Hypothalamusespituitary axis Hypothalamose n pituitary stalk n ADH

 Cell bodies in SON (ADH) & PVN • (Oxytocin) of hypothalamus")








 RESPONSE")
 Other effects: thickening,")


 n Cortisol(not specific),")
 1 -Overnight DST(1 mg")



 Single assay? Renal failure? Monoclonal gammopathies Magnesium")

hypercalcemia Primary hyperparathyroidism Hypercalcemia of Malignancy Uncommon causes of hypercalcemia n n")
 n n n")
 n")


- Slides: 33
Hypothalamuses-pituitary axis Hypothalamose n -pituitary stalk n ADH, OX Pituitary hormones
Posterior Pituitary (neurohypophysis) Cell bodies in SON (ADH) & PVN • (Oxytocin) of hypothalamus Consists of neural endings with • associated blood vessels Acts as storage area, secretory • granules travel down axon Connects to hypothalamus via • hypothalamic-hypophyseal tract Processes extend through infundibulum • and end in Post. Pit
Primary positive signal Fig. 4 -10 A Page 117
Pituitary hormones hypothalamus-Pituitary axis Prolactin GH Prolaction Structure function .
Regulation of prolactin
Laboratory tests Variation secretion n TRH stimulate production n Normal level in women (up to 20 ng/ml/12 ng/ml n Prolactin Excess n In women: Milk production(galactorrhea), amenorrhes) In Men: Infertility, and impotence, Rarely breast enlargment(Gynecomastia) >200 ng/ml: Pituitary tumores 100 -200 ng/ml: tumors 20 -100: diurnal variation, medications, stress, …
Prolactin levels
Growth hormones Structure n Function n -Indirect -Direct
Regulation
Prolactin levels Marked diurnal Variation n
Laboratory data n n n GH Levels (single mea. Unless 1 h sleep) RESPONSE TO Physiologic and pharmacologic changes. S STIMULATORS: Exersise, Insulu Hypogly. GHRH(1 mg/kg, clonidine(4 mg/kg), ldopa(0. 5 g)argenine(0. 5 g/kg) IGF-I and binding proteins IGF-1 best marker), <5 year very low Inhibition: liver disease, acute illoness, malnutreitient
Laboratory evaluation n n GH over production Pituitary tumore (gigantism, acromegaly) Other effects: thickening, In. sweating, oilness of skin, hypertention, joint paint, hyperglecia GH deficiency
n n Sampling Transfering Blood increase Blood decrease
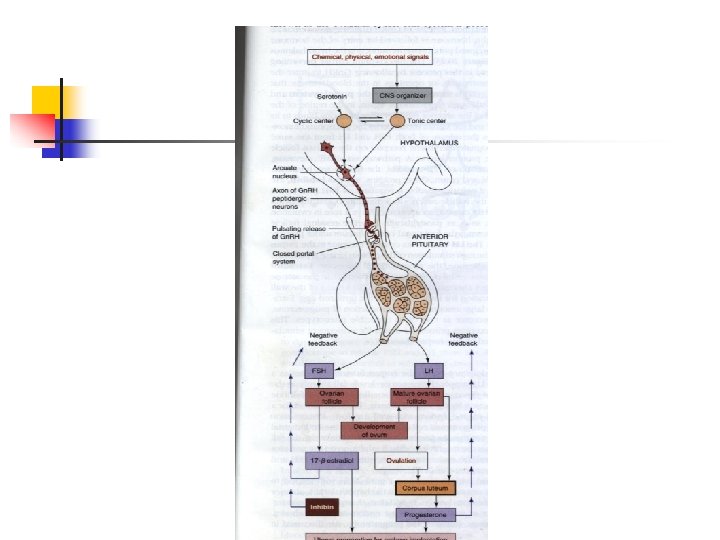
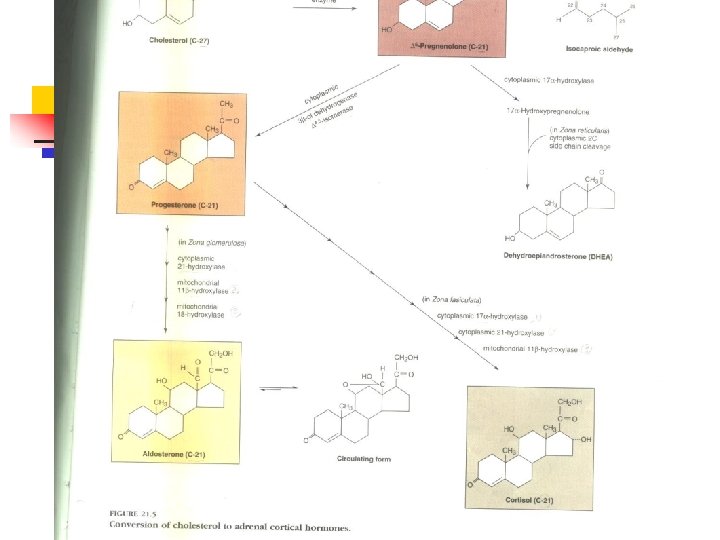
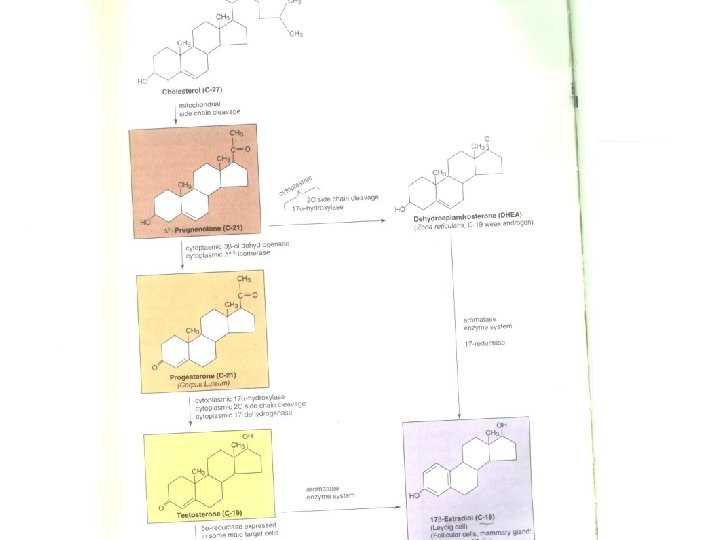
Evolution of Adrenal function Introduction Hypothalamic-pituitary-glucocorticosteroid Axis Biosynthesis Glococorticoids Mineral corticoids Sex Hormones Regulations n n n n
Direct tests of the hypothalamic – pituitary –adrenal Axis Cortisol, ACTH(stress) n Cortisol(not specific), n Synthetic stroids, CBG change. (↓Liver disease, malnutrition, ↑Est, pregnancy. ) Urine Free cortisol Plasma cortisol exceeds protein binding capacity, ref. (20 -90 µg/day) Corticosteroid intermediates Evaluation for suspected congenital adrenal hyperplasia or carcinoma(17 hydroxysteriods, ). Adrenal Androgen production DHEA_S (plasma, urine), Testesteron (gonads), Weak androgens(from gonads and adrenal(measured)
Dynamic tests of the hypothalamic-pituitary-adrenal Axis Dexamethasone suppression tests (DST) 1 -Overnight DST(1 mg Dexa. ). n 2 -Low dose. DST(0. 5 mg/6 h/2 d) n 3 -high dose(2 mg/6 h/2 d) n Stimulatory stimulation n n 1 - Cortrosyn stimulation(250 µg/0, 30, 60 min. after n injection), 7µg to 18 -20 µg, normal, 1µg physiological dose? 2 -Metyrapone Test(inhibites last step in cortisol synthesis) 3 -Insulin hypoglycemia(Insulin, 0. 05 -0. 1 u/kg) n 4 - corticotropin –releasing hor. stimulation n n
Abnormalities of Glu. production Suspected Cushing syndrome (excess Glu. Obesity, hypertention, virilization, hyperglycemia(hypokalemia and metabolic alkalosis may? ) Diagnosis of Cushing syndrome UFC or Overnight DS Adrenal insufficiency Mineral cor. (dehydration, hyponatremia, hyperkalemia, non-anion gap metyabolic acidosis. ) Glu. Deficeincy(weight loss, vometing, weakness) Primary insufficiency(addison disease). Pigmentation skin(POMC) Secondary adrenal insuficiency(pituitary). Neither min nor excess ACTH is present(Hyperglecimia) Diagnosing adrenal insufficiency Cortisol measument(18 -20µg ruling out) Trea. Administration dexametasine, cotrosyn) n
Congenital adrenal hyperplasia 21 -hydroylase deficiency 11 -hydroxylase deficiency n n
Laboratory tests of mineral and metabolism Plasma calcium Total and active form (PH, complexing anion) Adjusted Ca(mg/dl)=total. Ca(mg/d. L)+0. 8 x(4 Albumin(g/d. L) Free Calcium?
Phosphate Variation(Throuhgout the day and after meals↓) Single assay? Renal failure? Monoclonal gammopathies Magnesium Plasma equilibrates with cell magnesium n n n
PTH Mid-molecule or C-terminal assay measure long-lived, inactive metabolite Renal failure? PTH assay? Vitamin D assay 25 -Hydroxyvitamin D assay proportion to deficiency or toxicity 1, 25 Dihydroxyvitamin D(suspected ectopic) PTHr Urinary Mineral Excretion n n n n
Hypercalcemia Artifactual(protein bound)hypercalcemia Primary hyperparathyroidism Hypercalcemia of Malignancy Uncommon causes of hypercalcemia n n
Hypocalcemia Artfactual Chronic Renal failure Uncommon causes (hypo. PTH, Hypomagnesemia) n n n
Hyperphosphatemia Renal failure Uncommon causes(Hypo. PTH, Vitamin D Toxicity, hyperthyroidism, Cell lysis sydromes) n n
hypophosphatemia Osteoporosis Vitamin D defiemcy Paget, s disease Renal Osteodystrophy n n
Metabolic Bone disease