MAKATI MEDICAL CENTER MEDICAL GRANDROUNDS MARCH 12 2009




 Dx: Esthesioneuroblastoma (olfactory neuroblastoma) S/p craniofacial")
 (+) mass on R cheek (+)")
 (+) L submandibular mass 1 year")

 easy fatigability and malaise (+) bipedal")
 upward rolling of eyeballs, stiffening of")
 fever (-) rashes, sores, itchiness (-)")
 HPN, DM, BA, PTB n (-) allergies n")
 smoker n (-) alcoholic beverage drinker n (-) illicit drug use")
 HPN n (-) DM n (-) Asthma n (-) CA n")

 facial & back acne (+) cushingoid facies (+) 4")
 facial & back acne (+) cushingoid facies (+) 4")
 buffalo hump")

 grade 2 bilateral pitting edema, (-) atrophy of")









 9/20 9/22 Na 137 143 K 1. 9 2. 0 2. 8")
 Plasma aldosterone: 14. 49 ng/d. L n Plasma renin: 0. 259 ng/m.")




 n Plasma ACTH: 304. 12 pg/m. L")










 increased basal cortisol production (2) dependence of cortisol")




 n MRI/MRA OF BRAIN & INTRACRANIAL VESSELS 1. Anterior and posterior falcine")
 n CT SCAN OF UPPER ABDOMEN (PLAIN & IV CONTRAST) - Non-specific")
 n MRI OF THE SELLA TURCICA - Enlarged sella turcica with the")
- Slides: 62
MAKATI MEDICAL CENTER MEDICAL GRANDROUNDS MARCH 12, 2009 ESTHESIONEUROBLASTOMA and CUSHING’S SYNDROME ARIANNE SY-UMALI, MD PRESENTOR
OBJECTIVES n n n To discuss a case of Cushing’s syndrome 2 o to ectopic ACTH secretion 2 o to metastatic Esthesioneuroblastoma. Approach to diagnosis of a patient with Cushing’s syndrome. Management of a patient with ectopic ACTH secretion.
PATIENT DATA M. C. n 42 y/o n Female n
CHIEF COMPLAINT n Stiffening of extremities
HISTORY OF PRESENT ILLNESS 7 years PTA (2001) Dx: Esthesioneuroblastoma (olfactory neuroblastoma) S/p craniofacial resection with biopsy S/p cobalt therapy
HISTORY OF PRESENT ILLNESS 3 years PTA (2005) (+) mass on R cheek (+) facial swelling (+) weight gain, polyuria, polydipsia, nocturia, occasional difficulty swallowing, HA, diplopia, difficulty sleeping (-) body weakness, bone pains, excessive hair loss/growth, change in menstrual cycle
HISTORY OF PRESENT ILLNESS 2 years PTA (2006) (+) L submandibular mass 1 year PTA (2007) Consult MRI with biopsy of masses Bx: Esthesioneuroblastoma metastatic to the R maxillary and L submandibular areas Lost to follow-up
2002 2006
HISTORY OF PRESENT ILLNESS 4 days PTA (+) easy fatigability and malaise (+) bipedal edema (-) palpitations, dyspnea, PND, orthopnea 1 day PTA Rx: Furosemide 40 mg/tab x 1 dose
HISTORY OF PRESENT ILLNESS 5 hours PTA (+) upward rolling of eyeballs, stiffening of extremities x 5 mins (-) drooling, bowel/bladder incontinence Rushed to a local hospital Transfer ADMISSION
REVIEW OF SYSTEMS n n n n (-) fever (-) rashes, sores, itchiness (-) tinnitus, hearing deficits, ear aches (-) sorethroat, bleeding gums, hoarseness (-) nausea, vomiting, diarrhea, constipation (-) easy bruising or bleeding (-) heat or cold intolerance, excessive sweating, tremors (-) nervousness, tension, memory impairment
PAST MEDICAL HISTORY (-) HPN, DM, BA, PTB n (-) allergies n
PERSONAL/SOCIAL HISTORY (-) smoker n (-) alcoholic beverage drinker n (-) illicit drug use n (-) steroid use n
FAMILY HISTORY (-) HPN n (-) DM n (-) Asthma n (-) CA n
PHYSICAL EXAMINATION BP 130/90 CR 68 RR 19 To 37 o. C n Ht 157. 5 cms Wt 65 kg BMI 26. 2 n Conscious, coherent, oriented n Warm, moist skin, (-) hirsutism, (-) hyperpigmentation n
PHYSICAL EXAMINATION n n (+) facial & back acne (+) cushingoid facies (+) 4 x 4 cm hard, nontender, fixed mass R maxillary area topped with small vascularities (+) 8 x 10 cm hard, nodular, non-tender, movable mass on L submandibular area
PHYSICAL EXAMINATION n n (+) facial & back acne (+) cushingoid facies (+) 4 x 4 cm hard, nontender, fixed mass R maxillary area topped with small vascularities (+) 8 x 10 cm hard, nodular, non-tender, movable mass on L submandibular area
PHYSICAL EXAMINATION n (+) buffalo hump
PHYSICAL EXAMINATION n n n Pink palpebral conjunctivae, anicteric sclerae Moist buccal mucosa, nonhyperemic posterior pharyngeal wall, tonsils not enlarged Symmetrical chest expansion, clear breath sounds Adynamic precordium, normal rate and regular rhythm, distinct S 1 and S 2, no murmurs Globular abdomen, (+) truncal obesity, (-) striae, NABS, soft, nontender
PHYSICAL EXAMINATION n n n (+) grade 2 bilateral pitting edema, (-) atrophy of extremities Pulses full and equal Neuro Exam: - Awake, alert, oriented to 3 spheres - Cranial nerves intact - MMT: 5/5 BUE, 1 -2/5 BLE - Sensory: 35% sensory deficit RLE 25% sensory deficit LLE
ADMITTING IMPRESSION Seizure disorder probably 2 o to brain metastasis Esthesioneuroblastoma, metastatic to neck, R maxilla and brain
COURSE IN THE WARD n ADMISSION: - 12 -lead ECG, CXR - 2 D-echo with doppler - CBC, Stat 5, BUN, Creatinine, Mg, ABGs - Urinalysis - Neuro referral: MRI/MRA of brain with gadolinium, EEG
RESULTS ABGs CBC Hgb Hct WBC Seg Lym Eos Mono Plt ct 13. 2 41 16. 06 85 9 2 4 235, 000 p. O 2 76. 8 p. H 7. 55 p. CO 2 49. 8 HCO 3 43. 2 O 2 sat 96. 6 B. E. +18. 1 TCO 2 44. 7
RESULTS 9/20 9/22 Na 137 143 K 1. 9 2. 0 2. 8 BUN 18 16. 01 Crea 0. 8 0. 6 Glucose Mg 122. 08 105. 93 (R) (F) 2. 2 9/23 9/26 9/27 9/30 2. 9 3. 0 143 3. 2 2. 9 1. 0
RESULTS n EEG This is an EEG recording of a 42 y/o female with seizure and frontal mass. Background activity consists of fairly organized fairly modulated medium voltage 8 -10 Hz alpha rhythm best seen posteriorly attenuating on eye opening. Intermittent 4 -6 Hz theta activity with sharp slow wave components are seen on either side. Photic stimulation did not elicit any further abnormality. Interpretation: Abnormal EEG recording because of intermittent theta slowing with sharp slow wave components seen on either side.
RESULTS n MRI/MRA of brain with gadolinium
COURSE IN THE WARD n ADMISSION: - Valproic acid 250 mg/tab 1 tab TID - Dexamethasone 5 mg/IV q 6 h - Nephrology referral - p. NSS 1 L + 30 m. Eq KCl x 80 m. L/hr - Kalium durule 3 durules q 3 h x 4 doses
COURSE IN THE WARD n 3 RD HD - Urine K - Serum K - Radio-Oncology referral - Endocrine referral Dexamethasone suppression test Plasma renin, aldosterone, cortisol levels
2002 2008
RESULTS (9/23/08) 9/20 9/22 Na 137 143 K 1. 9 2. 0 2. 8 BUN 18 16. 01 Crea 0. 8 0. 6 122. 08 (R) 105. 93 (F) Glucose Urine K: 30. 8 mmol/L 9/23 9/26 9/27 9/30 2. 9 3. 0 143 3. 2 2. 9 1. 0
RESULTS (9/24/08) Plasma aldosterone: 14. 49 ng/d. L n Plasma renin: 0. 259 ng/m. L/hr n ARR: 55. 9 n n Plasma cortisol: 3, 401. 146 nmol/L
COURSE IN THE WARD n 6 TH HD - Plasma ACTH - Adrenal CT scan imaging
COURSE IN THE WARD n 7 TH HD - MRI of pituitary
COURSE IN THE WARD n 8 TH HD - Radiotherapy started
COURSE IN THE WARD n 12 TH HD - Discharged - THM: Kalium durule 2 durules TID : Aldactone 50 mg/tab 1 tab OD - Continue RT as outpatient
RESULTS (9/30/08) n Plasma ACTH: 304. 12 pg/m. L
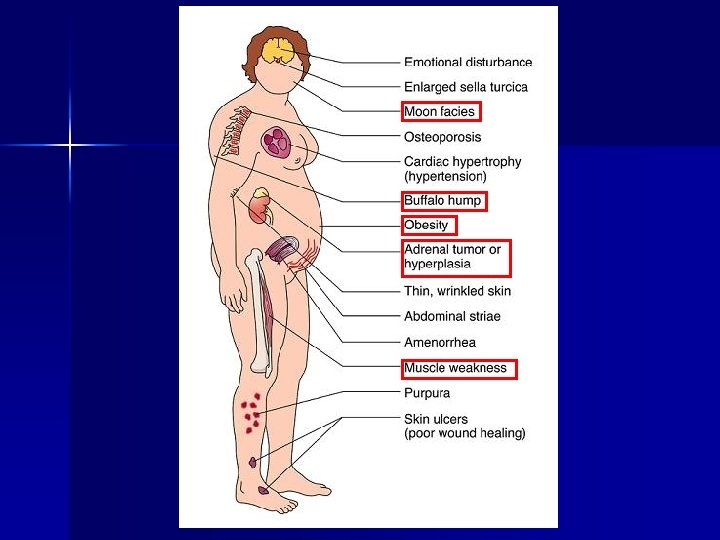
SALIENT FEATURES n HISTORY: - Esthesioneuroblastoma n CLINICAL SIGNS: - Moon facies - Buffalo hump - Facial and back acne - Truncal obesity - Bipedal edema - R Maxillary and L submandibular masses
SALIENT FEATURES n CLINICAL SYMPTOMS: - Weight gain - Polyuria, polydipsia, nocturia - Easy fatigability - Lower extremity weakness - Headaches and diplopia - Seizure
SALIENT FEATURES n DIAGNOSTICS: - Persistent hypokalemia - Metabolic alkalosis - Slightly elevated blood sugar levels - ↓ Renin - ↑ Cortisol - ↑ ACTH - MRI of brain: multiple necrotic midline lesions - Adrenal CT: Bilaterally enlarged adrenal glands - Pituitary MRI: “Empty sella”
FINAL DIAGNOSIS Generalized seizure 2 o to infiltrative brain metastasis Advanced esthesioneuroblastoma, metastatic to neck, R maxilla and brain Cushing’s syndrome 2 o to ectopic ACTH secretion probably 2 o to metastatic Esthesioneuroblastoma Hypokalemia 2 o to hypercortisolism 2 o to ectopic Cushing’s syndrome
DISCUSSION
ESTHESIONEUROBLASTOMA n n n n n Olfactory neuroblastoma 2 -3% of nasal tumors 1 -5% of malignant neurologic neoplasms Slow-growing Locally invasive Local recurrence: 68% All age groups M>F ACTH and ADH secretion reported
ESTHESIONEUROBLASTOMA n Common symptoms: - nasal obstruction - recurrent epistaxis - hyposmia - rhinorrhea - headaches - visual disturbances
ESTHESIONEUROBLASTOMA
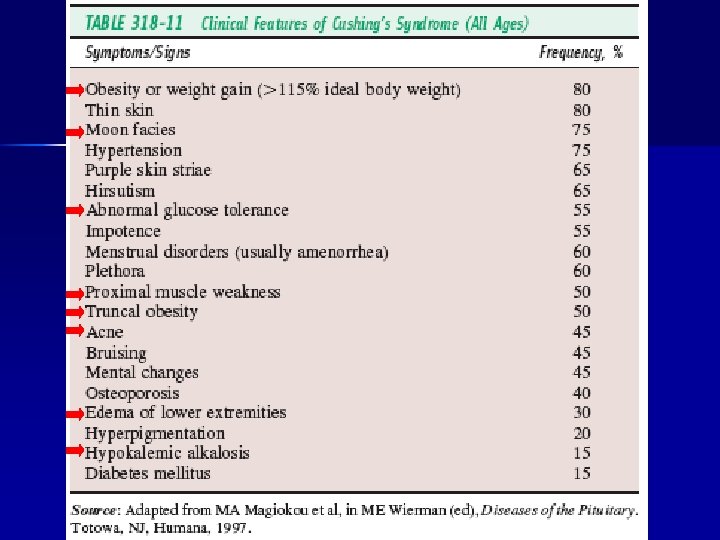
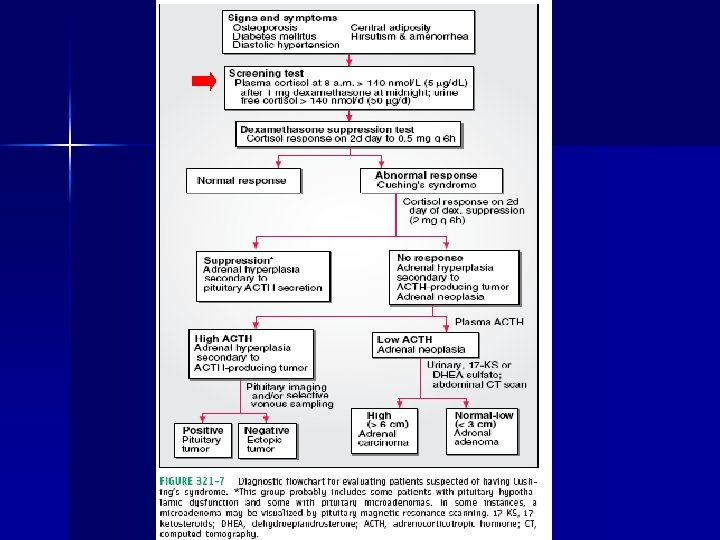
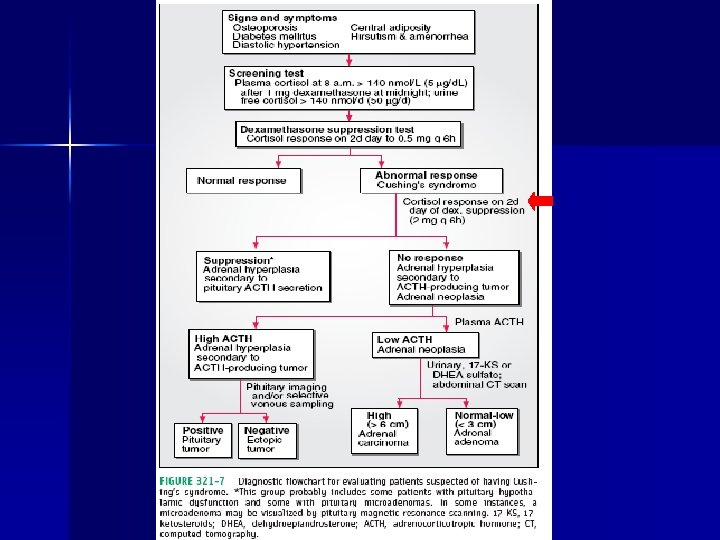
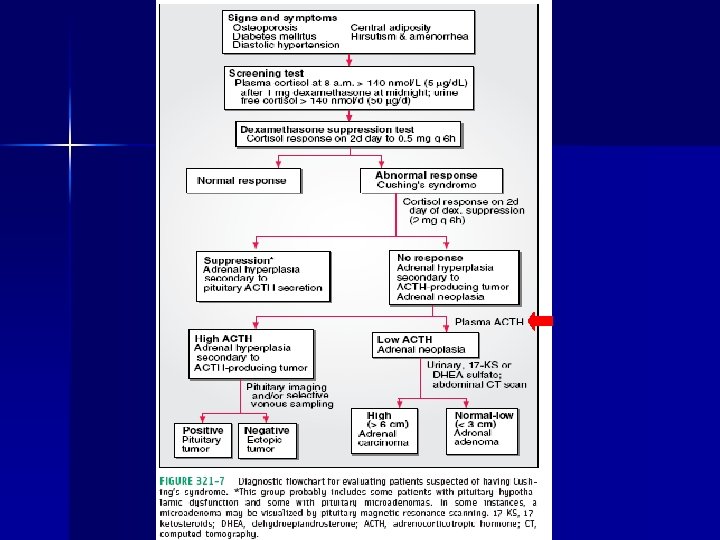
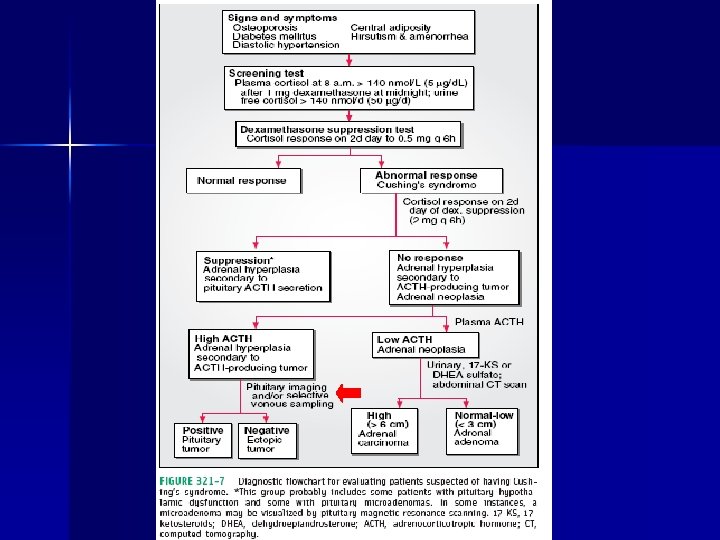
CUSHING’S SYNDROME n n n Excessive tissue exposure to cortisol Clinical features + biochemical abnormalities Exogenous vs endogenous 1. Exogenous glucocorticoids 2. Hypothalamic-pituitary disorders 3. Primary adrenal disorders 4. Ectopic secretion of ACTH
ECTOPIC ACTH SYNDROME n n n 10% of Cushing’s syndrome etiologies Majority have malignant tumors Localization is challenging Hypokalemic alkalosis is a prominent manifestation of the Ectopic ACTH Syndrome ACTH/cortisol – no circadian rhythm
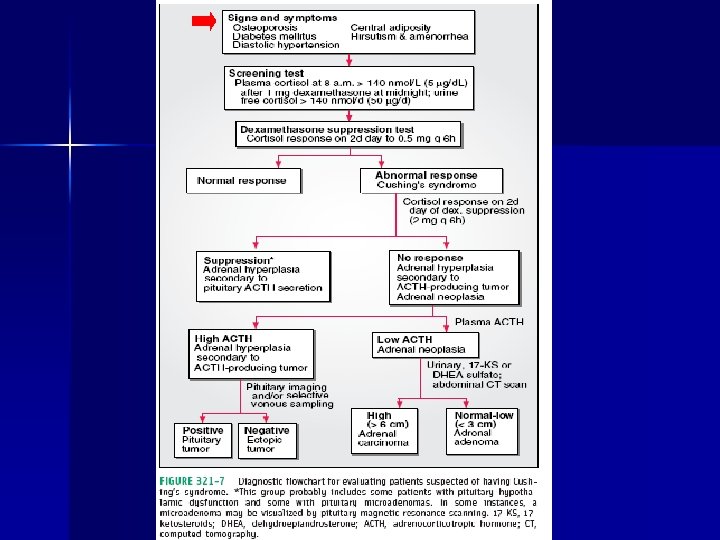
ECTOPIC ACTH SYNDROME n Diagnosis: (1) increased basal cortisol production (2) dependence of cortisol secretion on ACTH stimulation (3) resistance to glucocorticoid negative feedback (4) immunocytochemical techniques – Synaptophysin, S-100 protein, chromogranin A, tyrosinase, myc-2, EMA, cytokeratin
ECTOPIC ACTH SYNDROME n From esthesioneuroblastoma: 5 reported cases worldwide
TREATMENT n n Surgical resection Radiotherapy Medical: Chemotherapy : Ketoconazole, Metyrapone, Mitotane, Aminoglutethimide, Trilostane, Etomidate Adrenalectomy
THANK YOU!
RESULTS (9/20/08) n MRI/MRA OF BRAIN & INTRACRANIAL VESSELS 1. Anterior and posterior falcine tumors which appears to be separate from the nasal-anterior cranial fossa and left planum sphenoidale masses. Extension of the anterior falcine mass to the overlying right frontal bone is appreciated. 2. Incidental note of multiple cervical masses. 3. Metastatic disease from a known esthesioneuroblastoma vs multifocal neuroblastoma considered. 4. Normal MRA of the intracranial vessels
RESULTS (9/25/08) n CT SCAN OF UPPER ABDOMEN (PLAIN & IV CONTRAST) - Non-specific hypodense focus in hepatic segment IV. Correlation with biopsy and/or MRI with liver specific contrast (Primovist) is suggested for further evaluation. - Contracted gallbladder. - Bilaterally enlarged adrenal glands. - Consider hemorrhagic vs complicated cyst in the left kidney. - Consider dermoid cysts, probably ovarian, in the left hemiabdomen. - CT of the lower abdomen or UTZ is suggested for better pelvic evaluation.
RESULTS (9/27/08) n MRI OF THE SELLA TURCICA - Enlarged sella turcica with the infundibulum extending deep into the pituitary fossa (“Empty Sella”). No evidence of focal lesions nor abnormal enhancing masses in the pituitary fossa.