Common Sports Injuries Nathan Melton D O Medical







 Ø Very common- 70% of college football players have experienced one")
 Ø Grade I- neuropraxia with demyelination of the myelin sheath no")
 Ø Grade II- axonotmesis disruption of the axon and myelin sheath")
 Ø Grade III- complete transection extremely rare l Surgery required for")
 Ø Treatment- thorough neuro exam consider AC separation, clavicle fracture, or")
 Ø if symptoms last for more than a few minutes- Xray")



 Ø 70%")











































 428 -0400 ask for Linda")
- Slides: 75
Common Sports Injuries
Nathan Melton D. O. Medical School Residency: Grandview Hospital Fellowship
Team Physician
Team Physician
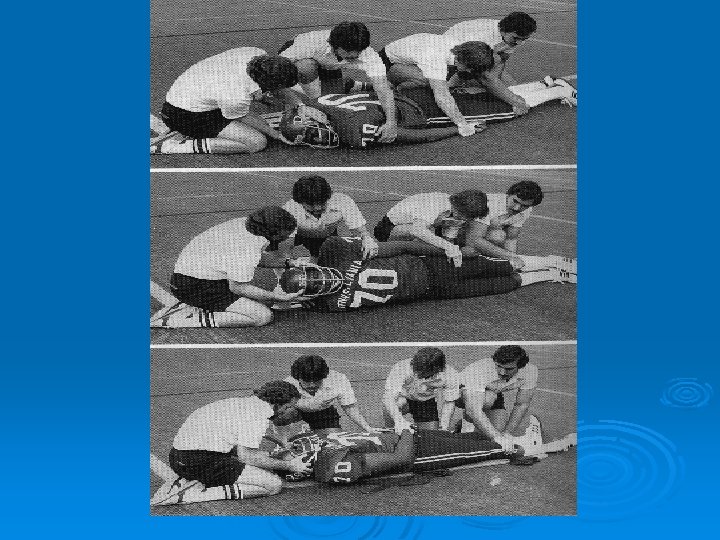
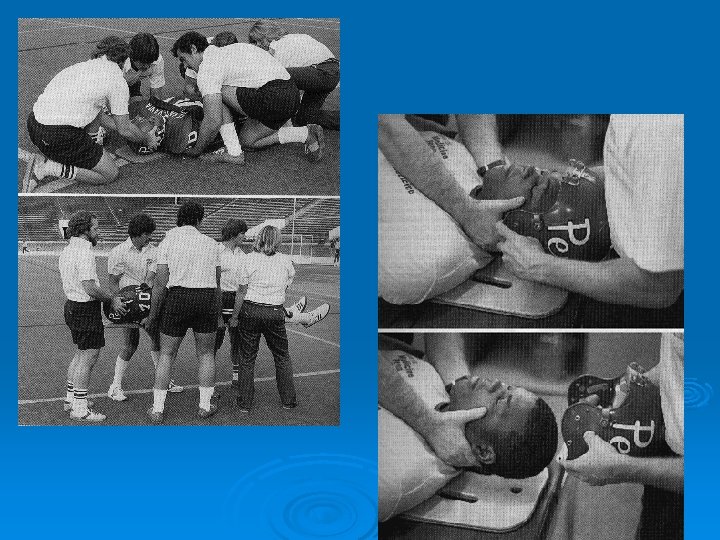
Cervical Spine Ø 11, 000 Catastrophic Cervical spine injuries per year Ø 7. 4 % are related to sports Ø Vast majority are football related
Cervical Spine ABC’s Ø Prevention of further injury Ø
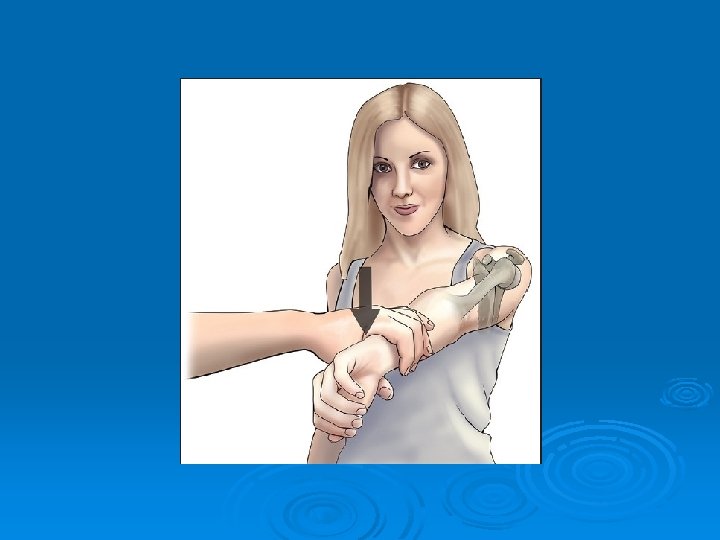
Burners
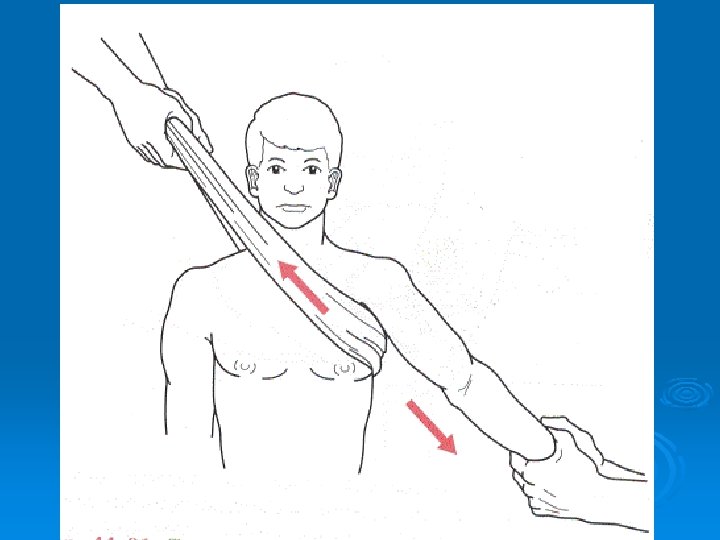
Burners (Brachial Plexopathies) Ø Very common- 70% of college football players have experienced one Ø Method of injury- Usually due to movement of the head away from the shoulder (Stretching of the Nerves) or direct trauma Ø Presentation- Usually unable to move the involved extremity (numbness & weakness)
Burners (Brachial Plexopathies) Ø Grade I- neuropraxia with demyelination of the myelin sheath no axonal disruption l Complete recovery in minutes to days l
Burners (Brachial Plexopathies) Ø Grade II- axonotmesis disruption of the axon and myelin sheath with preservation of the peri, endo, epineurium l Regrows at 1 -7 mm a day l Weakness lasts for weeks but full recovery can be expected. l
Burners (Brachial Plexopathies) Ø Grade III- complete transection extremely rare l Surgery required for any recovery l
Burners (Brachial Plexopathies) Ø Treatment- thorough neuro exam consider AC separation, clavicle fracture, or shoulder dislocation in your differential Ø if symptoms clear in minutes and no neck pain, limitation of neck movement, or shoulder pain- Patient can return. Ø Examine after the game
Burners (Brachial Plexopathies) Ø if symptoms last for more than a few minutes- Xray and MRI to rule out compressive pathology Ø Happens on more than 1 occasion they need to be removed and C Spine Xrays obtained
Things to look for Ø Cervical point tenderness Ø Neck stiffness Ø Bony deformity Ø Fear of head movement Ø Heavy head complaints Ø Bilateral symptoms Ø Treat like a spinal injury- Spine board and C-spine immobilization
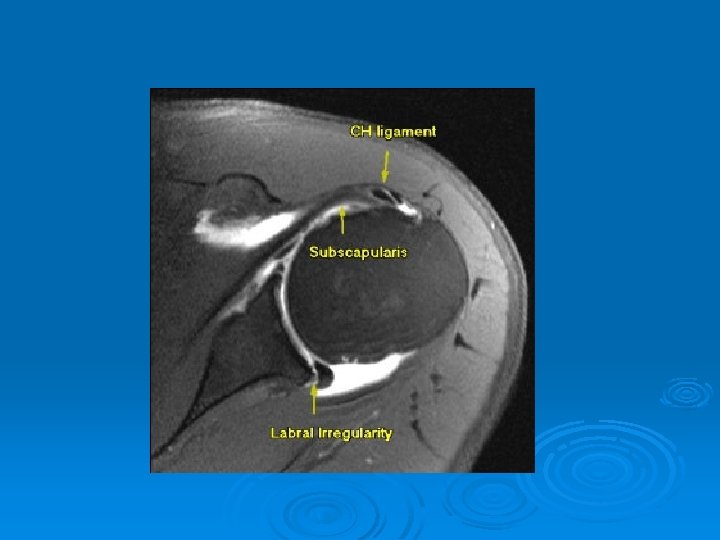
Shoulder Dislocation
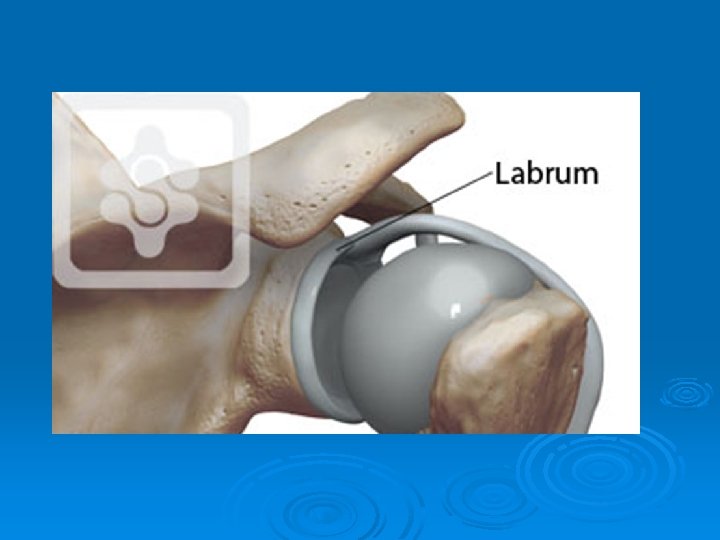
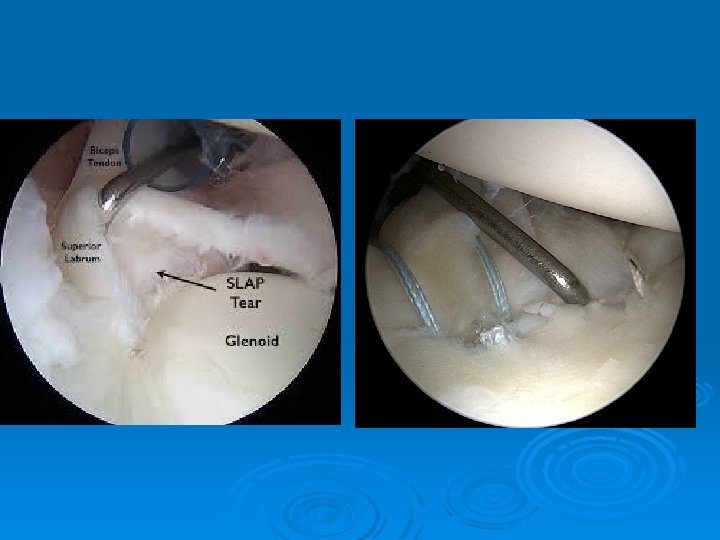
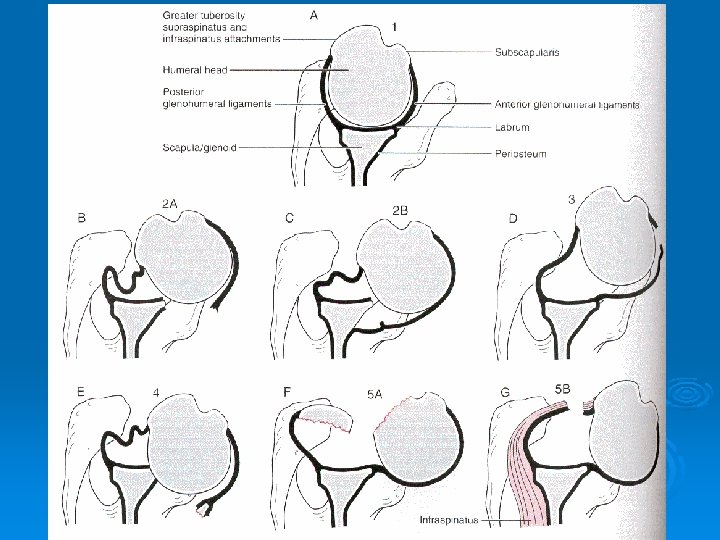
Dislocations Ø Most commonly traumatic and anterior Ø Postion of vulnerability (Abduction/ER) Ø 70% recurrence rate in patients under 22 Ø Independent of length of immobilization and physical therapy Ø Usually have a Bankart lesion (detached labrum) Ø Correlation between number of dislocations and soft tissue injury
Hippocrates Technique You’re gonna do what?
ZZZZZZZ Stimson Technique Most commonly used on the field technique Patience and Relaxation are key Typically takes 10 -15 minutes
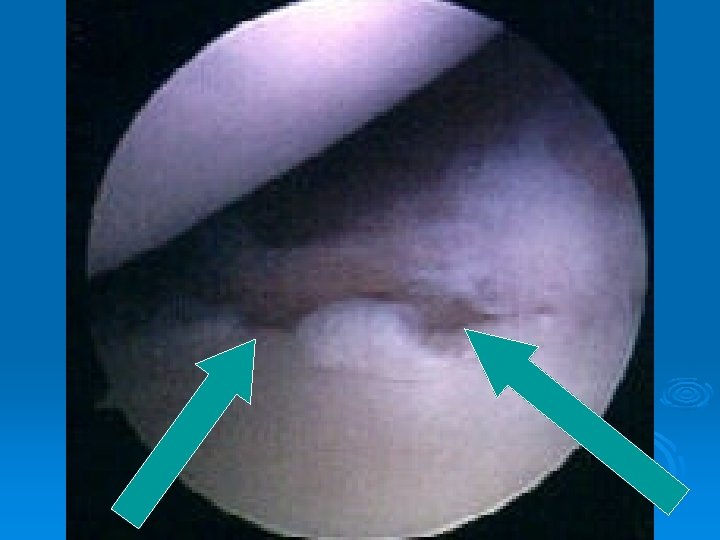
Bony Bankart
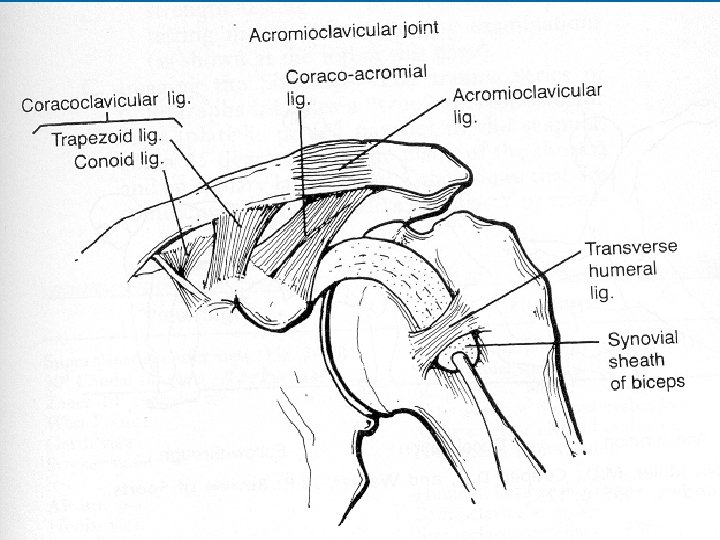
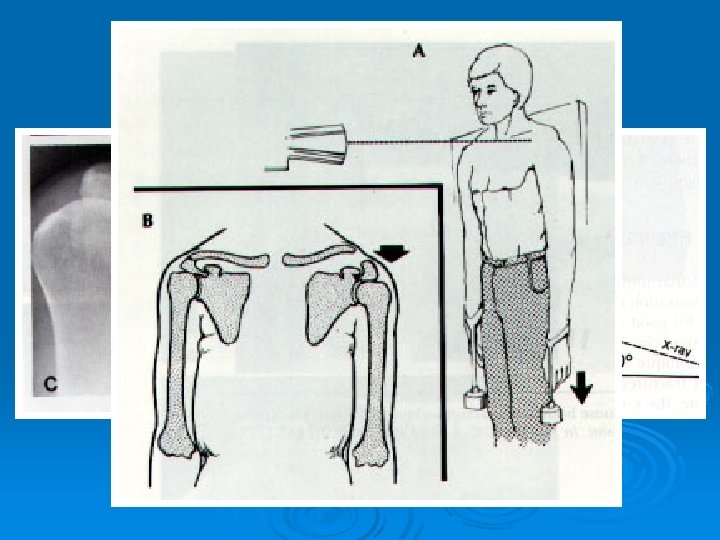
Acromioclaviclular Separation Ø Usually due to direct trauma- Superolateral aspect of the shoulder Ø Player striking the ground Ø the acromion is forced inferior relative to the clavicle
CLASSIFICATION Ø Type I AC ligament sprain l AC joint intact l CC ligament intact l Deltoid and Trapezius muscles intact l
CLASSIFICATION Ø Type II AC joint disrupted l CC ligament sprain l Deltoid and Trapezius intact l
CLASSIFICATION Ø Type III AC ligaments disrupted l AC joint dislocated l CC ligaments disrupted l Deltoid and Trapezius detached from distal clavicle l
CLASSIFICATION Ø Type IV AC/CC ligaments disrupted l Clavicle displaced posteriorly into or through Trapezius l
CLASSIFICATION Ø Type V AC/CC ligaments disrupted l Gross disparity btw clavicle and scapula l Deltoid and Trapezius detached from distal half of clavicle l
CLASSIFICATION Ø Type VI AC/CC ligaments disrupted l Clavicle displaced inferior to acromion or coracoid process l
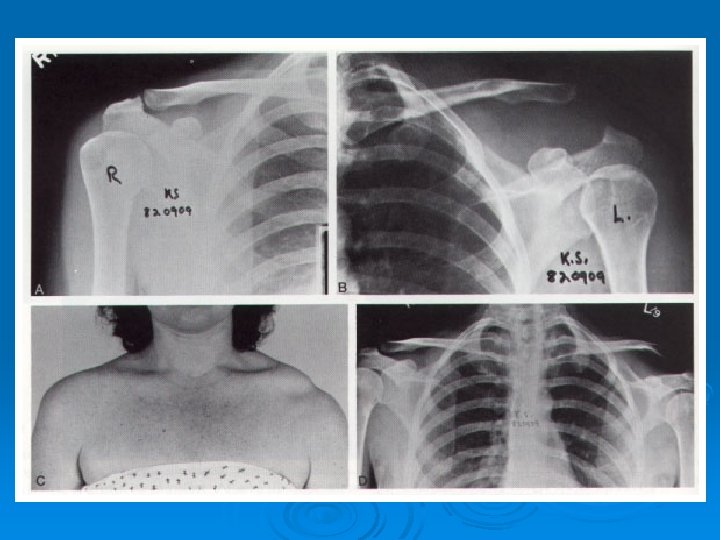
DIAGNOSIS Ø History Ø Mechanism of Injury Ø Physical Exam Ø Radiographs
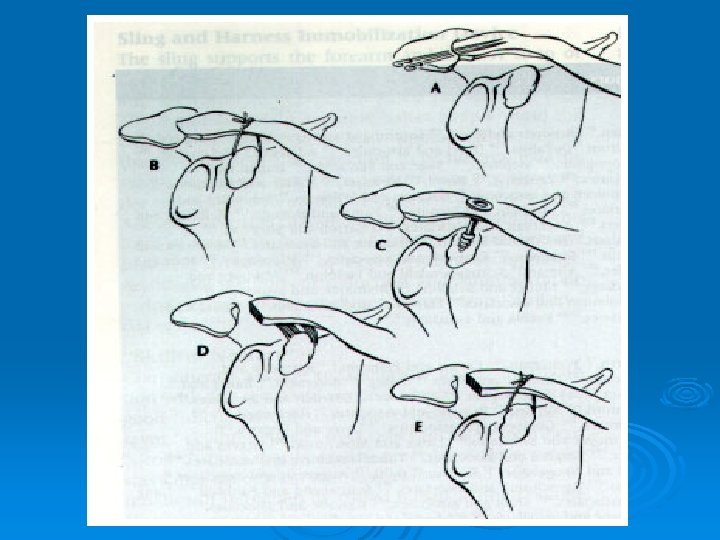
Nonoperative Treatment Type I and II l More than 35 different forms of management l Sling 10 -14 days, early and gradual PT l Heavy lifting and contact sports avoided for 8 -12 weeks l
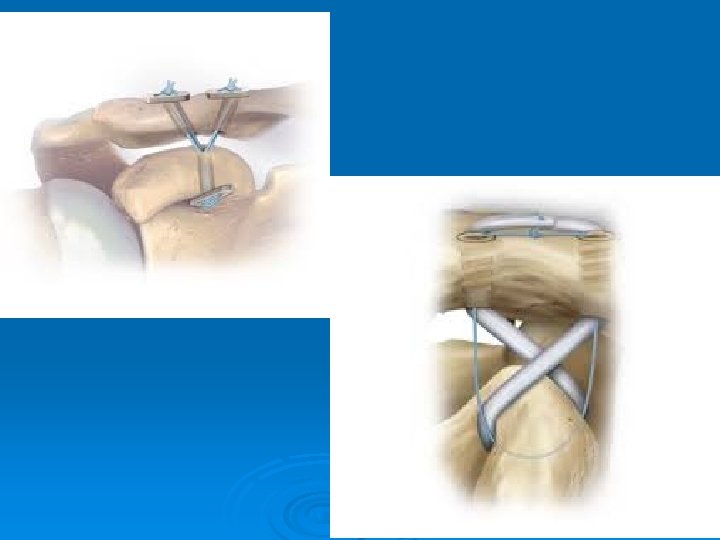
Operative Treatment Ø Grade III +/-, in younger, active Ø Grade IV, V and VI patients
Pelvis, Hip, and Thigh
Pelvis, Hip, and Thigh Ø Soft tissue injuries • Hip pointer l injury includes apophyseal avulsions and fractures and contusions of the iliac crest • rest, ice, compression, elevation, NSAIDs, physical therapy
Knee Injuries
Knee Ø 20% of all football injuries l 42 ACL tears per 1000 players per year Ø skiing accounts for at least one ACL tear per day at major ski resorts
Collateral ligamentous Injuries
Collateral ligamentous Injuries
ACL Exam Lachman test
ACL/PCL exam
Knee
Knee Dislocations Ø Named by location of the tibia to the femur Ø Mechanisms-Anterior, Posterior, Medial and Lateral
Knee Dislocations EMERGENCY l Limb threatening injury due to the high incidence of vascular injuries associated (25 -30%) l neurologic injury 9 -49% l management • immediate closed reduction on the playing field, followed by splinting; orthopedic/vascular evaluation
Knee Dislocations Document neurovascular status Ø Reduce by pushing the tibia in the appropriate direction Ø After reduction immobilize at 20 -30 degrees of flexion with NO casting or dressing materials Ø Arteriogram vs ABI debate post reduction Ø If the artery is repaired a fasciotomy is often done Ø Also look for neurologic injury the peroneal nerve is injured 14 -35% of the time Ø
Knee Dislocations Ø Popliteal is at risk due to proximal and distal fixation. Collateral arteries can’t maintain flow and pulses don’t exclude injury. Ø Repair 8 hrs. after injury 86% amputation rate Ø Repair < 8 hrs. 80% salvage rate
Patellar Dislocations Ø Extend knee l l Medial directed pressure on patella Knee immobilizer, may WB in extension
Shin Splints
Shin Splints Ø Topical or Oral NSAIDs Ø Compression Sleeves Ø Achilles Stretching Ø Most Importantly make sure it improves with these measures
Stress Fracture • Bone Scan MRI
Stress Fractures Protected or Nonweightbearing Long Term Issues • • • Nutrition Hormonal Training
The Ankle Sprain Ø Most frequently injured structure in all of sports
ANATOMY
Ø ATFL- 40% of injuries Ø ATFL and CFL- 58% Ø ATFL, CFL and PTFL- 3% Ø Deltoid- vast majority are a midsubtance tear
DIAGNOSIS Ø History- Mechanism Ø Physical examination l l l Location of Pain- Palpation Anterior drawer Talar tilt
In the Acute Setting Ø Joint Injury l l l Ø Articular injury Syndesmotic strain Fracture Tendon injury l l l Peroneal Anterior Tibialis Achilles
Treatment Ø Vast Majority-Nonoperative Ø Boot, SLC, Ankle brace du jour Ø Gradual return to full activities Ø Proprioceptive exercise (PT) l l Wobble Board 1 legged stand (+/- pillow)
Turf Toe l hyperextension injury of the first MTP joint associated with play on artificial turf
Turf Toe MRI
Thank You! (937) 428 -0400 ask for Linda