The Open Dialogue Method A radically different approach






















 there is nothing more terrible")
























- Slides: 48
The Open Dialogue Method A radically different approach for “psychosis” A Presentation By Ron Unger LCSW 4 ronunger@gmail. com 541 -513 -1811
What is the problem? n Is it that “bad” voices are speaking n And we need to shut them up? n n With drugs, if necessary? Or is the problem that not all voices are being heard n And so we need better ways of listening and of having dialogue?
Origins of open dialogue n n n Initiated in Finnish Western Lapland since early 1980’s Need-Adapted approach – Yrjö Alanen Integrating systemic family therapy and psychodynamic psychotherapy Treatment meeting 1984 Systematic analysis of the approach since 1988 –”social action research” Systematic family therapy training for the entire staff – since 1989 Slide by Jaakko Seikkula
COMPARISON OF 5 -YEARS FOLLOW-UPS IN WESTERN LAPLAND STOCKHOLM ODAP Western Lapland 1992 -1997 N = 72 Diagnosis: Schizophrenia Other non-affective psychosis Mean age years female Hospitalization days/mean Neuroleptic used - ongoing GAF at f-u Disability allowance or sick leave n Stockholm* 1991 -1992 N=71 59 % 54 % 41 % 46 % 26. 5 27. 5 30 29 31 33 % 17 % 66 19 % 110 93 % 75 % 55 62 % *Svedberg, B. , Mesterton, A. & Cullberg, J. (2001). First-episode non-affective psychosis in a total urban population: a 5 -year follow-up. Social Psychiatry, 36: 332 -337. Slide by Jaakko Seikkula
Three hypothesis n n n ”Psychosis” does not exist Psychotic symptoms are not symptoms of an illness strategy for our embodied mind to survive strange experiences Longstanding psychotic behaviour is perhaps more an outcome of poor treatment in two respect - treatment starts all too late - non adequate understanding of the problem leads to wrong response by the treatment Slide by Jaakko Seikkula
Problems with mainstream treatment models: n n Clients become not heard- neither the patient nor the family members Over-emphasize on inpatient treatment – patients disposed to others’ psychotic behavior (J. Cullberg) Over-emphasize in medication – increases the risk for untimely deaths & other problems Over-emphasize in pathologising the problems – resources are not seen Slide by Jaakko Seikkula
MAIN PRINCIPLES FOR ORGANIZING OPEN DIALOGUES IN SOCIAL NETWORKS n n n n IMMEDIATE HELP SOCIAL NETWORK PERSPECTIVE FLEXIBILITY AND MOBILITY RESPONSIBILITY PSYCHOLOGICAL CONTINUITY TOLERANCE OF UNCERTAINTY DIALOGISM Slide by Jaakko Seikkula
IMMEDIATE HELP n n n First meeting in 24 hours Crisis service for 24 hours All participate from the outset Psychotic stories are discussed in open dialogue with everyone present The patient reaches something of the ”not-yet-said” Slide by Jaakko Seikkula
SOCIAL NETWORK PERSPECTIVE n n n Those who define the problem should be included into the treatment process A joint discussion and decision on who knows about the problem, who could help and who should be invited into the treatment meeting Family, relatives, friends, fellow workers and other authorities Slide by Jaakko Seikkula
FLEXIBILITY AND MOBILITY n n n The response is need-adapted to fit the special and changing needs of every patient and their social network The place for the meeting is jointly decided From institutions to homes, to working places, to schools, to polyclinics etc. Slide by Jaakko Seikkula
RESPONSIBILITY n n n The one who is first contacted is responsible for arranging the first meeting The team takes charge of the whole process regardless of the place of the treatment All issues are openly discussed between the doctor in charge and the team Slide by Jaakko Seikkula
PSYCHOLOGICAL CONTINUITY n n n An integrated team, including both outpatient and inpatient staff, is formed The meetings as often as needed The meetings for as long period as needed The same team both in the hospital and in the outpatient setting In the next crisis the core of the same team Not to refer to another place Slide by Jaakko Seikkula
TOLERANCE OF UNCERTAINTY n n To build up a scene for a safe enough process To promote the psychological resources of the patient and those nearest him/her To avoid premature decisions and treatment plans To define open Slide by Jaakko Seikkula
Tolerance of Uncertainty n Be present without a preconceived definition of the problem n Speak as a listener n “Live your way into the answer”-- Rilke Mary E. Olson, Ph. D. 2010
DIALOGISM n n n The emphasize in generating dialogue not primarily in promoting change in the patient or in the family New words and joint language for the experiences, which do not yet have words or language Listen to what the people say not to what they mean Slide by Jaakko Seikkula
SIMPLE GUIDES FOR THE DIALOGUE IN PRESENT MOMENT n n n n Prefer themes of the actual conversation instead of narratives of past, but be realistic Follow clients stories and be careful with your own openings Guarantee response to spoken utterances. Responses are embodied, comprehensive Note different voices, both inner and horizontal Listen to your own embodied responses Take time for reflective talks with your collegians Dialogical utterances, speak in I form Proceed peaceful, silences are good for dialogue Slide by Jaakko Seikkula
1: GUARANTEEING JOINT HISTORY n n n Everyone participates from the outset in the meeting All things associated with analyzing the problems, planning the treatment and decision making are discussed openly and decided while everyone present Neither themes nor form of dialogue are planned in advance Slide by Jaakko Seikkula
2: GENERATING NEW WORDS AND LANGUAGE n n The primary aim in the meetings is not an intervention changing the family or the patient The aim is to build up a new joint language for those experiences, which do not yet have words Slide by Jaakko Seikkula
3: STRUCTURE BY THE CONTEXT n n Meeting can be conducted by one therapist or the entire team can participate in interviewing Task for the facilitator(s) is to n n (1) open the meeting with open ended questions; (2) to guarantee voices becoming heard; (3) to build up a place for reflective comments among the professionals; (4) to conclude the meeting with definition of what have we done. Slide by Jaakko Seikkula
4: BECOMING TRANSPARENT n n n n Professionals discuss openly of their own observations while the network is present There is no specific reflective team, but the reflective conversation is taking place by changing positions from interviewing to having a dialogue - look at your collegian – not at clients - positive, resource orientated comments - in form of a questions – “I wonder if …” - in the end ask clients comments Reflections are for me to understand more – not a therapeutic intervention Slide by Jaakko Seikkula
5: FOLLOWING WORDS – NOT MEANINGS n In the conversation the team tries to follow the words and language used by the network members instead of finding explanations behind the obvious behavior Slide by Jaakko Seikkula
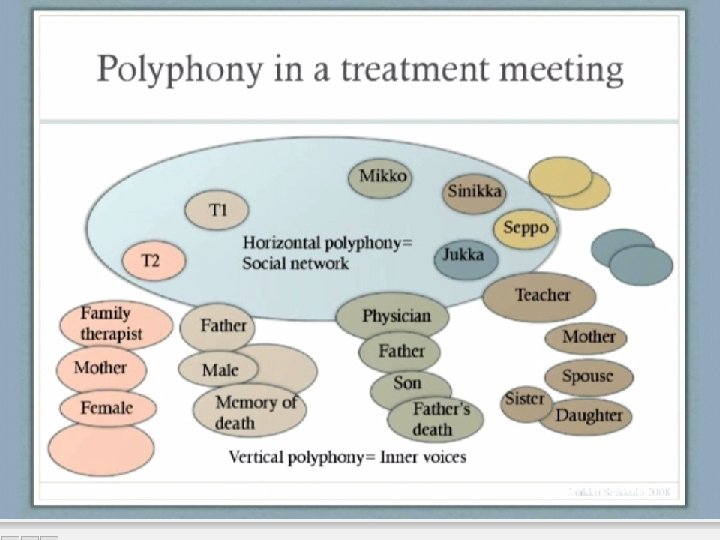
Basic assumptions of relational life n n We born into relations – relations become our emodied being We are intersubjective – not one entity We are living in the polyphony of voices Dialogue between voices is the basic human experience Slide by Jaakko Seikkula
“For the word (and, consequently, for a human being) there is nothing more terrible than a lack of response” “Being heard as such is already a dialogic relation” (Bakhtin, 1975) Slide by Jaakko Seikkula
A Dangerous Myth n In modern psychiatric systems, people are commonly taught that responding to psychotic sorts of expressions make the psychosis worse n n The failure to respond increases isolation And isolation is a known contributor to psychosis
How to respond: n “Answering does not mean giving an explanation or interpretation, but rather, demonstrating in one’s response that one has noticed what has been said, and when possible, opening a new point of view on what has been said. ”
“Love is the life force, the soul, the idea. There is no dialogical relation without love, just as there is no love in isolation. Love is dialogic. ” (Patterson, D. 1988) Literature and spirit: Essay on Bakhtin and his contemporaries, 142) Slide by Jaakko Seikkula
Moments of Change n “Feelings of love, manifesting powerful mutual emotional attunement in the conversation, signal moments of therapeutic change” n From the article, “Making sense of multiactor dialogs”
Love is a Dialogic Relation The feelings of love that emerge in us during a network meeting are neither romantic nor erotic. They are our own embodied responses to participation in a shared world of meaning co-created with people who trust each other and ourselves to be transparent, comprehensive beings with each other. --Jaakko Seikkula (2005) Copyright © 2014
The role of heavy, difficult emotions n The usual pattern: n n The heavier the emotions lived through in the meeting, the more favorable the outcome The key is not to treat painful emotions as dangerous, but to let them flow
Slide by Jaakko Seikkula
Wisdom emerges out of a process where all the voices are heard n DBT therapists emphasize that “wise mind” is where emotional mind and rational mind overlap n That’s just one example of how to be healthy, we need to draw from a variety of sources at the same time n Rather than attempting to suppress divergent views
Two simultaneous histories 1. Embodied living in the present moment - shared experience - implicit knowing - comments about the present experience 2. Narratives that we tell of the past incidents, experiences and things - meanings constructed Slide by Jaakko Seikkula
Emphasis on how the story is being told in the present moment n “Those who do not have power over the story that dominates their lives, the power to retell it, rethink it, deconstruct it, joke about it, and change it as times change, truly are powerless. ” — Salman Rushdie
Andersen’s Reflecting Process • Comments are formed as a logical connotation as opposed to blaming or pejorative statements • Ideas are presented tentatively • Comments attend to verbal and non-verbal communication • Reflections attempt to address different sides of the dilemma • Emphasis is on presenting a “smorgasbord of ideas” • Speculations are restricted to the conversation • Comments may be raised regarding what was not said or asked by the interviewer • Comments may be presented as stories, metaphors, and with images Mary E. Olson, Ph. D. 2010
Reflecting Process in OD n n Professionals and family sit in a circle The interviewer can participate in reflecting process More spontaneous and unstructured Geared toward emotional reassurance and giving language to the psychotic experience Mary E. Olson, Ph. D. 2010
Michael White’s Algorithm For the Reflecting Process n n Expression: What caught your attention? Image: What images came to you as you listened? Resonance: What feelings and memories were evoked from your own experience? Transport: How were you moved? (Moved can be in terms of understanding, new ideas, or emotions. ) Mary E. Olson, Ph. D. 2010
Open Dialogue and Voice Dialogue n When dialogue is facilitated in the social network n n Then it is also more likely to happen within a person An Open Dialogue facilitator is interested in hearing all the voices n n All the voices within a person And the voices of all those in the social network
Crisis & the move toward Monologue n In a simple crisis, we attempt to find resolution by deciding on the “right” thing to think or do n This leads to attempts to shut other points of view that seem wrong n n In some cases, this sets off prolonged conflict In a complex crisis, there is no one “right” thing to do or way to think n In a complex crisis, we do better to seek out dialogue, with multiple points of view
What we each can do on our own n n It takes a well trained team with lots of institutional support to practice the Open Dialogue method But any one of us (or two or three) can use some of the principles to make our interactions more “dialogical” n And that can start to make a difference
A few dialogical principles for everyday mental health treatment n Humility by professionals n n n Seek to respond to all attempts at communication n n Admit uncertainty Keep multiple views “on the table” Rather than define some messages as “too psychotic” to respond to Involve the person & social network in decisions wherever possible
Another dialogical principle for everyday mental health treatment n Seek to have all voices be heard, both inner voices & voices of family etc. n n Rather than elimination of “bad” voices Avoid letting destructive voices dominate n n But also be curious about what they may have to offer Look for health to emerge out of dialogue, not imposition of “sanity”
12 Key Elements of Dialogic Practice Two or more therapists 2. Participation of family and/or network members 3. Use of initial open-ended inquiry questions 4. Responding to client utterances 5. Emphasis on the present moment 6. Integration or exchange of multiple viewpoints 1. Inner and outer polyphony 7. Responding problematic discourse or behavior as meaningful 8. Use of relational focus, e. g. circular questions 9. Emphasis on current stories, not symptoms 10. Reflecting conversation among professionals 11. Principle of transparency 12. Tolerance of Uncertainty 1. Copyright © 2014 by Mary Olson
Exercise n Volunteers Needed: n 3 Community Members n n with concerns they would like to discuss in a meeting in front of all of us 2 “team members” n n Will assist in interviewing the community members Will take part in the reflecting exercise
Problem in current system: n n Shift in Language. Loss of Language of Living World—History, Stories, Metaphor, Narrative, Dialogue, etc. Instead the Assumption that Things Can Be Comprehensively Understood in Nonliving Terms: “Chemical Imbalances. ”
S M S
S M S
S M S