Pediatric infectious diseases Vaccination programs Prof Dr Gyrgy





, streptococcal antigen test (specificity: >95%)")

")




")


")


 Inflammation of the subcutaneous connective tissue – may lead to abscess n")

 n n Paramyxovirus, RNA virus 10 -14 days incubation Rash: retroauricular, temporal")
 (RNA virus, maculopapulous rash, Koplik spots)")
")
 n n Togavirus, RNA Painful lymphadenopathy: retroauricular, cervical, occipital region: Theodor-")
 (RNA virus, Togaviridae – Rubivirus, maculopapular rash, occipital lymphadenopathy)")


 (Human Herpesvirus-6, maculopapular rash)")
")
 (Varicella-Zoster virus/HHV -3, vesicles)")
 n n n Incubation period: 10 – 21 days (1415 days) Complications:")
 Treatment: aciclovir")
")

")

")

")





 Birth Rotavirus 6 w, 3 mo (Hepatitis")
")

, or bacterial endocarditis (BE), is")



- Slides: 53
Pediatric infectious diseases. Vaccination programs Prof. Dr. György Fekete
Localizing symptoms n n n n n Skin Upper respiratory Lower respiratory Genitourinary Gastrointestinal CNS Skeletal Cardiovascular Hepatic
Characteristics in infants and children n n Neonates, infants: non-specific initial symptoms (irritability, lethargy, poor feeding) Specific rashes Sites of infection Prevention: vaccination/ immunization
Group A Streptococcal infections n n n n n Acute pharyngitis Otitis media Paranasal sinusitis Impetigo, pyoderma Cellulitis Scarlat fever Pneumonia Septic arthritis Osteomyelitis Meningitis
Streptococcal tonsillopharyngitis n n 5 - 15 years Beta –haemolysing Streptococcus spp. Other bacteria: S. aureus, H. influenzae positive results in throat microbiological cultures are not pathogenic. Antibiotic treatment is not necessary! Aminopenicillin antibiotics are not recommended –possible infectious mononucleosis
Tonsillopharyngitis streptococcica n n Diagnosis: microbiology (sensitivity: 90 -95%), streptococcal antigen test (specificity: >95%) Treatment: oral Penicillin, 10 days
Complications n n Abscess of the cervical lymphnodes Peritonsillar abscess Sepsis Late: rheumatic fever, acute diffuse glomerulonephritis
Scarlet fever (Group A Streptococcus, erythrogenic toxin, /pyrogenic exotoxin/, fine papular rash)
Scarlet fever n n n Incubation period: 1 – 4 days Skin: diffusely erythematous („sandpaper rash): confluent maculo-papulous – 6 – 9 days Petechiae on the soft palate, on the upper abdomen and trunk Circumoral pallor Desquamation (peeling) on the face: end of the first week, then generalized Strawberry tongue
Scarlet fever
Scarlet fever
Scarlet fever n n Abdominal pain, vomiting Treatment: oral Penicillin, 10 days
Kawasaki disease (Multisystem vasculitis)
Kawasaki disease n n Coronary aneurism / dilatation < 5 years, incidence: 3 – 6: 100 000 Fever, non – suppurative conjunctivitis, cheilitis, strawberry tongue, polymorphic rash, pharyngitis, lymphadenopathy, peeling on the extremities Treatment: high dose IVIG (2 g/kg bw. ) + aspirin (80 -100 mg/kg bw. )
Erysipelas n n n Superficial and deep inflammation of the skin, demarkated rash Invasive infection Streptococcus pyogenes, Staphylococcus aureus Complication/ infants: sepsis Treatment: penicillin, clindamycin
Erysipelas (Group A Streptococcus, acute cellulitis and lymphangitis)
Impetigo n n Papule, vesiculation, then it breaks Denuded area, covered by a honeycolored crust
Impetigo n n n 2 – 5 years Streptococcus pyogenes Staphylococcus aureus Local treatment Systemic: antibiotic therapy
Cellulitis (phlegmone) Inflammation of the subcutaneous connective tissue – may lead to abscess n Streptococcus pyogenes, Staphylococcus aureus, Haemophilus influenzae (<2 yrs) n Therapy: penicillin+ clindamycin n
Infectious diseases with rash Stadium incubationis: in generalno symptom n Stadium prodromum: non-specific symptoms n Stadium floritionis n
Measles (Rubeola) n n Paramyxovirus, RNA virus 10 -14 days incubation Rash: retroauricular, temporal region, then on the face - maculopapulous exanthemes Complications: encephalitis, cerebellitis, subacute sclerotizing panencephalitis
Measles (Rubeola) (RNA virus, maculopapulous rash, Koplik spots)
Measles (Rubeola)
Rubella (German measles) n n Togavirus, RNA Painful lymphadenopathy: retroauricular, cervical, occipital region: Theodor- Klatsch symptom Peeling Congenital rubella syndrome
Rubella (German measles) (RNA virus, Togaviridae – Rubivirus, maculopapular rash, occipital lymphadenopathy)
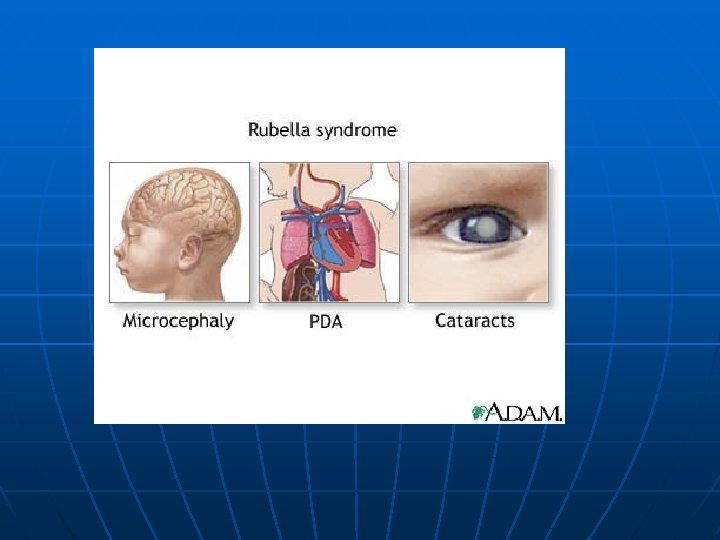
Congenital rubella syndrome n n Infection of seronegative mother during pregnancy Risk of fetal infection • • I. trimenon: 75 -90% II. trimenon: 20 -40% III. trimenon: 25 -50% Fetal lesion n 1 -8. gest. week: 80% 9 -12. gest. week: 30% 13 -20. gest. week: 10%
Congenital rubella syndrome n Gestation • 14 - 60. days: embryopathy – cataracta, microphthalmia, hearing loss, congenital heart disease, microcephalus, thymus hypoplasia Rubella vaccination is prohibited during pregnancy!
Roseola (exanthema subitum) (Human Herpesvirus-6, maculopapular rash)
Varicella (chickenpox)
Varicella (chickenpox) (Varicella-Zoster virus/HHV -3, vesicles)
Varicella (chickenpox) n n n Incubation period: 10 – 21 days (1415 days) Complications: secondary bacterial infection – streptococcal toxic shock syndrome Pneumonitis
Progressive varicella (toxic) Treatment: aciclovir
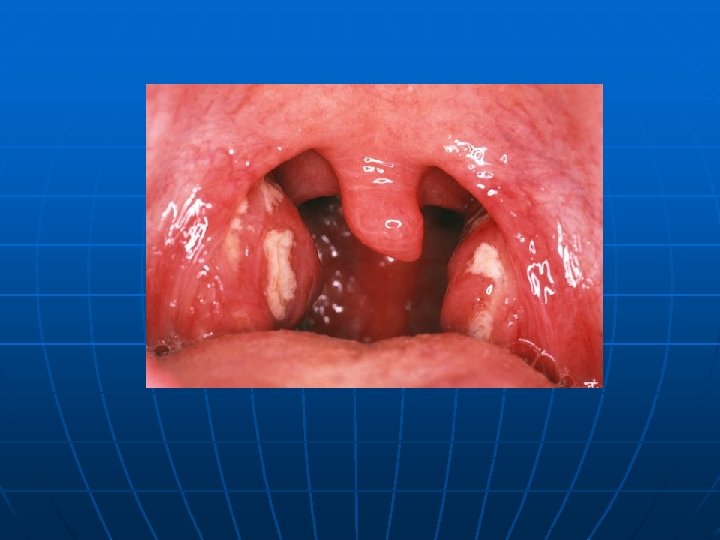
Infectious mononucleosis (Epstein- Barr virus infection, CMV, adenovirus, toxoplasma)
Infectious mononucleosis n n n n Incubation period: 4 – 8 weeks Incidence: <10 years: <1: 1000 10 – 19 years: 6 -8 : 1000 Fever, lymphadenopathy, pharyngitis Hepato –splenomegaly Jaundice Rash Atypic lymphocytes
Infectious mononucleosis (Epstein-Barr virus, enanthema=pharyngeal petechiae)
Infectious mononucleosis
Lyme disease (Borrelia Burgdorferi, erythema chronicum migrans)
Lyme borreliosis n n Skin, joints, CNS, heart Erythema migrans – regional lymphadenopathy Treatment: oral doxycyclin, amoxicillin, cefuroxim-axetil 10 days Ceftriaxon iv.
Tetanus (Clostridium tetani exotoxins)
AIDS n n n Occurrence is rare in children 80% intrauterine, intra partum, breast feeding, 10 - 15% blood and blood products, 5% unknown origin Risk of children of HIV infected mother: 20 -40%
AIDS/ clinical forms n n Slowly progressing form: intra partum, post partum infection Frequent and severe infections after latency (1 -2 yrs) Lymphoid interstitial pneumonitis, hypergammaglobulinemia Death before the age of 6 yrs in 60%
AIDS / prevention n n Antiviral treatment of infected mother during pregnancy Isolation of newborn baby from infected mother No breast feeding BCG vaccination is prohibited!
AIDS / clinical forms n n Rapidly progressing: intrauterine infection Repeated, severe infections with classical and opportunistic pathogens (Pneumocystis carinii, Cryptosporidium, Candida, HSV, EBV, CMV) Failure to thrive, enlargement of parotid gland, lymphadenopathy, cortical atropy, demyelinisation of the brain, death at the age of 3 yrs BCG sepsis!
Immunization schedule/ Hungary n n BCG Birth Hepatitis B 1 12 yr n H. infl. Typ b 2, 3, 4, 18 mo DTP+IPV 2, 3, 4, 18 mo, 6 yr PCV 13 x 2, 4, 12 mo MMR 15 mo, 12 yr HPV 12, 13 yr /females/ Recommended: varicella, hepatitis A n X = pneumococcal conjugate vaccine n n n European Centre for Disease Prevention and Control
Immunization schedule/ Norway n n n (BCG) Birth Rotavirus 6 w, 3 mo (Hepatitis B 1) Birth n H. infl. Typ b 3, 5, 12 mo DTP+IPV 3, 5, 12 mo, 7 yr, 15 yr PCV 13 x 3, 5, 12 mo MMR 15 mo, 11 yr HPV 12 yr /females/ n X = pneumococcal conjugate vaccine n n n European Centre for Disease Prevention and Control
Types of vaccines n n n Live attenuated viruses (measles, mumps, rubella, varicella, polio) Inactivated viruses (polio, hepatitis B, influenza) Inactivated bacteria (pertussis, diphtheria, tetanus, H. influenzae type b, pneumococcus)
Non- mandatory vaccines n Polysaccharid vaccines • Meningococcus A, C, W-135, Y serotypes • Pneumococcus, 13, 23 serotypes, 7 serotypes n n n n Hepatitis- A, A+B Human papillomavirus (HPV) Influenza Tick - borne encephalitis Rotavirus Chickenpox (varicella) RSV
Dental Procedures and Infective Endocarditis n Infective endocarditis (IE), or bacterial endocarditis (BE), is an infection caused by bacteria that enter the bloodstream and settle in the heart lining, a heart valve or a blood vessel
Antibiotic prophylaxis to prevent endocarditis I. n n n n For all patients with significant cong. heart defect (unoperated, palliated or repaired) Rheumatic valve lesions Prosthetic heart valves Mitral heart prolapse Subaortic stenosis Transvenous pacemaker leads Previous endocarditis NOT indicated: isolated secundum ASD, repaired sec. ASD and VSD 6 mo after patch placement, ligated PDA 6 mo after repair
Oral-dental procedures requiring endocarditis prophylaxis n n n n Extractions Periodontal procedures Dental implant placement Root canal surgery beyond the apex Subgingival placement of orthodontic bands but not brackets Prophylactic cleaning of teeth / bleeding is anticipated Intraligamentary local anesthetic injections
Antibiotic prophylaxis to prevent endocarditis II. n n n During dental / respiratory procedures : oral amoxicillin, 50 mg/kg 1 hr before During gastrointestinal/ genitourinary procedures: oral amoxicillin or parenteral ampicillin + gentamicin, iv. 30 min before For patients allergic to penicillin: clindamycin, 20 mg/kg