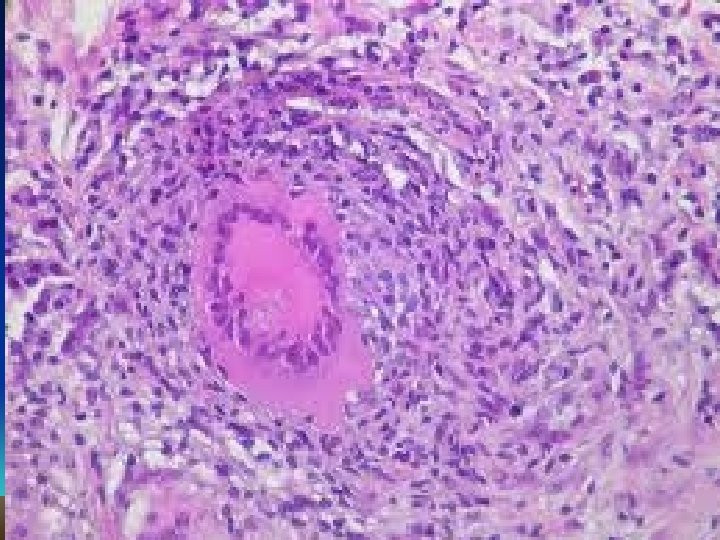
Histology : Epithelioid cell granulomas • epithelioid cells • lymphocytes • plasma cells • multinucleated langhan’s type giant cells • with or without central caseation
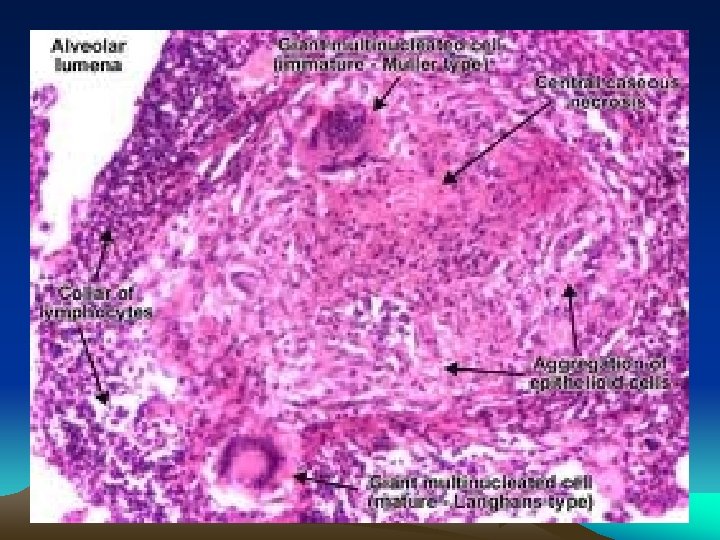

Granulomatous Inflammation • Clusters of T cell-activated macrophages, which engulf and surround indigestible foreign bodies (mycobacteria, H. capsulatum, silica, suture material) • Resemble squamous cells, therefore called “epithelioid” granulomas

Morphology B – Secondary Tuberculosis : • Focus of consolidation, < 2 cm • Within 1 -2 cm of apical pleura • Histology : Caseating granulomas

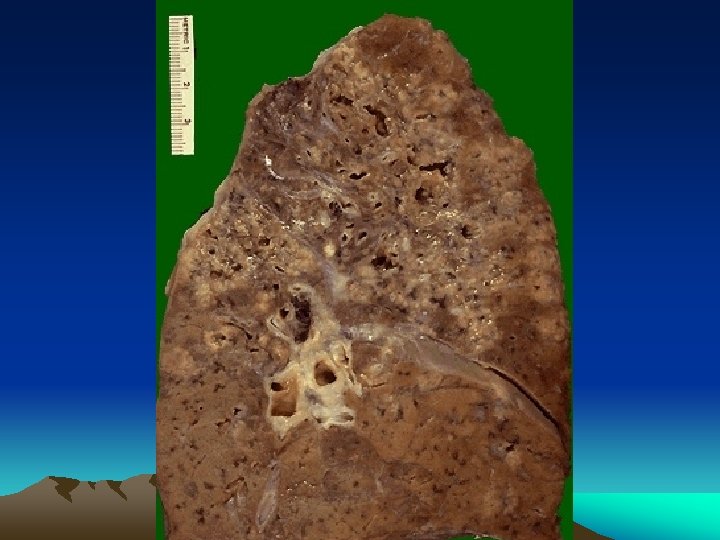
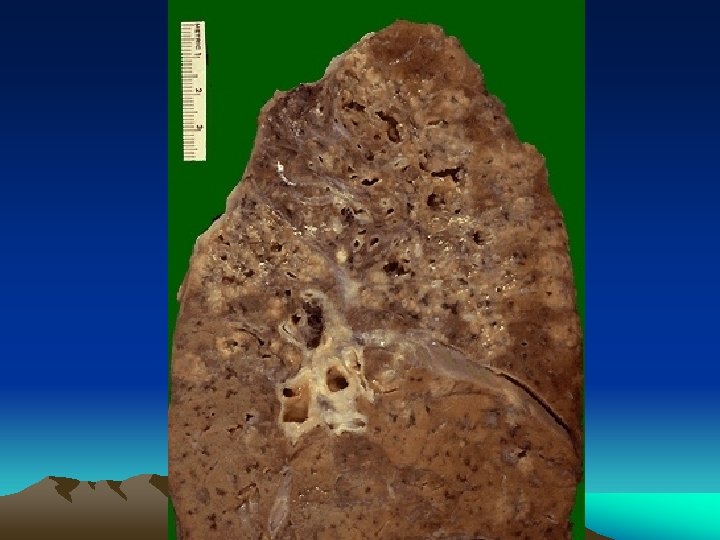
Morphology C – Progressive Pulmonary Tuberculosis: • Elderly/ immunosupressed • Apical lesion---Spreads to adjacent lung tissue--Involves : a) Bronchi b) Blood vessels • Irregular cavity , poorly walled off by fibrosis

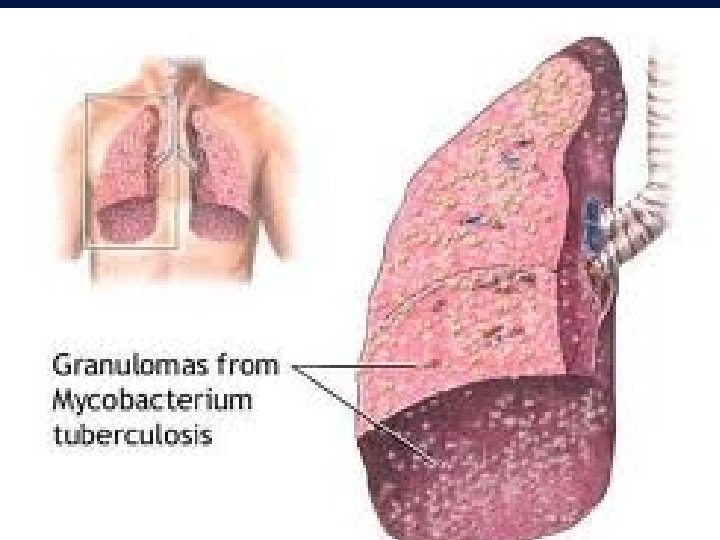
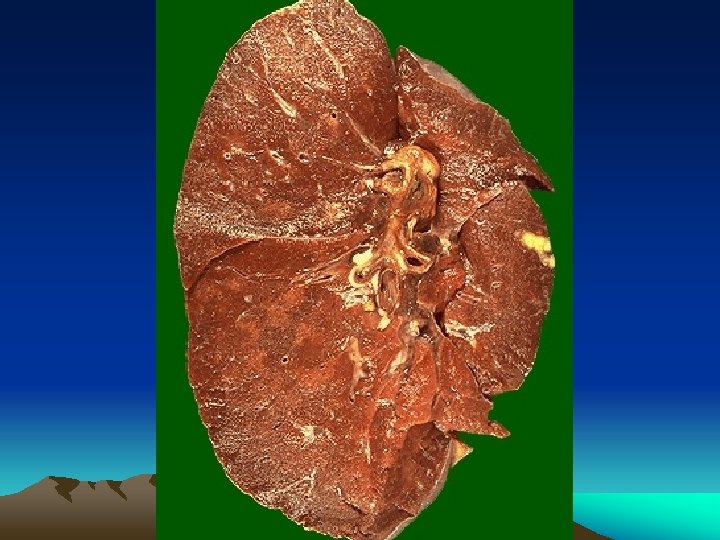
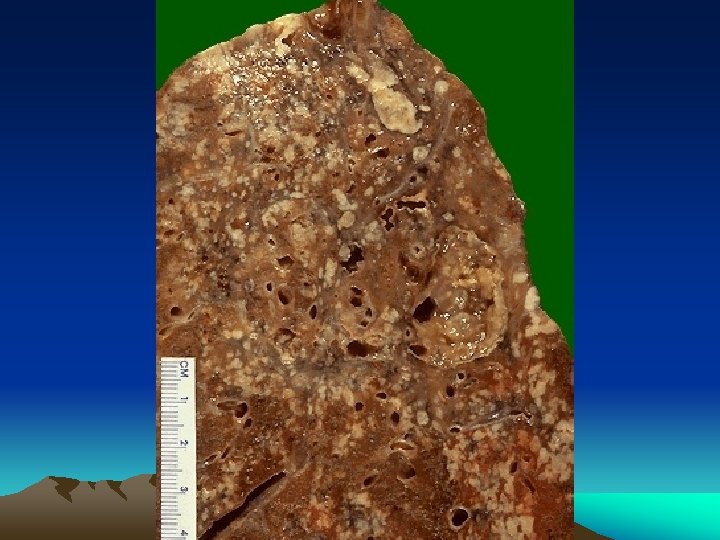
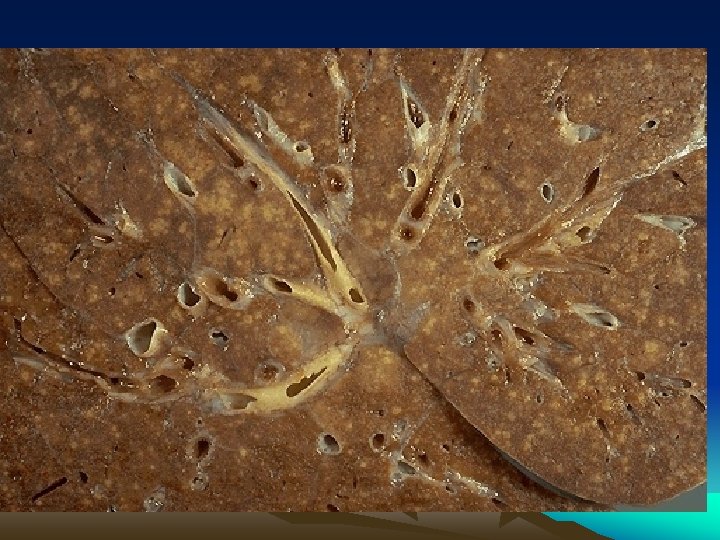
Morphology D – Miliary Pulmonary Tuberculosis : • Organisms draining through lymphatics enter venous blood and circulate back into the lung and involving most of the parenchymal tissue. • Microscopic or small visible yellowish white foci resembling “millet” seeds • Coalesce to form larger cavity



Pleural cavity : Involvement of Pleural cavity in Progressive pulmonary tuberculosis; • Serous pleural effusion • Tuberculous empyema • Obliterative fibrous pleuritis

E – Endobroncheal, Endotracheal or Laryngeal Tuberculosis : • Spread via lymphatics or • Expectoration of infected material • Histology : - Mucosal lining studded with tiny granulomas

TB Infection and Disease a. The lungs are the most common place for TB. This is known as pulmonary TB. a. TB of the voice box is the second most common and is usually called laryngeal TB.

F – Systemic Miliary Tuberculosis : • Bacteremia--- Involvement of Systemic Arterial System--- Any organ : - Liver - Bone marrow - Spleen - Adrenals - Meninges - Kidneys - Fallopian tubes - Epididymus
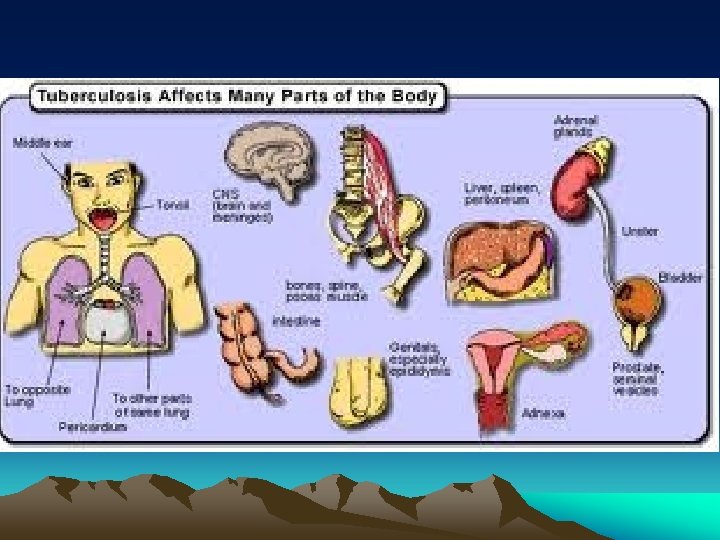

• G – Isolated Tuberculosis : • Any organ or tissue can be involved in isolation ; hematogenous spread ; - Meninges - Kidneys - Adrenals (Addison’s Disease) - Bone - Fallopian tubes - Vertebra (Pott’s Disease) . Paraspinal Cold Abscess track along tissue planes ( Abdominal or pelvic mass)



H – Intestinal Tuberculosis : • Drinking contaminated unpasteurised milk or • Swallowing of coughed - up infected material in patients with advanced pulmonary tuberculosis • Organism invade lymphoid aggregates-- Granulomatous inflammation--- Mucosal ulceration (usually illeum)

I- Lymphadenopathy : • Most common presentation of Extrapulmonary Tuberculosis • Usually in Cervical region (“Scrofula”) • Unifocal or localised • Multifocal in HIV patients


Lymph Nodes and Lymphatics • Lymphatics drain tissues – Flow increased in inflammation – Antigen to the lymph node – Toxins, infectious agents also to the node • Lymphadenitis, lymphangitis • Usually contained there, otherwise bacteremia ensues • Tissue-resident macrophages must then prevent overwhelming infection

Systemic effects • Fever – One of the easily recognized cytokinemediated (esp. IL-1, IL-6, TNF) acute-phase reactions including • Anorexia • Skeletal muscle protein degradation • Hypotension • Leukocytosis – Elevated white blood cell count
 – Bacterial infection (neutrophilia) – Parasitic infection (eosinophilia) – Viral infection")
Systemic effects (cont’d) – Bacterial infection (neutrophilia) – Parasitic infection (eosinophilia) – Viral infection (lymphocytosis)

Granulomatous inflammation Granulomas are millimeter size nodules of chronic inflammatory cells that can be isolated or confluent. Granuloma formation is the result of dealing with indigestible substances or pathogens and walls them off The essential component are modified macrophages named epithelioid cell (because of shape). Epithelioid cells can form multinucleated giant cells. Epithelioid cells are surrounded by a collar of lymphocytes and occasionally plasma cells. Fibrous connective tissue often surrounds granulomas (remodeling of tissue) Areas within the granuloma can undergo necrosis (prototype: caseous necrosis in tuberculosis). Necrosis can lead to calcification or liquefaction and formation of a cavern if drained.

Microscopic and macroscopic appearance of tuberculosis Characteristic tubercle with caseating necrosis in center Cavity formation due to liquefaction and drainage of TBC lesion Macroscopic lesion in TBC

Differential Diagnosis : • LEPROSY -Mycobacterium Leprae Tuberculoid Form: Granulomas with acid fast bacilli in macrophages and epitheloid cells.

• CAT SCRATCH DISEASE -Gram positive bacilli Rounded or stellate granulomas containing central granular debris with neutrophils.

• SCHISTOSOMIASIS -S. Mansoni, S hematobium, S. japonicum Granulomas around eggs with numerous eosinophils.

• FUNGAL Cryptococcus neoformans Organism yeast like, budding, 5 -10 mm clear capsule. Coccidioides immitis Organism appears as 30 – 80 mm cyst containing spores of 3 – 5 mm each.

• IN ORGANIC METALS , DUSTS Silicosis : Beryliosis : Involvement of lungs , fibrosis.

• SARCOIDOSIS Unknown Etiology : Noncaseating granulomas , langhan and foreign body type giant cells.

Treatment

Treatment for Active TB a. The CDC recommends that infections due to Mycobacterium tuberculosis be treated with several drugs in addition to INH: Rifampin, Ethambutol, Streptomycin, and Pyrazinamide.
, is isoniazid, rifampicin,")
Tuberculosis treatment • The standard "short" course treatment for tuberculosis (TB), is isoniazid, rifampicin, pyrazinamide, and ethambutol for two months, then isoniazid and rifampicin alone for a further four months. The patient is considered cured at six months (although there is still a relapse rate of 2 to 3%). For latent tuberculosis, the standard treatment is six to nine months of isoniazid alone. • If the organism is known to be fully sensitive, then treatment is with isoniazid, rifampicin, and pyrazinamide for two months, followed by isoniazid and rifampicin for four months. Ethambutol need not be used.

Drugs • 1. 2. 3. 4. 5. All first-line anti-tuberculous drug names have a standard three-letter and a single-letter abbreviation: ethambutol is EMB or E, isoniazid is INH or H, pyrazinamide is PZA or Z, rifampicin is RMP or R, Streptomycin is STM or S.
 used for the treatment")
Drugs • There are six classes of second-line drugs (SLDs) used for the treatment of TB. A drug may be classed as second-line instead of first-line : it may be less effective than the first-line drugs. 1. aminoglycosides: e. g. , amikacin (AMK), kanamycin (KM); 2. polypeptides: e. g. , capreomycin, viomycin, enviomycin; 3. fluoroquinolones: e. g. , ciprofloxacin (CIP), levofloxacin, moxifloxacin (MXF); 4. thioamides: e. g. ethionamide, prothionamide 5. cycloserine (the only antibiotic in its class); 6. p-aminosalicylic acid (PAS or P).

Drugs “Third-line • • 1. 2. 3. 4. 5. 6. 7. 8. drugs" Not very effective or because their efficacy has not been proven. Rifabutin is effective, but is not included on the WHO list because for most developing countries, it is impractically expensive. rifabutin macrolides: e. g. , clarithromycin (CLR); linezolid (LZD); thioacetazone (T); thioridazinea; arginine; vitamin D; R 207910.
 is defined as resistance to the two most")
Drugs • Multi-drug resistant TB (MDR-TB) is defined as resistance to the two most effective first-line TB drugs: rifampicin and isoniazid. • Extensively drug-resistant TB (XDR-TB) is also resistant to three or more of the six classes of second-line drugs.
 a. Multidrug-resistant TB is on the rise.")
Treatment for Active TB Multidrug-resistant TB (MDR) a. Multidrug-resistant TB is on the rise. MDR TB means that some TB bacteria have developed resistance, so that traditional antibiotics, like INH, no longer kill the bacteria. “This is due to people not taking their medication properly; new strains of the bacteria evolve. ”

Monitoring and DOTS • DOTS stands for "Directly Observed Therapy, Short-course" and is a major plan in the WHO global TB eradication programme. • The DOTS strategy focuses on five main points of action. 1. These include government commitment to control TB, 2. diagnosis based on sputum-smear microscopy tests done on patients who actively report TB symptoms, 3. direct observation short-course chemotherapy treatments, 4. a definite supply of drugs, and 5. standardized reporting and recording of cases and treatment outcomes.

Treatment for Active TB…. a. TB is curable, IF it is diagnosed early and appropriate treatment is started promptly. a. Active TB can be spread to other people if the person is not taking medication to kill the bacteria!

Treatment for Active TB a. When a person with active TB is diagnosed, they should be isolated from other people until the medication begins to kill the bacteria-usually 2 weeks, but sometimes longer.

Prevention • TB prevention and control takes two parallel approaches : • In the first, people with TB and their contacts are identified and then treated. • Identification of infections often involves testing high-risk groups for TB. • In the second approach, children are vaccinated to protect them from TB.

Current Surgical Intervention • Patients with hemoptysis first received Bronchial Artery Embolization because of the recurrent hemoptysis. • Current indication of Lung Resection for pulmonary tuberculosis includes MDR-TB with a poor response to medical therapy, hemoptysis due to bronchiectasis or Aspergillus superinfection, and destroyed lung as previously reported, which are consistent with our indications. • Surgery remains a crucial adjunct to medical therapy for the treatment of MDR-TB and medical failure lesions.

Fundamentals of TB Infection Control Practices a. Identify persons with active TB early. a. Initiate effective and appropriate isolation of known or suspected TB cases. a. Initiate effective anti-TB treatment promptly. . .

As a healthcare worker, how can I protect myself from being exposed? a. Instruct your patients to cover their mouth when coughing and do not transport patients with TB throughout the hospital unless they are wearing a mask.

- Slides: 106