Pituitary Gland Two areas Anterior Pituitary Posterior Pituitary
















. 3. Action on milk")




















 cholecalciferol to 1 -25(OH)2 to")






- Slides: 54
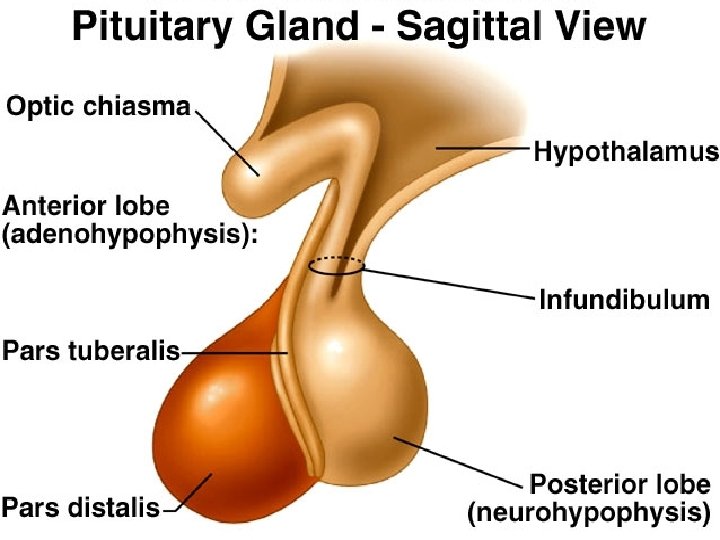
Pituitary Gland Ø Two areas ØAnterior Pituitary ØPosterior Pituitary Ø Structurally, functionally different
The pituitary gland HYPOTHALAMUS Hypothalamus secretes releasing factors ADH & oxytocin carried from hypothalamus INFUNDIBULUM Thyroid stimulating hormone Adrenocorticotropic hormone Gonadotropic hormones (FSH & LH) Growth hormone Prolactin Antidiuretic hormone ANTERIOR LOBE POSTERIOR LOBE Oxytocin
Anterior pituitary gland:
Cell types in anterior Pituitary Chromophilic cells Ø Somatotrophs- GH Ø Lactotrophs- Prolactin Ø Corticotrophs- ACTH Ø Thyrotrophs- TSH Ø Gonadotrophs- FSH, LH Chromophobic cells Folliculostellate cellsØ cytokines like IL 6
Growth hormone:
Actions of growth hormone:
Mechanism of action • Receptor on the membrane of the cell • Acts via JAK-STAT pathway
PHYSIOLOGICAL ACTION OF GH
Growth Hormone Direct effect Indirect effect Somatomedins Growth Bone, Cartilage
1. Action on growth: • Stimulates the growth of the skeleton. Specific action on the epiphyseal cartilage. Causes a linear growth of body. Increases growth of the skeletal frame by ü Proline collagen ü Incorporates sulfate into chondroitin. ü Increased deposition of protein by the chondrocytic and osteogenic cells that cause bone growth. ü Increased size and no of chondrocytes. ü Prechondrocytes ü Converting chondrocytes into osteogenic cells, thus causing deposition of new bone and increases osteoblastic activity.
• Stimulates the growth of the viscera. • Increases the skeletal muscle mass by increasing protein synthesis. • Pubertal and gonadal growth- promotes pre pubertal sexual maturation.
GH increase the length of the bones till fusion of epiphysis with the shaft Once the fusion occurs, GH looses the ability to increase the length of the bones. However, since the GH strongly stimulates osteoblasts, the bone continues to become thick throughout the life (jaw bone, skull bone)
2. Action on metabolism:
METABOLISM On. CARBOHYDRATE carbohydrate metabolism. Ø Decrease in the uptake of the glucose by the cells. Ø Decrease in the peripheral utilization of glucose for the production of the energy. Ø Facilitates hepatic neoglucogenesis. Ø Decreases insulin sensitivity. Ø Diabetogenic effect.
On fat metabolism: Lipid Metabolism Ø Is lipolytic – releases fatty acid from adipose tissue. Ø Increases fatty acids in the body fluids. Ø Enhances conversion of fatty acids to acetyl co-A and used as source of energy. Ø Can be Ketogenic in excessive amounts
On protein metabolism: Protein Metabolism Ø is a protein anabolic hormone. Ø Enhancement of amino acid transport through the cell membranes. Ø Enhancement of protein synthesis by ribosomes. Ø Increased transcription of DNA from RNA. Ø Decreased catabolism of protein and amino acid - “Protein sparer”
• On electrolytes: Conserves the electrolytes (Ca, Na, phospahte). 3. Action on milk production. Lactogenic and mammogenic activity. Help in the maintenance of milk secretion along with thyroxine and Prolactin. 4. Action on erythropoiesis: Increase erythropoietin production.
5. Action on lymphocytes: Stimulates the growth of the lymphoid tissue and proliferation of lymphocytes. 6. Action on gonads: Stimulates the growth of genitalia.
Biological Actions Of Human Growth Hormone Adipose Tissue Liver RNA synthesis Muscle Lipolysis Protein synthesis Glucose Uptake Somatomedin AA Uptake gluconeogenesis Protein Synthesis Somatomedins IGF- 1 and 2 Bone Chondrocytes
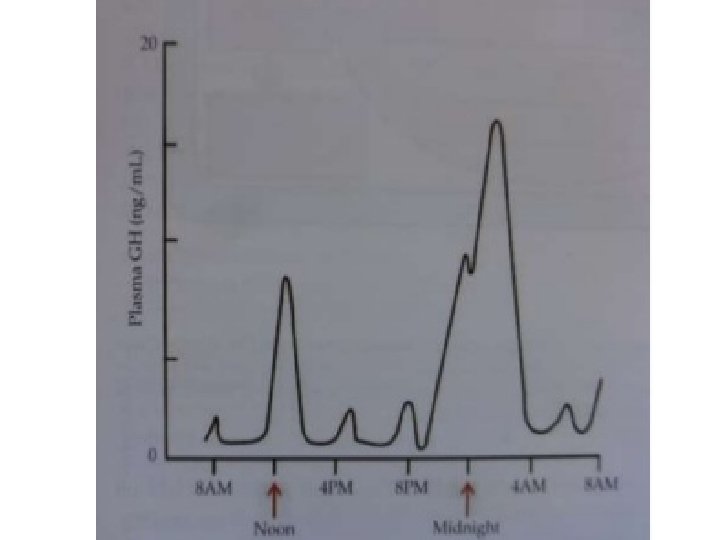
Factors influencing GH release • Stimulates ü Nor epinephrine ü Dopamine agonist ü Exercise ü Stress ü Hypoglycemia ü Starvation • Inhibits ü Dopamine blockers ü Obesity ü Hyperglycemia ü Chronic steroid treatment
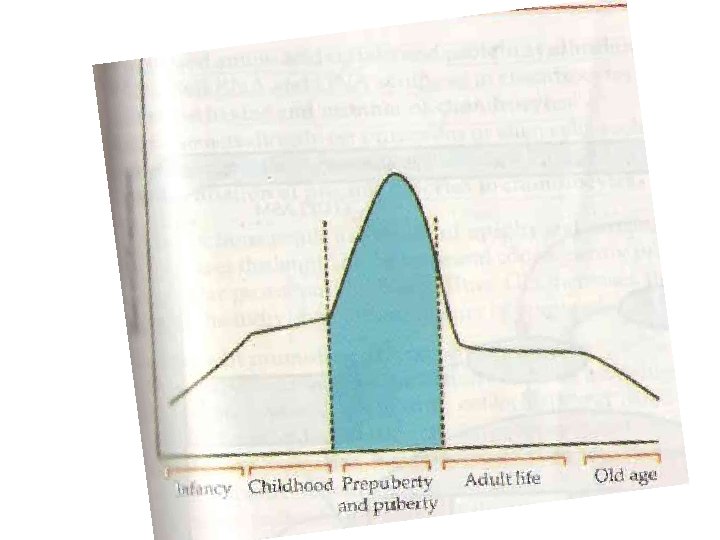
Regulation of Growth Hormone Body growth.
Applied aspects
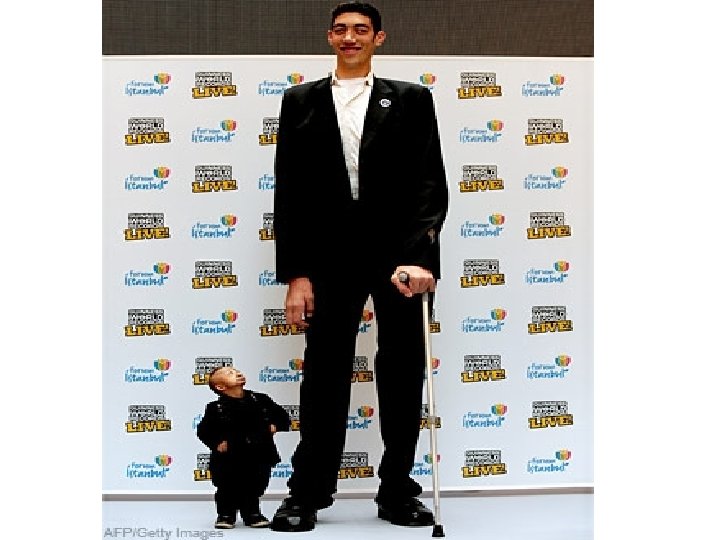
Abnormalities in GH Secretion 1. Hyposecretion: Dwarfism 2. Hypersecretion: Gigantism and Acromegaly
Hypersecretion of GH Leads to • Gigantism- In children • Acromegaly - In adults
Gigantism • • • occurs right from childhood. Before fusion of epiphysis. Abnormal height (7 feet and above. ) Forward bending of vertebral column ( Kyphosis ). High blood sugar( Diabetes mellitus) Limb-trunk proportion is abnormal.
22 yrs Twins
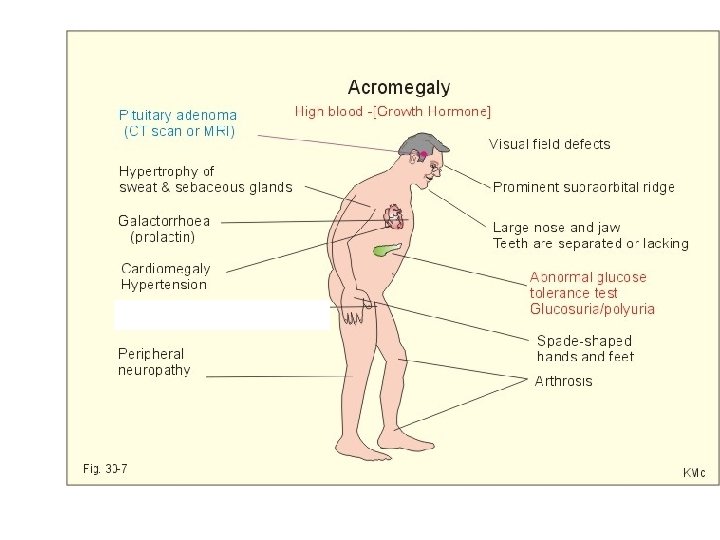
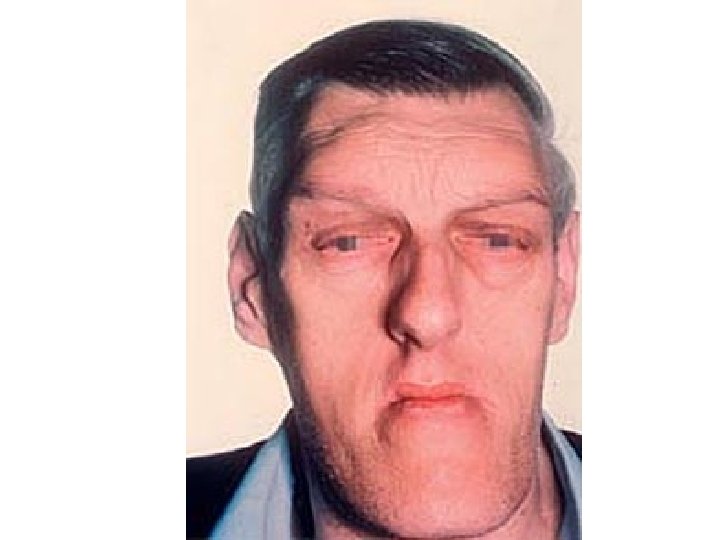
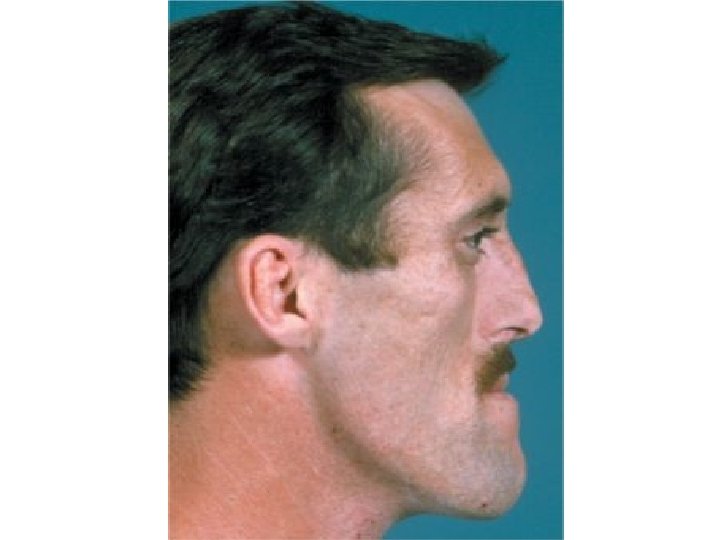
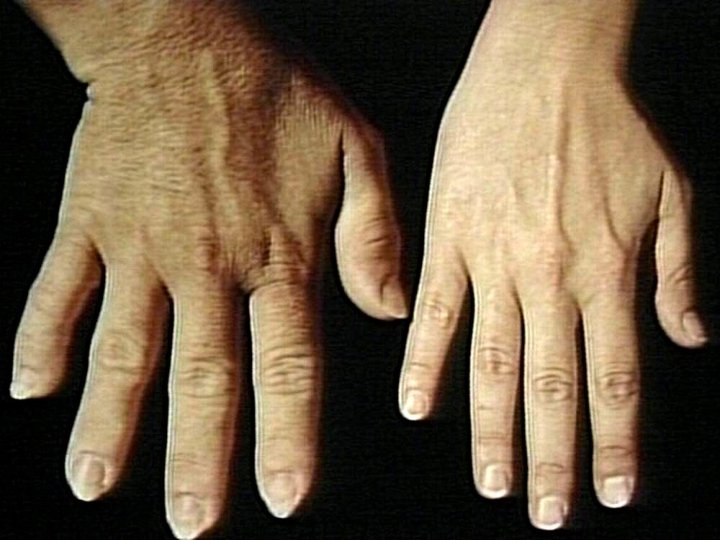
Ø Acromegaly Ø After fusion of epiphysis. Ø Enlargement of hands and feet. Ø Enlargement of membranous bones like cranium, nose, supraorbital ridges and lower jaw. Ø The lower jaw is protruded (Prognantism). Ø Bowing of spine (Kyphosis)
Ø Ø Over growth of malar, frontal and facial bones are thickened with thickening of skin and edema (Acromegalic or guerrilla face) Ø General overgrowth of body hair Ø Enlargement of visceral organs (lungs, thymus, heart, liver, spleen) Ø Bitemporal hemianopia Ø Hyperglycemia or glycosuria occur resulting in diabetes mellitus
• In the above photographs, we see a woman at 16, 33 and 52 years of age who has a condition caused by excessive secretion of growth hormone during adulthood. This condition is characterized by disproportionate growth in the jaw, hands and nose.
Dwarfism • • Disorder in children Characterized by stunned growth. No mental retardation. Sexual growth: Occurs normally in these individuals. Cause • Decrease GH secretion • Due to deficiency of secretion of GHRH • Atrophy of the acidophil cells
Panhypopituitarism Decreased secretion of all anterior pituitary hormones. The decrease in the secretion might be congenital or it may occur suddenly at any time during the life of the individual
Simmond’s disease • Occurs mostly in panhypopituitarism • Atrophy of anterior pitutiary gland
Laron dwarfism • The secretion of GH is normal or high • Unresponsiveness of GH receptors.
Action of prolactin:
1. Causes lactogenesis in the breast: • Initiates milk secretion and then maintains the same. • Stimulates the growth of alveoli and duct systems. 2. Suppresses menstrual cycle. 3. Stimulates erythropoiesis. 4. Maternal behavior.
5. Immunological function. 6. Increases the conversion of 25(OH) cholecalciferol to 1 -25(OH)2 to cholecalciferol. Increase in males-> impotency.
Regulation of prolactin secretion.
1. By hypothalamus. PRH, PIH. 2. Oestrogen and progesterone. High levels – Decrease the secretion. 3. Suckling of the breast and stimulation of vagina during coitus – Stimulates prolactin secretion. 4. Dopamine agonist- Decrease prolactin secretion.
Applied aspects
Hyper Prolactinemia: • In females: Galactorrhoea, Amenorrhoea and infertility. • In males : Sexual impotency
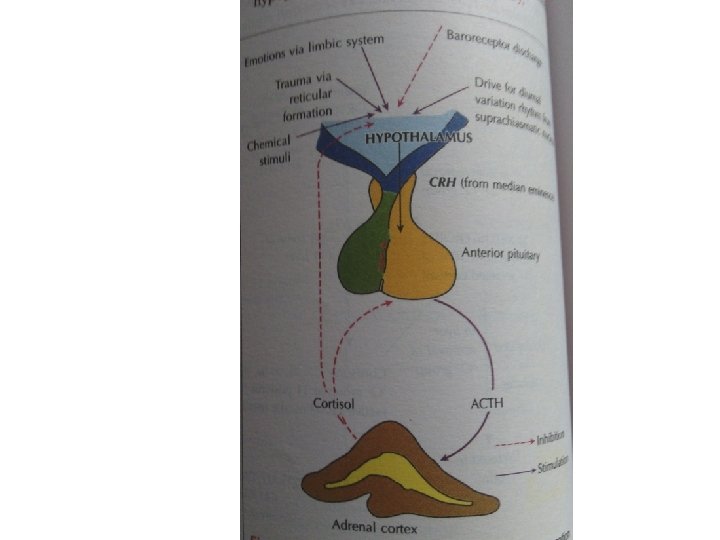
ADRENOCORTICOTROPIC HORMONE • Secreted from corticotrophs of anterior pitutiary • Proopiomelanocortin beta lipotropin • ACTH has intrinsic α- MSH activity.
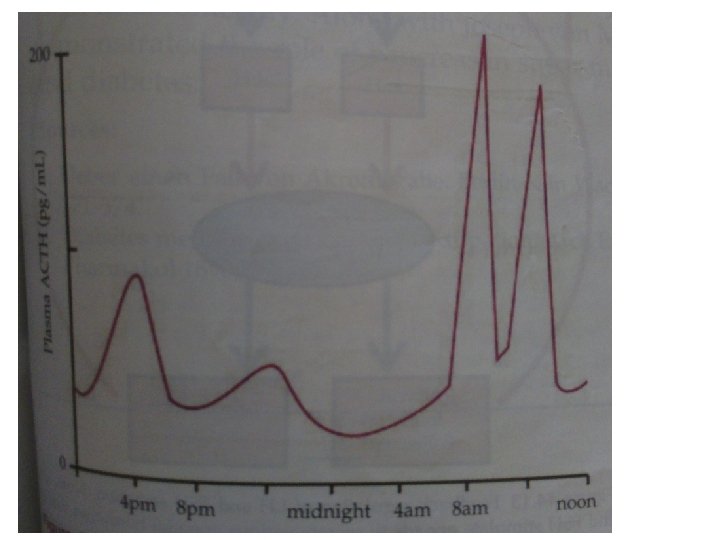
Factors influencing ACTH release • Stimulates ü CRH, ADH ü Stress ü Sleep wake cycle ü Anxiety, depression ü Seratonin ü Alpha receptor agonist, beta antagonist • Inhibits ü Cortisol ü ACTH ü Somatostatin ü GABA