Sock Removal Shock Lower Extremity Wounds in Dialysis





















 DUE TO WORSENING WOUNDS WITH TENDON EXPOSURE ON THE DORSAL RIGHT")
 ON 2/28/17 REPORTED TO THE ED ALTERED MENTAL STATUS PT WOKE")





- Slides: 30
Sock Removal Shock: Lower Extremity Wounds in Dialysis Patients DEB KOZENY, NP, CWS
Disclosures No disclosures or conflict of interest
Objectives Evaluate frequent causes of foot wounds in the dialysis patient: Diabetes, PAD, venous, mixed Discussed how to evaluate what type of wound may be present Discuss treatment options based on the diagnosis: i. e. surgical versus medical intervention Use case studies to discuss how providers in the dialysis unit can assist in the assessment and care of wounds in the dialysis patient
Case Study Pt is a 48 y/o male with ESRD on dialysis Pertinent past medical history At initial appointment patient reported discoloration on the plantar heel surface and was not sure he even had a wound. Had previous right fifth toe amputation due to osteomyelitis Had been fitted for diabetic shoes with custom inserts but preferred to wear Nike tennis shoes Diabetes mellitus Type 2 Retinopathy affecting both eyes Bilateral peripheral neuropathy that extends to below the knee Bilateral foot drop Gait abnormality Does not use walker as instructed Balance problems Reports fasting blood sugar of 130 History of previous diabetic foot ulcer on the same foot Eats only one meal a day and has frequent high carb snacks
Incidence of Foot Ulcers in ESRD 25 -30% of all diabetic pts developed kidney damage 4 -17% of diabetic patients will experience ESRD at 20 yrs. and 16% at 30 yrs. Diabetic nephropathy is the most common cause and primary etiology of endstage renal disease US renal data system - diabetes is the precipitating factor for ESRD in 45% of patients Foot ulcerations were 5 x more likely in diabetics on dialysis versus diabetics who had chronic kidney disease There is a 2 fold increase in the prevalence of PAD and amputations in dialysis treated patients Behan, S. , Reyzelman, A. Understanding the Impact of End-stage Renal Disease on Healing in Patients with Diabetes. Podiatry Today, March 2018
Case study Pt comes to clinic 10 days later and now has worsening heel wound and new wound on dorsal ankle, cause? ? Tendon exposure Admitted to hospital for IV AB MRI shows soft tissue swelling, no osteomyelitis Vascular studies obtained, why?
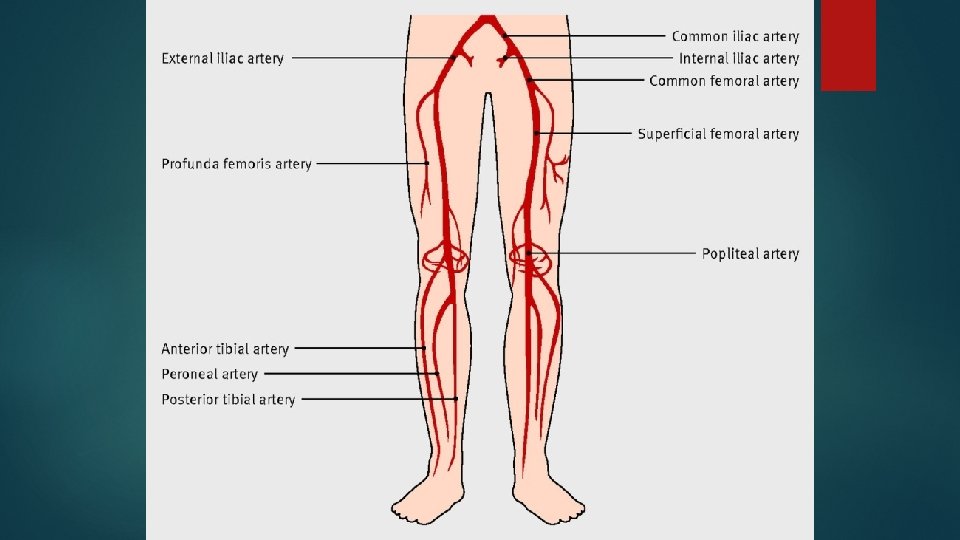
Arterial evaluation
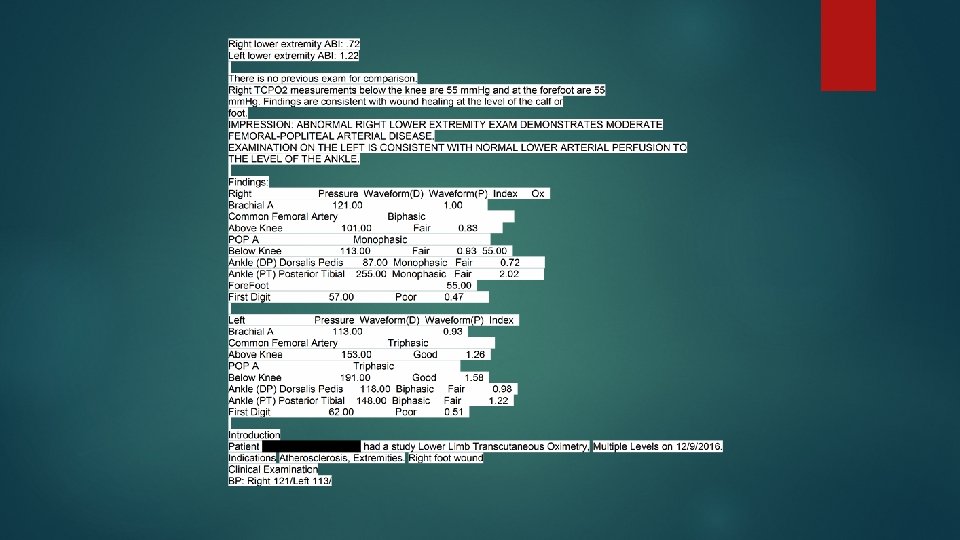
Case Study ABI’s Impression Single - level lower extremity arterial single-level pressures and PVR waveforms were performed. Right lower extremity ABI: 1. 94 Left lower extremity ABI: 1. 94 Right TCPO 2 measurements below the knee are 17 mm. Hg and at the forefoot are 9 mm. Hg. Left TCPO 2 measurements below the knee are 17 mm. Hg and at the forefoot are 3 mm. Hg. Findings are equivocal and readings are not in a range in which wound healing can be predicted at the level of the calf or the foot. Question accuracy due to patient movement. When compared to previous exam done on March 28 th, 2016 this exam is significantly changed. IMPRESSION: ABNORMAL RIGHT LOWER EXTREMITY EXAM DEMONSTRATES SEVERE TIBIAL ARTERIAL DISEASE. EXAMINATION ON THE LEFT IS CONSISTENT WITH NORMAL LOWER ARTERIAL PERFUSION TO THE LEVEL OF THE ANKLE. THERE IS ARTIFICIAL ELEVATION OF ANKLE-BRACHIAL INDICES, SUBSEQUENTLY THEY MAY BE NON-RELIABLE. THIS CAN BE SEEN IN DIABETICS WITH MEDIAL VASCULAR CALCIFICATION. TOE PULSE VOLUME RECORDINGS APPEAR FAIR ON THE RIGHT AND GOOD ON THE LEFT. TOE BRACHIAL INDICES ON THE RIGHT ARE 0. 60 AND ON THE LEFT ARE 0. 95.
Case study Impression Arterial Duplex Examination using B-mode, color flow and spectral Doppler was performed. Exam was technically difficult and visualization was limited due to severely calcified plaque, unable to visualize flow in lumen due to heavy shadowing. There is no previous exam for comparison. IMPRESSION: ABNORMAL RIGHT LOWER ARTERIAL EXAMINATION WITH AN OCCLUSION NOTED IN THE PROXIMAL ANTERIOR TIBIAL ARTERY. ABNORMAL RIGHT LOWER ARTERIAL EXAMINATION WITH >50% STENOSIS NOTED IN THE ANTERIOR TIBIAL ARTERY. ABNORMAL LEFT LOWER EXTREMITY ARTERIAL EXAMINATION, THERE WAS <50% SCATTERED ATHEROSCLEROTIC PLAQUE THROUGHOUT THE ARTERIAL CIRCULATION.
PAD and ESRD 35% of adult patients on hemodialysis have PAD Kidney disease increases the incidence of PAD threefold versus patient’s without kidney disease Severity of PAD worsens as kidney disease progresses Coexistence of end-stage renal disease and diabetes exacerbates PAD, affecting 1 out of 3 patients, is related to both atherosclerosis and accelerated calcification of blood vessels Kidney disease leads to increasing calcium and phosphate deposits into the blood vessels Secondary hyperparathyroidism contributes to promoting calcification and advancing PAD Behan, S. , Reyzelman, A. Understanding the Impact of End-stage Renal Disease on Healing in Patients with Diabetes. Podiatry Today, March 2018
Case study Pt underwent right lower extremity angiogram and was found to have stenosis in the proximal popliteal artery with patent peroneal and PT and mid AT occlusion Was treated with angioplasty Underwent debridement of both wounds: The wound on the anterior ankle was down to the tendons in some places. The heel wound was into the subcutaneous fat Returns to the wound clinic, unable to visualize the heel wound, elevating his leg infrequently, nutrition is still poor, eating 1 meal a day so arranged for home health care which the patient reluctantly agreed to. Remains at high risk for limb loss
Case study
Case study
Case Study Referred to plastic surgery for wound debridement and grafting – underwent surgical debridement and application of primatrix to the anterior right ankle wound and epi-fix to a heel wound Problem list contains > 30 diagnoses Reinforced need to increase protein in diet, offload right foot and follow plan of care
Case study
End-stage renal disease other causes for poor wound healing Uremic pruritus- due to degenerating sweat glands, chronic itching develops which compromises the skin delaying wound healing and promoting wound development Calciphylaxis- is a thrombolic event that provokes ischemia and tissue infarction, cause of the embolic event in calcified vessels is not known but the 1 year mortality rate is greater than 50% secondary to sepsis from ulcerations Hemodialysis – decrease in TCPO 2 during and after dialysis has been reported with studies showing declining trend for at least 4 hours after dialysis, thought to be related to systemic hypoxemic state but also the fluid shift produced to preserve central circulation by decreasing peripheral blood flow, this leads to decrease skin perfusion and slows delivery of nutrients crucial for wound healing Behan, S. , Reyzelman, A. Understanding the Impact of End-stage Renal Disease on Healing in Patients with Diabetes. Podiatry Today, March 2018
End-stage renal disease other causes for poor wound healing Low serum zinc levels are present in 40 -78% patients with chronic kidney disease, related to coincidental excretion infiltration of zinc during hemodialysis as well as decreased absorption in the gut and increase intake due to dietary restrictions Zinc assists in wound healing by protecting against bacterial toxins and reactive oxygen species and is also a cofactor for the enzymatic pathway that improves autolytic debridement and epidermal cell migration Protein is a required nutrient to promote wound healing, which is decreased in end-stage renal disease due to increased protein catabolism, protein malnutrition also impacts the immune system by inhibiting phagocytosis increasing susceptibility to infection Behan, S. , Reyzelman, A. Understanding the Impact of End-stage Renal Disease on Healing in Patients with Diabetes. Podiatry Today, March 2018
End-stage renal disease other causes for poor wound healing Immune system – depressed with end-stage renal disease, is not only caused by protein deficiency but by the presence of uremic toxins increasing risk of infection in wounds Anemia – renal damage and end-stage renal disease affects the production of RBCs and the perception that the body is even hypoxic, this impairs perfusion of oxygen nutrients to the wound site Neuropathy –uremia is an independent risk factor for the development of neuropathy which affects 60 -100% of patients with end-stage renal disease. Similar to diabetic peripheral neuropathy with symptoms of paresthesias, diminished deep tendon reflexes, weakness and muscle atrophy Behan, S. , Reyzelman, A. Understanding the Impact of End-stage Renal Disease on Healing in Patients with Diabetes. Podiatry Today, March 2018
93 Y/O FEMALE • INITIAL WOUND: RT LATERAL ANKLE PRESENT FOR OVER YEAR • ROOKE BOOTS TOO EXPENSIVE, NOT COVERED BY INSURANCE (>$200) • LIVES WITH ADULT DAUGHTER (PRIMARY CAREGIVER) • STANDS, PIVOT TRANSFERS, URINARY INCONTINENCE (WEARS PAD) • SPENDS TIME ON COUCH AND BED; LIMITED AMBULATION, WHEELCHAIR • GOOD APPETITE, STABLE WEIGHT • HISTORY OF HF WITH EDEMA, DEMENTIA, FALLS, SKIN TEARS, CIRRHOSIS WITH ASCITES (ETOH), HTN, PAD • HOME HEALTH WEEKLY SENT FOR VASCULAR STUDIES: ABNORMAL CONSERVATIVE WOUND MANAGEMENT LIGHT COMPRESSION (TUBIGRIP), ROOKE BOOTS, BETADINE HOSPITALIZATIONS FOR EXACERBATION OF HF (RECOMMENDED HOSPICE IN HOSPITAL) PCP ADDED ACE WRAP TO RIGHT FOOT SECONDARY TO INCREASED EDEMA
Initial 3 weeks post 3 weeks later 2 wks. later
Case Study (continued) DUE TO WORSENING WOUNDS WITH TENDON EXPOSURE ON THE DORSAL RIGHT FOOT UNDERWENT ANGIOGRAM ON 2/20/17. NEEDED KIDNEY PROTECTION DUE TO CREATININE WAS 1. 42 WITH A GFR 35 ON 2/13/17 PROCEDURE: 1) LEFT FEMORAL ARTERY PUNCTURE AND ABDOMINAL AORTOGRAM 2) RIGHT LOWER EXTREMITY RUNOFF 3) ANGIOPLASTY OF THE RIGHT DISTAL SUPERFICIAL FEMORAL ARTERY AND POPLITEAL ARTERY FOR OCCLUSION 4) PLACEMENT OF 6 MM STENTS FROM THE BELOW THE KNEE POPLITEAL ARTERY TO ABOVE THE ADDUCTOR CANAL 5) POST ANGIOPLASTY OF STENTS WITH 4 MM BALLOON 6) PLACEMENT OF AN ANGIO-SEAL CLOSURE DEVICE IN THE LEFT FEMORAL ARTERY DUE TO NEEDING STENTS PLACED WAS STARTED ON PLAVIX ALONG WITH ASA
Case Study(continued) ON 2/28/17 REPORTED TO THE ED ALTERED MENTAL STATUS PT WOKE UP AND DIDN'T FEEL GOOD. PT'S DAUGHTER CALLED 911, PER SQUAD STROKE SCALE NEGATIVE. PT STATED "MY DAUGHTER THOUGHT I NEED TO COME HERE" PT ALERT AND ORIENTED X 4 GI BLEEDING IN THE ER THE PATIENT WAS FOUND TO HAVE SYSTOLIC BLOOD PRESSURE 69 AND HAD 2 LARGE MELANOTIC STOOLS WITH A HGB ON ADMISSION OF 8. 0. THE PATIENT WAS GIVEN 2 L IV FLUID AND 1 UNIT OF PACKED RED BLOOD CELLS. UNDERWENT EGD ON 3/1/17 - 8 MM ANTRAL ULCER WITH CLEAN BASE STOPPED PLAVIX AND STARTED ON ASA 325 MG DAILY WITH FOOD
New wound Left Trochanter May 2017 Rt lateral foot May 2017 Rt Dorsal foot Nearly closed July 2017
12. 29. 2017
Medications and Wound Healing Antihypertensives Anticoagulants Nicotine Antibiotics – sulfa, penicillin Vasoconstrictors OTC products Herbal supplements Steroids Vitamins, minerals Hormones
What can I do? Pay attention to high risk patients – are they wearing proper footwear, using ambulatory aids, controlling edema, diabetes under control ( FBS <180 ), personal hygiene, prevent vs treat, vision problems, dexterity What is their nutritional status - consider food log, technology aids, monitoring weight, lab results Social issues – play a major role in wound healing Adherence – do they have the skill set to perform wound care, do they have the supplies they need, are they performing wound care as ordered Early recognition of presence of wound(s) – examine pts feet/extremities in private exam area, need early referral to wound care, vascular surgery or other appropriate provider, what is the involved area(s) skin/wound color, pulse status, wound size, odor, drainage, edema, how long has wound been present, new onset or recurrent, callous presence, nail care
References Behan, S. , Reyzelman, A. Understanding the Impact of End-stage Renal Disease on Healing in Patients with Diabetes. Podiatry Today, 2018, 31(3): 68 -78. Beitz, J. M. Pharmacological Impact (“Breaking Bad”)of medications on Wound Healing and Wound Development: A Literature–based Overview. Ostomy Wound Management 2017; 63 (3): 18 -35 Hess, C. T. Clinical Guide to Skin and Wound Care, Seventh Edition. Lippincott Williams & Wilkins, Philadelphia, 2013. Livingston, M. , Wolvos, T. Scottsdale Wound Management Guide, Second Edition. HMP Communications, LLC, 2015