Liver Failure Mackay Memorial Hospital Department of Internal



, viruses Developing countries: viruses, regional Difference (endemic")
17, S 268–S 273")

, vascular abnormality, toxin, acute fatty")

 Respiratory failure Renal")

: mechanical ventilation. n Renal failure (hypovolemia, hepatorenal syndrome, ATN): hemodynamic monitor,")






 and brainstem Herniation the most common causes")



, corticosteroid")
: cardiovascular support n Malignant infiltration: liver biopsy for :")

 either PT>100 second or")
")


")

")
- Slides: 32
Liver Failure Mackay Memorial Hospital Department of Internal Medicine Division of Gastroenterology R 4 陳泓達 97/6/22
n Liver failure: Clinical syndrome: sudden loss of liver parenchymal and metabolic function Manifest as coagulopathy and encephalopathy
Acute liver failure : Defined as interval between onset of the illness and appearance of encephalopathy < 8 weeks n
Etiology: Western countries: heterogenous, drugs (acetaminophen, NSAID), viruses Developing countries: viruses, regional Difference (endemic area ? ) n
Journal of Gastroenterology and Hepatology(2002)17, S 268–S 273
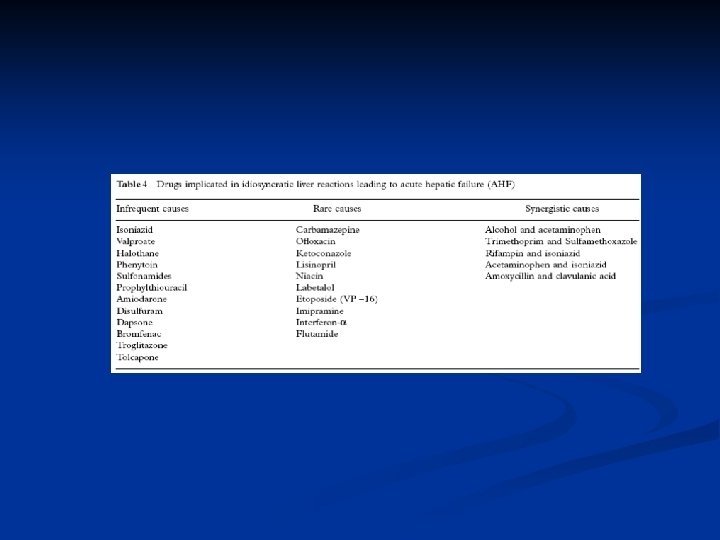
Acetaminophen toxicity Idiosyncratic drug toxicity Hepatotropic viruses Miscellaneous causes Indeterminate acute liver failure (viruses can not be demonstrated ? )
Uncommon causes: Wilson’s disease, other infections (CMV, HSV, EBV), vascular abnormality, toxin, acute fatty liver of pregnancy, antoimmune hepatitis, ischemia, malignant infiltration n
Symptoms and signs: Jaundice, altered mental status, nausea/ vomiting, anorexia, fatigue, malaise, myalgia/arthralgia Most of them present hepatoencephalopathy and icteric appearance. n
Non-specific Management Hypoglycemia Encephalopathy Infections Hemorrhage Coagulopathy Hypotension(hypovolemia, vascular resistance ↓) Respiratory failure Renal failure Pancreatitis
Hypoglycemia: monitoring blood glucose, IV glucose supplement. n Infection: aseptic care, high index of suspicion, preemptive antibiotic. n Hemorrhage (i. e. GI): NG placement, H 2 blocker or PPI. n Hypotension: hemodynamic monitoring or central pressures, volume repletion n
Respiratory failure (ARDS): mechanical ventilation. n Renal failure (hypovolemia, hepatorenal syndrome, ATN): hemodynamic monitor, central pressure, volume repletion, avoid nephrotoxic agent n
Encephalopathy major complication n precise mechanism remains unclear n Hypothesis: Ammonia production n Treatment toward reducing ammonia production n Watch out airway, prevent aspiration n
Encephalopathy Stage 1: day-night reversal, mild confusion, somnolence n Stage 2: confusion, drowsiness n Stage 3: stupor n Stage 4: coma n
Encephalopathy Predisposing factor of hepatic encephalopathy: GI bleeding, increased protein intake, hypokalemic alkalosis, hyponatremia, infection, constipation, hypoxia, infection, sedatives and tranquilizers
Encephalopathy TX upon ammonia hypothesis n Correction of hypokalemia n Reduction in ammoniagenic substrates: cleansing enemas and dietary protein restriction. n Lactulose: improved encephalopathy, but not improved outcome. Dose 2 -3 soft stools per day
Encephalopathy Oral antibiotics: neomycin lack of evidence nephrotoxicity limited use. n
Cerebral Edema Cerebral edema develops in 75 - 80 % of patients with grade IV encephalopathy. n precise mechanism : not completely understood n Possible contributing factor: osmotic derangement in astrocytes changes in cellular metabolism alterations in cerebral blood flow n
Cerebral Edema Clinical manifestations: ↑intracranial pressure (ICP) and brainstem Herniation the most common causes of death in fulminant hepatic failure ischemic and hypoxic injury to the brain hypertension, bradycardia, and irregular respirations, ↑ muscle tone, hyperreflexia n
Cerebral Edema Monitoring of ICP: routinely used by more than one-half of liver transplantation programs in the United States n Tx: to maintain ICP below 20 mm. Hg and the CPP above 50 mm. Hg. n
Coagulopathy diminished capacity of the failing liver to synthesize coagulation factors. n The most common bleeding site: GI tract. n Prophylactic administration of FFP: not recommended. performed before transplant or invasive procedure n
Specific Treatment ACT intoxication: charcol followed by NAC n Drug induced hepatotoxicity: discontinue drugs supportive treatment n Viral hepatitis: HBV: anti-HBV treatment, lamivudine HSV/varicella zoster: acyclovir : others: supportive care n
Wilson’s disease: early diagnosis liver transplant n autoimmune hepatitis: confirm diagnosis (liver biopsy), corticosteroid liver transplant n acute fatty liver of pregnancy or the HELLP syndrome: obstetrical services, and expeditious delivery are recommended n
Acute ischemic injury (shock liver): cardiovascular support n Malignant infiltration: liver biopsy for : diagnosis treat underlying disease. n Indeterminate etiology: consider biopsy for diagnosis and further guide of treatment n
Liver transplant: remain backbone of treatment of fulminant hepatic failure reliable criteria to identify these patients who really need transplant. remain unresolved in fulminant hepatic failure. n
At King’s College hospital in London (not due to ACT) either PT>100 second or the presence of any three of the following variables: 1. age < 10 or > 40 years ; 2. an etiology of non-A, non-B hepatitis, halothane, drug induced liver failure; 3. duration of jaundice before onset of encephalopathy > 7 days, prothrombin time >50 s, and serum bilirubin > 300 mmol/L.
Encephalopathy Coagulopathy (PT)
Liver transplant Criteria: In chronic liver disease most commonly used prognostic model MELD score (Model for End-stage Liver Disease ) 3. 8[Ln serum bilirubin (mg/d. L)] + 11. 2[Ln INR] + 9. 6[Ln serum creatinine (mg/d. L)] + 6. 4 Ln: natural logarithm. n
Liver transplant n 1. 2. 3. CONTRAINDICATIONS: Cardiopulmonary disease can not be corrected, or preclude surgery. Malignancy outside of the liver within 5 years of evaluation, or can not be cured. Active alcohol and drug use
n Advanced age and HIV disease: relative contra -indication (site-specific management)
Liver support system Non-cell-based: plasmapheresis and charcoalbased hemoabsorption n Cell-based systems : known as bioartificial liver support systems n
Liver support system Non-cell-based: not improved survival. Available systems: molecular adsorbents recirculation system (MARS) n Cell-based systems: undergoing trial. n