Prevention of UTI in children with VU reflux








 - studies § Background: ABP recommended for all grades VUR §")




















 VUR (severe")

- Slides: 44
Prevention of UTI in children with VU reflux: management controversies Moshe Efrat MD September 2006
(Vesicoureteral Reflux (VUR § Retrograde passage of urine from bladder to § upper urinary tract VUR = most common urologic abnormality in kids § 1% newborns § 30 - 45% of children with UTI § UTI (upper) = most common serious bacterial infection of children in the developed world in the age of conjugate pneumococcal and H. flu vaccines (Israel is not there yet!! – why? )
Two clinical presentations VUR § Prenatal: § male > female, VUR diagnosed prenatally (by § US) § Severe VUR common § Significant rates spontaneous resolution, but § Renal hypoplasia and dysplasia frequent § Increased risk renal failure and hypertension Postnatal: § Mostly female § Presents as febrile UTI § Spontaneous resolution is a function § of age and grade § and if 1 or 2 sided
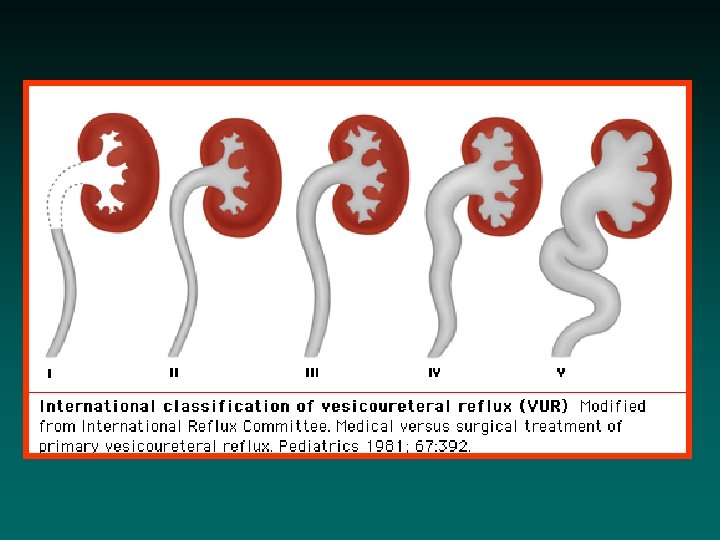
VUR - grading § GRADING — The International Reflux Study Group § § § standardized grading the severity of VUR based on findings from a contrast voiding cystourethogram (VCUG). Grade I — Reflux only fills the ureter without dilation. Grade II — Reflux fills the ureter and the collecting system without dilation. Grade III — Reflux fills and mildly dilates the ureter and the collecting system with mild blunting of the calyces. Grade IV — Reflux fills and grossly dilates the ureter and the collecting system. One-half of the calyces are blunted. Grade V — Massive reflux grossly dilates the collecting system. All the calyces are blunted with a loss of papillary impression and intrarenal reflux may be present. There is significant ureteral dilation and tortuosity.
Principles of management § Premise: VUR can cause upper UTI by bringing bacteria to the kidneys § Results: renal scarring, loss of parenchyma reflux nephropathy: § Potential for hypertension, decreased renal function, proteinuria, renal failure/ end stage renal disease § Management: based on § Identification of kids with VUR § Prevention of renal damage due to reflux
How to prevent damage due to VUR? § Medical vs surgical approach § Not clear which is more effective! § Medical: § VUR resolves spontaneously by age 4 -5 years § Continuous antibiotics sterile urine § VUR with sterile urine is assumed benign § Most appropriate antibiotics: TMP-SMX, nitrofurantoin § Not β-lactams!? !? Why? … § Increased bacterial resistance
More concerns about medical therapy § Long-term antibiotics may complications: § minor to severe - including bone marrow suppression, Stevens-Johnson syndrome § Adherence (compliance) § Breakthrough infection § Need to monitor reflux with either VCUG or radionuclide cystography (RNC), both with discomfort and radiation
The main controversy § Does antibiotic prophylaxis of kids with VUR really prevent recurrent upper UTI and concomitant renal scarring? § Over the last 5 -6 years this has been increasingly questioned / debated and to a certain extent studied…
Antibiotic prophylaxis (ABP) - studies § Background: ABP recommended for all grades VUR § Most studies to date: compare [ABP with surgery] to ABP alone, or compare ABP with surgery § Meta-analysis (Wheeler, et al, Arch Dis Child 2003; 88: 688 -594): 1 randomized, controlled study found no difference in UTI risk with ABP, either continual or intermittent, vs no ABP § No large, randomized, prospective trials comparing ABP+ with ABP- in VUR!!!
Aims § Evaluate the role of VUR in affecting frequency and severity of UTI and renal scarring after APN § Determine whether ABP reduces frequency and/or severity of UTI and/or prevents renal parenchymal damage in patients with mild-moderate VUR (grades I, III only)
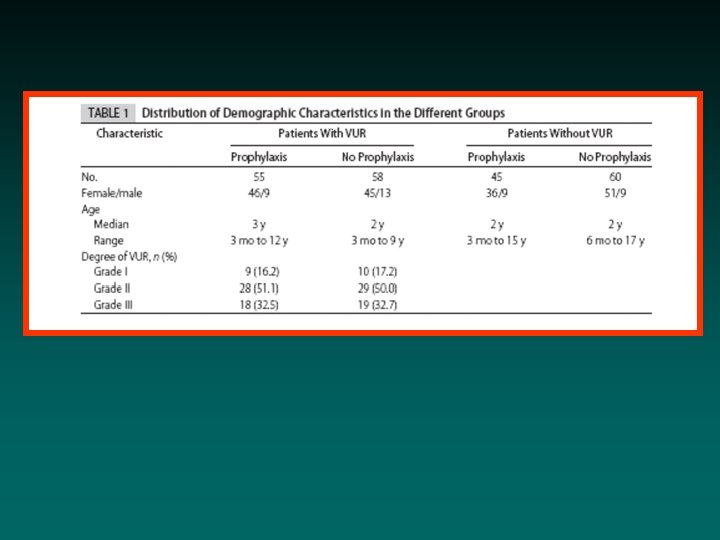
The study § Randomized, controlled study § N= 236 children, 3 months – 18 years § APN = acute pyelonephritis: pyuria, fever, positive culture (>105) + DMSA confirmation § All tested for VUR by VCUG 2 groups: § 113 VUR grades I-III and 115 no VUR § After initial treatment for APN, both groups randomized: +/- antibiotic prophylaxis (ABP)
Conclusion: antibiotics do not prevent APN nor renal scarring in patients with mild or no VUR!!! Results: § Overall UTI recurrence 20. 1% § - ABP: recurrence 22. 4% VUR, 23. 3% no VUR (NS) § +ABP: recurrence 23. 6% VUR, 8. 8% no VUR (NS, but close, p=0. 63) § Most recurrences at 9 -12 months, most cystitis (DMSA nl), APN only 5. 5% § No clear-cut advantage for +ABP § All recurrences were with resistant bacteria! § More APN in +VUR than in -VUR (8 vs 4, but NS)
Results, continued § 6/8 recurrent APN were in VUR grade III § 2/8 in grade II, none in grade I § 4 recurrences in non-VUR (2 ABP+, 2 ABP-) § Cystitis also VUR III, II >>VUR I Renal scars: § Only 5. 9% developed scars (1 year F/U only!) § 7 VUR+, 6 VUR- (NS) § Similar scarring rates ABP+ and ABP- (NS) § Increased scarring with increase grade VUR (NS) § No difference in scarring in VUR vs non-VUR
Conclusions at 1 year endpoint: 1. Antibiotics do not prevent cystitis, APN or renal scarring in patients with mild to moderate or no VUR!!! 2. ABP UTIs with resistant bacteria 3. ABP in VUR+ more APN than in VUR(NS)
: The Editorial
Fact or fantasy I § The study is highly problematic: § 1 year follow-up only § 1 year follow-up required, no ITT analysis in those not completing 1 year § Low incidence APN § Low rate renal scarring § Non-standardized ABP: §either trimethoprim-sulfamethoxazole (TMP-SMX) or nitrofurantoin §no placebo given to controls
Fact or fantasy II § Therefore, too few patients, too short a time § period, and maybe the wrong population (VUR I -III), maybe wrong antibiotics - to reach conclusions of significance… § Current study: trend for more UTI and more scarring with increasing grades of VUR… § III > I Important: no evaluation of severe VUR (grades IV, V) § Therefore results are not applicable to these patients !
Discussion § UTI pathogenesis related to bacterial binding to uroepithelial receptors § No reason to think that VUR increases UTI incidence, but… § Reasonable to think that VUR increases APN (vs lower UTI) incidence in those with propensity for UTI = trend but not significant in some studies § Scarring is a function of APN and not sterile reflux: good evidence exists
ABP should prevent recurrent UTI – few good data to support this! § 2 potential barriers to successful ABP for UTI: § Adherence (compliance) difficult over years, also antibiotic adverse effects, though rare, increase with exposure time §Maybe recurrences mostly at 9 -12 months indicate decline in adherence? § Emergence of antimicrobial resistance
? Which drugs are used § Nitrofurantoin or TMP-SMX § Theory: absorption high in the in GI tract - § colon flora not “exposed” = protected from antibiotics little induction of resistance § Problem – areas where TMP-SMX cannot be used: high % GI flora resistant (Israel? ) Other agents (e. g. β-lactams) are theoretically poor choices § Colonic bacteria exposed to low AB levels § Within weeks GI colonized primarily with bacteria inherently or newly resistant
Another issue § Is there any proof that prevention of UTI by continuous ABP prevents scarring better than very early initiation of therapy for APN? §No studies performed
? Possible solutions § Use rotating ABP schedule parallel to ABP for chronic lung disease, switching drug q 2 -4 weeks §Few data for UTI, some potentially encouraging § Use non-antibiotic prophylaxis e. g. methenamine mandelate § When urine p. H <6, methenamine formic acid (like formaldehyde) §Problem: urine acidification required
Suggestions? § Additional studies required: § To clarify ABP use in VUR grades I, III § Larger, better designed, longer F/U, § ITT… § To study VUR grades III, IV, V Until new data: § For all (? ) VUR (severe > moderate > mild), continue using ABP (or surgery for high grade, non-resolving VUR) § If TMP-SMX inappropriate epidemiologically, maybe nitrofurantoin should be used > others
? What about previous studies § Not a lot of data § Good systematic review of data available up to 2005…
Our questions: antibiotics, yes or no, which, and when? § Medical vs surgical therapy? § Not clear! § Meta–analysis (Wheeler, et al, Arch Dis Child 2003; 88: 688 -594): found 7 randomized, controlled studies, ABP vs surgery, n = 859 § 4 studies: no difference after 5 years § 2 studies: less febrile UTI, at 5 years, surgery (10%) vs ABP (22%) §But no difference in scarring!
Meta-analysis, continued § 4 studies: no differences in scarring after 5 years § 5% overall risk of new scars by DMSA § 4 studies: no differences in renal growth § 2 studies: no difference in hypertension or end-stage renal disease § Lack of information about surgical vs medical adverse events!!
Conclusions § 9 reimplantations required to prevent 1 febrile UTI! § No reduction in rate of renal scarring! § Hardly seems wise to prefer surgical therapy § Except. . . ?
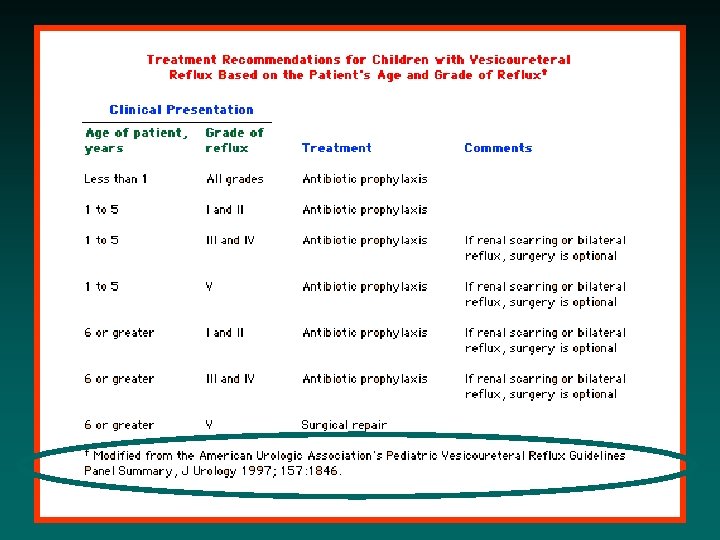
Rationale AUA guidelines § Low grade VUR, VUR in very young kids good chance spontaneous resolution so prefer ABP § The older kids get or the higher grade the VUR, ABP still recommended but surgery is an option especially if bilateral disease or renal scarring exists § Only in children ≥ 6 years old with grade V VUR is surgery preferred since the likelihood of spontaneous resolution is very low
…If ABP follow-up § Close monitoring to identify breakthrough § Urine-analysis and cultures whenever UTI possible § Surveillance cultures q 3 -4 months § RNC > VCUG monitoring of VUR ~ yearly
…So, in conclusion § Until new data: § For all (? ) VUR (severe > moderate > mild)… § continue using ABP §or surgery for high grade, nonresolving VUR § Nitrofurantoin preferred!?
!Thanks §Questions? §Comments? §Protests?