COMMON COMPLICATIONS OF LIVER DISORDERS Acute liver failure






























- Slides: 42
COMMON COMPLICATIONS OF LIVER DISORDERS • • • Acute liver failure Portal hypertension Ascites Hepatic encephalopathy Jaundice Hepatorenal syndrome Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 1
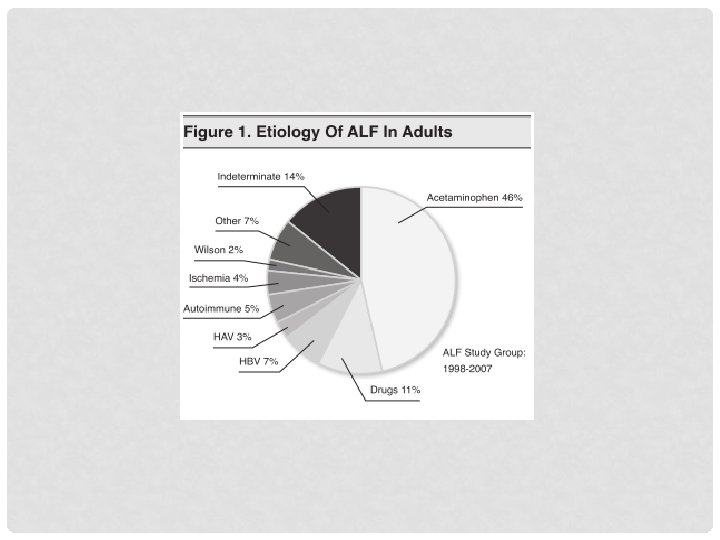
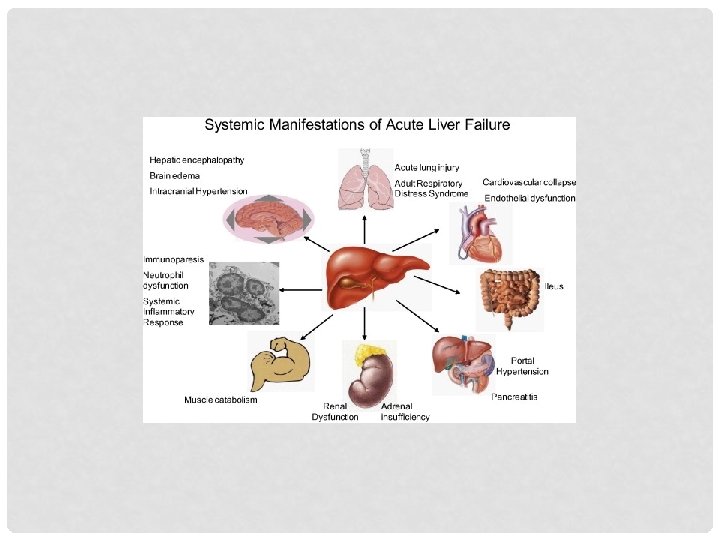
ACUTE LIVER FAILURE • Severe impairment or necrosis of liver cells without preexisting liver disease or cirrhosis • Leading cause: Acetaminophen overdose • Pathophysiology: • Hepatocytes become edematous. • Patchy areas of necrosis and inflammatory cell infiltrates disrupt the parenchyma. • Hepatic necrosis is irreversible. Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 2
ACUTE LIVER FAILURE • Clinical manifestations • Anorexia, vomiting, abdominal pain, and progressive jaundice • Treatment • • N-acetylcysteine: For acetaminophen poisoning Antiviral therapy: To improve survival in cases of viral hepatitis Lowering blood ammonia levels Liver transplantation Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 3
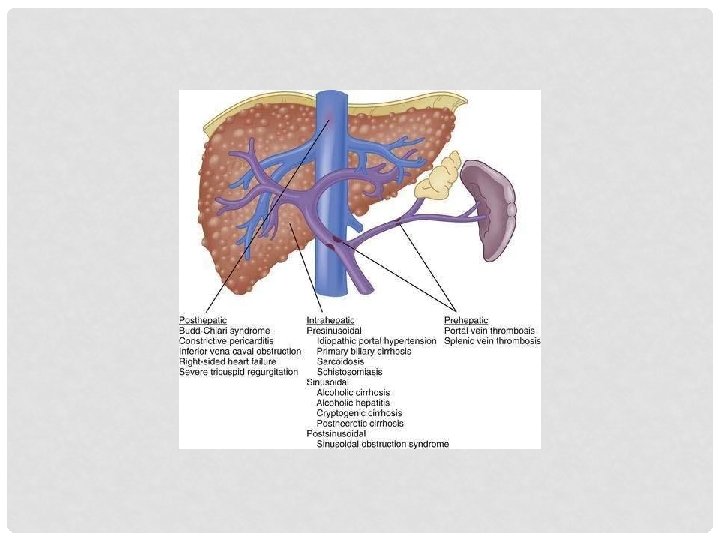
PORTAL HYPERTENSION • Abnormally high blood pressure in the portal venous system primarily caused by resistance to portal blood flow • Increase to at least 10 mm Hg (normal is 3 mm Hg) • Causes • Prehepatic • Intrahepatic • Posthepatic • Can cause fatal consequences Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 6
PORTAL HYPERTENSION • Consequences • Varices • Distended, tortuous, collateral veins • Lower esophagus, stomach, rectum • If rupture: Life threatening • Splenomegaly • Enlargement of the spleen • Thrombocytopenia: Increased risk for bleeding Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 8
PORTAL HYPERTENSION • Consequences • Hepatopulmonary syndrome • • Respiratory complications with pulmonary hypertension Intrapulmonary vasodilation Intrapulmonary shunting and hypoxia Portopulmonary hypertension (pulmonary vasoconstriction and vascular remodeling) Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 9
PORTAL HYPERTENSION • Clinical manifestations • Vomiting blood; ascites • Treatment • No definite treatment • Beta-blockers: To prevent variceal bleeding • Bleeding varices • Fluid resuscitation • Administration of prophylactic antibiotics, vasoactive drugs (nonselective β-receptor antagonists and terlipressin) • Endoscopic variceal band ligation, compression of the varices with an inflatable tube or balloon, and injection of a sclerosing agent Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 10
PORTAL HYPERTENSION • Varices Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 11
ASCITES Peripheral Arterial Vasodilation Theory or Forward Theory Overflow Theory Underfill Theory Renal sodium retention is stimulated by portal hypertension Hepatic sinusoidal hydrostatic Is the synthesis of the pressure increases, and overflow and underfill theories plasma oncotic pressure decreases Causes intravascular hypervolemia, which overflows or “weeps” into the peritoneal cavity Causes weeping of the lymph fluid from the surface of the liver Is the most accepted theory Portal hypertension and splanchnic vasodilation occurs Causes fluid transudation and lymph formation, producing ascites Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 13
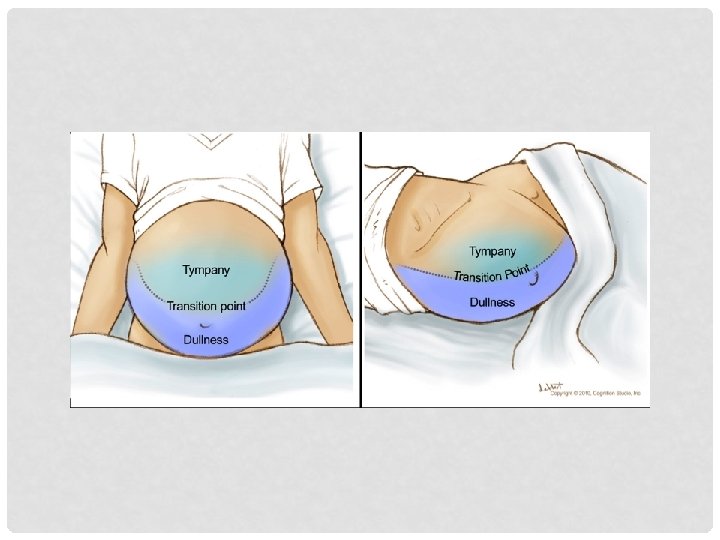
ASCITES • Accumulation of fluid in the peritoneal cavity • Most common cause: Cirrhosis • Clinical manifestations • Abdominal distention, increased abdominal girth, and weight gain • Evaluation • Serum-ascites albumin gradient (SAAG): Most specific diagnostic indicator Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 14
ASCITES • Mechanisms Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 15
ASCITES • Treatment • • • Dietary salt restriction Potassium-sparing diuretics Strong diuretics, such as furosemide or ethacrynic acid Vasopressin receptor 2 antagonists: For dilutional hyponatremia Possible administration of albumin Monitor serum electrolytes, especially sodium and potassium Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 17
ASCITES • Treatment • Paracentesis: Removal of 1 or 2 L of ascitic fluid and relief of respiratory distress • Removing too much fluid too fast relieves pressure on the blood vessels, causing arteriolar vasodilation and carries the risk of hypotension, shock, or death. • Ascitic fluid reaccumulates in individuals with irreversible disease. • Is likely to cause peritonitis. • Transjugular intrahepatic portosystemic shunt or peritoneovenous shunt: For refractory ascites • Liver transplant: Best treatment option Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 18
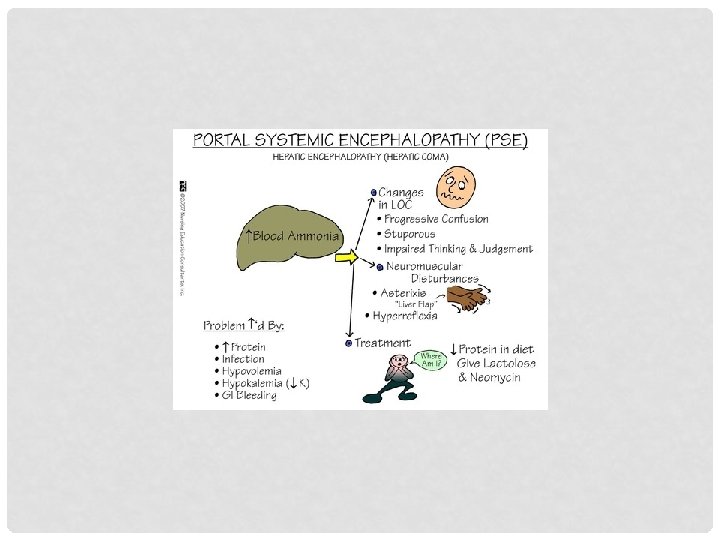
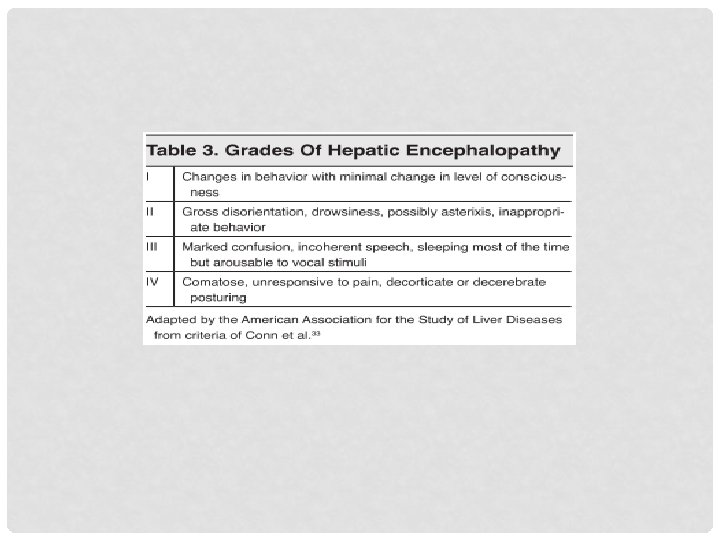
HEPATIC ENCEPHALOPATHY • Accumulation of toxins related to liver failure, causing a disruption of neurotransmission • Ammonia toxic to the brain • Clinical manifestations • • • Personality changes Confusion Memory loss Flapping tremor (asterixis) Stupor, coma, death Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 19
HEPATIC ENCEPHALOPATHY • Treatment • • Correct fluid and electrolyte imbalances Withdraw depressant drugs metabolized by the liver Restrict dietary protein intake Eliminate intestinal bacteria • • Neomycin Lactulose Rifaximin Sodium benzoate and L-ornithine-L-aspartate Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 22
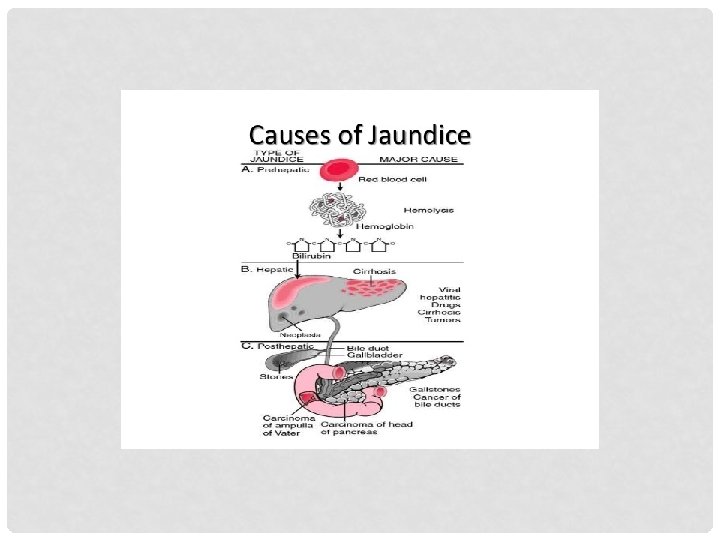
JAUNDICE • Called icterus • Yellow or greenish pigmentation of the skin caused by hyperbilirubinemia (total plasma bilirubin concentrations >2. 5 to 3 mg/dl) • Causes • Extrahepatic obstruction to bile flow (gallstones) • Intrahepatic obstruction (hepatocellular disease such as cirrhosis or hepatitis) • Prehepatic obstruction: Excessive production of bilirubin (excessive hemolysis of red blood cells) Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 23
JAUNDICE • Clinical manifestations • Dark urine • Clay-colored stools • Yellow discoloration possibly occurring first in the sclera of the eye and then progressing to the skin • Skin xanthomas (cholesterol deposits) and pruritus • Treatment • Correct the cause: Jaundice is only a sign of an underlying disorder. Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 25
JAUNDICE • Pathophysiology Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 27
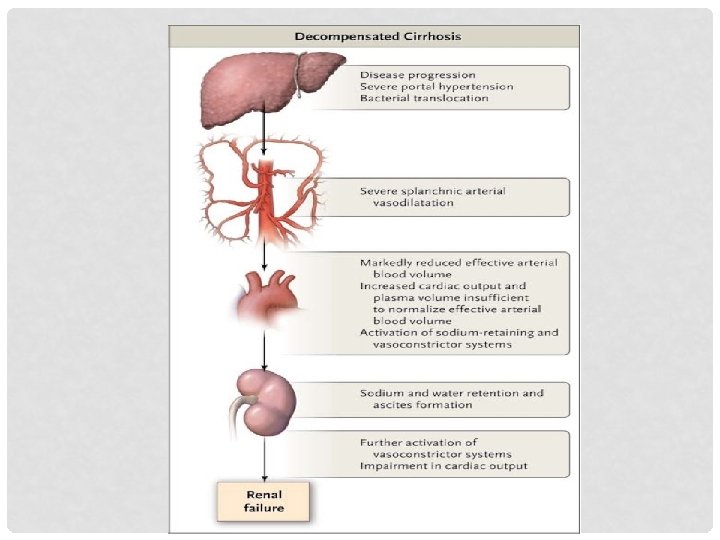
HEPATORENAL SYNDROME • Renal failure demonstrating oliguria, hypotension, and peripheral vasodilation as a result of advanced liver disease • Usually associated with alcoholic cirrhosis • Treatment • Manage fluid and electrolyte disorders, bleeding, infections, and encephalopathy • Administer systemic vasoconstrictors (α-adrenergic agonists and terlipressin) and albumin • Liver transplantation Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 28
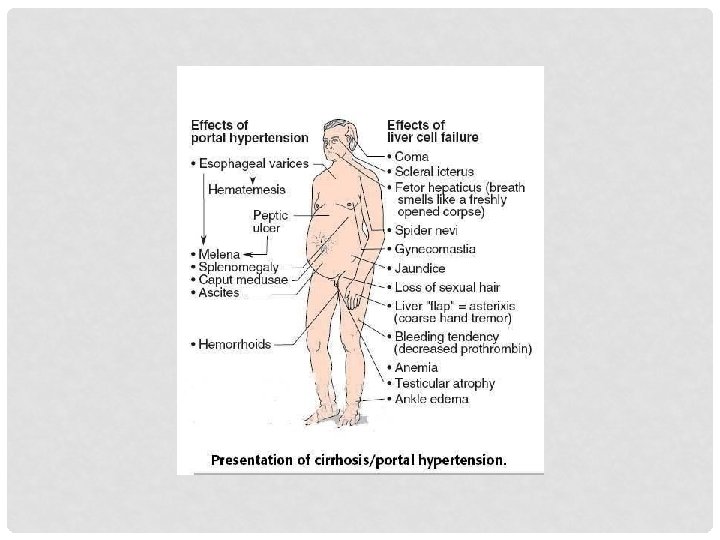
CIRRHOSIS • Is an irreversible inflammatory fibrotic disease that disrupts liver function and even liver structure. • Most common causes are alcohol abuse and viral hepatitis. • Hepatic function from nodular and fibrotic tissue synthesis (fibrosis) decreases. • Biliary channels become obstructed and cause portal hypertension. • Because of the hypertension, blood is shunted away from the liver, and hypoxic necrosis develops. Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 30
CIRRHOSIS • Alcoholic liver disease • Oxidation of alcohol, causing damage to hepatocytes • Steatosis (alcoholic fatty liver) • Is the mildest form. • Is reversible if drinking is stopped. • Alcoholic hepatitis (steatohepatitis) • Is characterized by inflammation. • Degeneration and necrosis of the hepatocytes occur. • Alcoholic cirrhosis (fibrosis) • Toxic effects of alcohol metabolism on the liver, immunologic alterations, oxidative stress from lipid peroxidation, and malnutrition occur. Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 31
CIRRHOSIS • Alcoholic liver disease • Impairs the hepatocytes’ ability to oxidize fatty acids, synthesize enzymes and proteins, degrade hormones, and clear portal blood of ammonia and toxins • Clinical manifestations • Nausea, anorexia, fever, abdominal pain, and jaundice • Treatment • • Cessation of alcohol Rest, a nutritious diet Corticosteroids, antioxidants, drugs that slow fibrosis Management of complications: Ascites, gastrointestinal bleeding, infection, and encephalopathy Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 32
CIRRHOSIS • Clinical manifestations Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 33
CIRRHOSIS • Nonalcoholic fatty liver disease • Is the infiltration of hepatocytes with fat that occurs in the absence of alcohol intake. • Is associated with obesity. • Biliary (bile canaliculi) • Cirrhosis begins in bile canaliculi and ducts. • Primary biliary cirrhosis (autoimmune) • T lymphocyte–mediated antibody-mediated destruction of the small intrahepatic bile ducts • Secondary biliary cirrhosis • Obstruction of common bile duct Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 34
CIRRHOSIS • Primary sclerosing cholangitis • Chronic inflammatory fibrotic disease of the medium- and largesized bile ducts outside of the liver Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 35
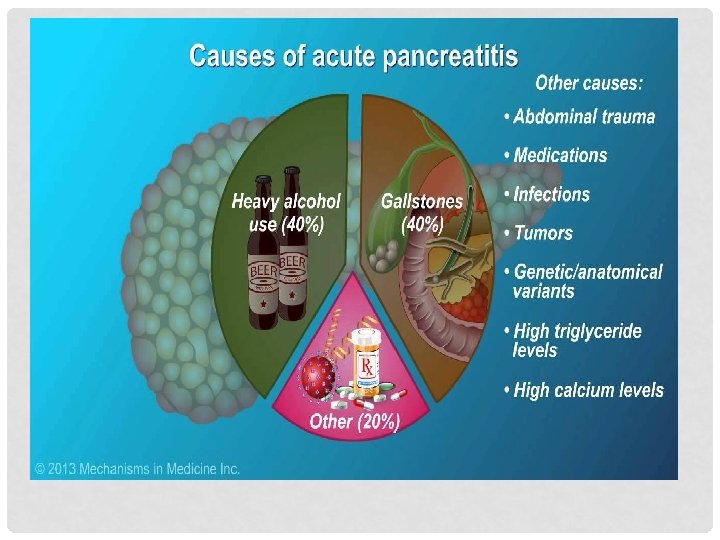
DISORDERS OF THE PANCREAS • Pancreatitis • Inflammation of the pancreas • Associated with several clinical disorders (alcohol intake and cholelithiasis) • Is caused by injury or damage to pancreatic cells and ducts, causing a leakage of pancreatic enzymes into the pancreatic tissue. • These enzymes cause autodigestion of pancreatic tissue and leak into the bloodstream to cause injury to blood vessels and other organs. • Acute versus chronic Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 36
ACUTE PANCREATITIS • Resolves spontaneously • Clinical manifestations • Epigastric or midabdominal pain; nausea and vomiting • Fever and leukocytosis • Evaluation • Elevated serum lipase: Primary diagnostic marker • Treatment • Narcotic pain medication • Nasogastric suctioning • IV fluids Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 38
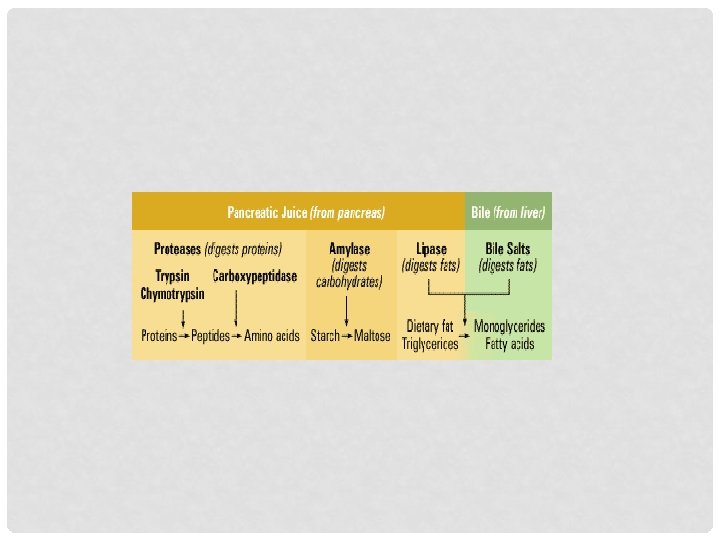
ACUTE PANCREATITIS • Pathophysiology Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 39
CHRONIC PANCREATITIS • Repeated exacerbations of acute pancreatitis can lead to chronic changes. • Destroys acinar cells and the islets of Langerhans. • Pancreatic parenchyma is destroyed and replaced by fibrous tissues, strictures, calcification, ductal obstruction, and pancreatic cysts. • Chronic alcohol abuse: Is the most common cause. • Is a risk factor for pancreatic cancer. Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 41
CHRONIC PANCREATITIS • Clinical manifestations • Continuous or intermittent abdominal pain • Treatment • Corticosteroidal agents: For autoimmune pancreatitis • Cessation of alcohol use and smoking • Analgesics, endoscopic therapy, and surgical drainage of cysts or partial resection of the pancreas Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 42