Focus Question 1 How are sports injuries classified






: a disruption of the fibres of muscle or tendon.")




 Rest: minimal movement for the first 48 -72")





















 Talk: talk and find out")






 People with asthma have extrasensitive airways. Triggers like dust,")



















 Most sporting codes match young athletes")






































































- Slides: 134
Focus Question 1 How are sports injuries classified and managed?
WAYS TO CLASSIFY SPORTS INJURIES Injuries are generally classified according to the cause of the injury or the way it occurred. e. g. Direct/Indirect Other classifications can be used such as the type of tissue damaged in the injury. e. g. Hard Tissue/Soft Tissue
DIRECT Caused by external forces to the body Injury occurs at the site of the force Can result in fractures, dislocations, sprains and bruises. Examples include: – A cricketer catching the ball and getting a dislocated finger – A footballer hit high and gets a broken cheekbone INDIRECT Can be caused by internal or external forces and usually results in an injury occurring at a site away from the intial force Can occur as a result of poor preparation or excessive movement. Can occur because of undue strain on muscles, tendons or ligaments and can cause irritation and possible structure damage. Examples include. : – Cyclist falls, puts out his hand dislocates shoulder – Netballer tears ligaments from twisting
SOFT TISSUE This includes: – Muscles – Tendons – Ligaments – Joint tissue – Fatty tissue Any injury to these are classified as soft tissue injuries Types of soft tissue injuries include: – Bruises (haematoma) – Sprains (ligaments) – Strains (tendons) – Lacerations (skin) – Dislocations (joints) – Tendonitis (tendons) HARD TISSUE Hard tissue includes: – Teeth – Bones Any injuries to these are classified as hard tissue injuries.
OVERUSE • Caused by excessive use over a long period of time. • Brought on by repetitive low impact exercise such as jogging or swimming. • Causes include poor training techniques, high intensity too soon, poor surfaces, inappropriate equipment and physical characteristics (flat feet, etc). • Injuries characterized by pain and inflammation. Common overuse injuries include: Shin splints Tendonitis Stress fractures Commonly called Repetitive Strain Injuries (RSI
SOFT TISSUE INJURIES
TEARS, SPRAINS, CONTUSIONS Tears (Strains): a disruption of the fibres of muscle or tendon. Occurs when the muscle/tendon is overstretched or the muscle contracted too quickly Sprains: a stretching or tearing of the ligament fibres, muscles or tendons supporting a joint. Occurs when a joint is extended beyond its range of movement. Strains and Sprains can be classified according to severity Grade 1 being the least serious up to Grade 3 being the most serious Contusions: a bruise (bleeding) into the soft tissue. Generally caused by contact with a solid (usually blunt) object.
SKIN ABRASION, LACERATION, BLISTERS, CALLUSES Skin abrasions: occur when the outer layer of the skin is removed, usually a scraping action. Lacerations: a cut, which will usually require stitches, depending on the depth of the cut. This is usually caused by a sharp object. Blisters: occur because of friction, which causes a pocket of fluid to form under the skin Calluses: when a build-up of dead skin forms at a site where constant friction has occurred.
INFLAMMATORY RESPONSE This is the initial stage of repair involving the first 48 -72 hrs after the injury as the body increases blood flow to the injured site.
Phase 1 – Inflammatory stage: Redness Heat Swelling Pain Loss of function Phase 2 – Repair stage (3 days to six weeks) Eliminate debris Form new fibres Produce scar tissue Phase 3 – Remodelling stage (6 weeks to months) development of scar tissue needs to strengthen in the direction force is applied dependant on amount of exercise and rehab routine aim to regain full function
MANAGING SOFT TISSUE INJURIES
RICER (Rest, Ice, Compression, Elevation, Referral) Rest: minimal movement for the first 48 -72 hrs Ice: causes blood vessels to constrict to decrease blood flow. Apply for 20 -30 mins every 2 hrs for 48 -72 hrs. Compression: ice should be firmly applied in a wide elastic bandage. This reduces swelling and provides support. Elevation: ensure the injury site is elevated above the heart. This reduces the volume and pressure of blood flow to the injury and reduces swelling. Referral: a medical assessment should be sought ASAP to as ascertain the full extent of the injury. See Table 11. 1 pg 410 of outcomes
SOFT TISSUE INJURIES – MUSCLES/TENDONS/LIGAMENTS ALWAYS THINK RECOGNITION OF INJURY AND APPROPRIATE MANAGEMENT- ACUTE – CHRONIC? USE: R - REST I – ICE C – COMPRESSION E – ELEVATION R – REFERRAL STRAINS/SPRAINS
SOFT TISSUE INJURIES DEFINITELY NO: H – HEAT A – ALCOHOL / ASPIRIN R – RUNNING (exercise) M – MASSAGE IN THE FIRST 24 – 72 HOURS OR LONGER
KNOW SOME BASIC ANATOMY The knee. A minefield to diagnose. Leave it to the experts!
LATERAL/MEDIAL ANKLE
ICE SHOULD BE AVAILABLE AT ALL TRAINING AND GAMES Where would you not apply ice to a soft tissue injury?
IMMEDIATE TREATMENT OF SKIN INJURIES The immediate response aims to: – – – Prevent further damage and reduce the risk of infection Reduce swelling Erase or minimise pain Restore flexibility Regain full function Prevent reoccurrence. For abrasions/lacerations: – Stop bleeding if necessary and clean the wound where possible – Apply non stick sterile dressing – Seek stitches if necessary For burns: – – Immediately apply cold running water No ice or creams Keep clean and sterile Seek medical advice
HARD TISSUE INJURIES
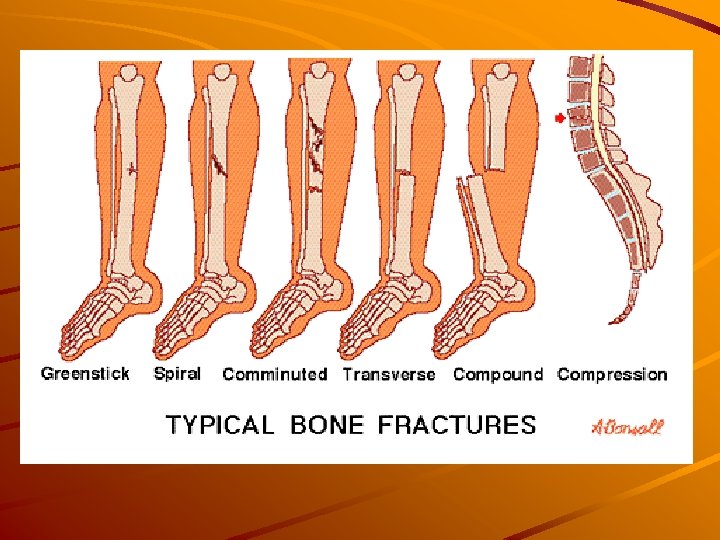
FRACTURES It is a break in a bone, which can be as simple as a small crack with no visible deformity, or complex, in that it may affect vital organs close to the fracture site.
Common causes include: Direct contact with: Others Objects The ground Indirect force on another body part (falling and landing on arm; fractured clavicle) Inappropriate muscular action (jumping from a height, landing on feet; fractured patella) Overuse, repeated trauma (running; stress fracture in foot)
Types of fractures include Simple/Closed: the bone is fractured but there is no wound at the site. Open/compound: the jagged end of a fractured bone protrudes through the skin. Complicated: the fractured bone damages local tissues, i. e. organs
Signs and symptoms include: Pain Reduced/no movement Local tenderness Deformity Irregular alignment Swelling
DISLOCATIONS It is where one bone is displaced from another Signs and symptoms may include: Loss of movement at the joint Obvious deformity Swelling and tenderness Pain at the injury site Subluxation: a partial dislocation where the joint dislocates and then relocates.
FRACTURE - DISLOCATION ALWAYS THINK DAMAGE TO SOFT TISSUES NERVES BLOOD VESSELS MINIMAL MOVEMENT - IMMOBILISE. TRANSPORT - AMBULANCE IN ALL CASES OF MAJOR FRACTURE OR DISLOCATION.
A DISLOCATION IS A FRACTURE UNTIL PROVEN OTHERWISE
FRACTURE - DISLOCATION GREAT CARE!
FRACTURE - DISLOCATION IMMOBILISATION?
DO NOT REDUCE! ICE - SUPPORT - TRANSPORT
MANAGING HARD TISSUE INJURIES IMMOBILISATION To another limb To another part of the body To a firm, smooth, straight object Splint above the joint above the fracture and below the joint below the fracture
MEDICAL TREATMENT Support the site with a sling or splint Check for impaired circulation Arrange for transport Implement RICER if it does not cause pain. NEVER ATTEMPT TO REDUCE/RELOCATE A DISLOCATION! DO NOT ATTEMPT TO RE-ALIGN FRACTURED LIMBS! SEEK MEDICAL ATTENTION! Complete application pg 413
ASSESSMENT OF INJURIES
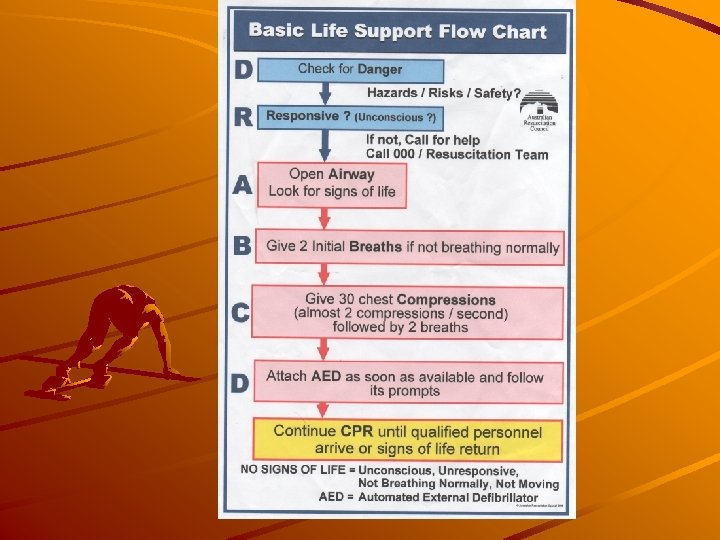
PROTOCOL WHEN INJURY/ILLNESS OCCURS – VITAL! D. R. S. A. B. C. D. T. O. T. A. P. S.
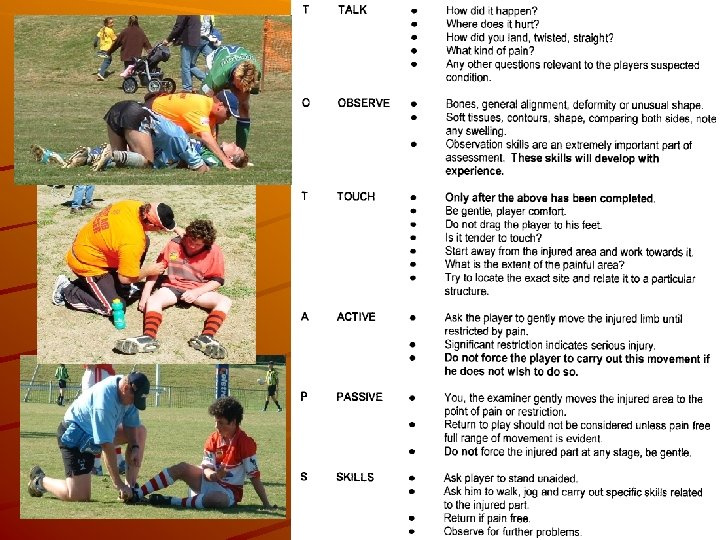
TOTAPS (Talk, Observe, Touch, Active movement, Passive movement, Skills) Talk: talk and find out exactly what happened. This will provide valuable info about the nature of the injury. Observe: look at the injury site and see if there any signs of obvious deformity. Compare opposite sides of the body. Touch: gently feel the areas for any sign of deformity or swelling and try to pinpoint the area of pain. Active movement: ask the player to perform a range of movements such as flexion, extension and rotation. If these can be done without pain, proceed. Passive movement: physically mobilize the joint as far or further than the patient did actively, aiming to identify painful areas and any instability Skills test: ask the player to perform a range of skills necessary for participation in the game, i. e. sidestep. CLICK FOR ROLE PLAY ACTIVITY SCENERIOS
REMOVAL FROM THE FIELD OF PLAY ALWAYS THINK DO NOT ATTEMPT TO REMOVE A PLAYER FROM THE FIELD WHO: IS UNCONSCIOUS. HAS A SUSPECTED SPINAL INJURY. HAS A MAJOR DISLOCATION/FRACTURE. HAS A SUSPECTED INTERNAL INJURY. HAS AN INJURY OR CONDITION THAT COULD BE SERIOUSLY WORSENED BY MOVEMENT.
REMOVAL FROM THE FIELD OF PLAY ALWAYS ENSURE AN AMBULANCE IS CALLED IN THE ABOVE SITUATIONS – OR IF IN DOUBT – PROTOCOL? CONSIDER: ALL CONDITIONS MUST BE MANAGED BY THE FIRST AID OFFICER UNTIL THE AMBULANCE RESPONDS. THIS WILL DEPEND UPON LOCATION. ISOLATED AREAS – DISTANCE. AVAILABILITY OF AN AMBULANCE. TIME IS AN IMPORTANT FACTOR! – YOU WILL BE OF GREAT ASSISTANCE TO THE FAO!!
Assessment can be stopped at any stage if the player cannot proceed or if danger is apparent. If the player can perform to the satisfaction of the assessor, the player can return to the game. If there is risk of further damage through continued play, remove the player from the game
HOW WOULD YOU MANAGE THIS?
Focus Question 2 How does sports medicine address the demands of specific athletes?
CHILDREN AND YOUNG ATHLETES
MEDICAL CONDITIONS (ASTHMA, DIABETES, EPILEPSY) People with asthma have extrasensitive airways. Triggers like dust, pollens, animals, smoke and exercise may cause the airways to swell and narrow. This leads to wheezing, coughing and difficulty breathing.
Management of an Asthma Attack Steps to follow in case of asthma attack: Sit the person comfortably upright. Stay calm and reassuring. Give 4 puffs of a blue reliever puffer/inhaler. These are best given through a spacer. Give one puff every 4 breaths for 4 puffs, holding the breath for 2 -4 seconds after a puff. Wait 4 minutes. If there is no improvement, give another 4 puffs. If little or no improvement, call an ambulance (000)
Some activities provoke an asthma attack more than others – there is significant risk with running, some risk with cycling and little risk with swimming. There is far less risk swimming in warm water.
It is generally agreed that exercise is of more benefit than no exercise at all, even if it leads to an attack.
Diabetes It is a complex hereditary or developmental disease where the supply of insulin is reduced or eliminated.
Type 1 diabetes is usually hereditary and the pancreas does NOT produce insulin at all. It is treated with injected insulin. Type 2 diabetes is usually developmental and is usually the result of a sedentary lifestyle and poor nutrition. Obesity is a significant determinant for type 2. It is treated with a managed diet and lifestyle adjustments.
Hypo-glycemia Low glucose levels. Mild cases cause: – Dizziness – Weakness – Disorientation Severe cases can lead to: – – – Convulsions Unconsciousness Brain damage A hypo is generally a blood sugar level below 3. 0 Hypo food: – – – Cordial/fizzy drink Jelly beans Juice Hyper-glycemia High glucose levels Sufferers will be: – – – Lethargic Thirsty Strong thirst Can result in damage to: – Eyes – Kidney – Nerves If left untraced, can cause a coma or death. Occurs as a result of too little insulin. Requires an injection of insulin and a doctor’s visit. A hyper is generally a blood sugar level of over 10. 0
Exercise is seen as an important part of the management of diabetes. It is important that insulin levels are balanced by either injection, food intake or exercise. Diet needs to be well balanced, with complex carbohydrates forming a significant portion Because exercise utilizes sugar, diabetics need a pre-game meal to raise blood sugar levels and hourly glucose supplements if exercise is prolonged.
Precautions for Diabetics Increase intensity and duration gradually Undertake exercise regularly Allow for adequate warm-up and cool-down Always have a supply of hypo food Constantly maintain blood sugar levels
EPILEPSY Epilepsy is a brain disorder characterized by recurring seizures and fits. Seizures are caused by sudden flurries of electrochemical activity in the brain, which disrupts the conversation between neurons.
Some people falsely believe that exercise will trigger a seizure, but this is not the case. Some anti-epileptic drugs (AED’s) cause fatigue, or problems with concentration, vision or coordination.
Exercise-related risk factors include: Extreme fatigue Lack of sleep Dehydration Electrolyte loss Hyperthermia Hypo-glycaemia
Safety suggestions include: Consult with doctor/specialist regularly Avoid known seizure triggers Ensure you keep an adequate supply of medication Alert your teammates to your condition Wear a medical bracelet Wear protective equipment Avoid contact sports, scuba diving, bungee jumping and boxing Avoid high altitudes Let people know of your walking routes
OVERUSE INJURIES Overuse injuries in children are created by the same factors as for adults. – – – excessive training repetitive movements incorrect training techniques Most overuse injuries in children occur in the lower limbs.
Some examples include: Achilles tendonitis: the tendons that connect the heel bone to the calf muscle become inflamed. Plantar fasciitis: the tissue that runs along the arch of the foot becomes inflamed. Stress fractures: repetitive pounding on foot and anklebone causes hairline fractures. Tendo-achilles bursitis: the fluid-filled sac between the Achilles tendon and the heel bone becomes inflames.
To avoid overuse injuries: Be knowledgeable about overuse injuries Use the right shoes Manage training and competition loads Avoid repetitive movements Be sure the level of competition is within the child’s range.
TREATMENT FOR STRESS FRACTURE IMMEDIATE REST 4 -8 WEEKS FREQUENT USE OF ICE POSSIBLE USE OF ANTI-INFLAMATORY MEDICATION MAINTAIN PHYSICAL CONDITIONparticipate in activities that don’t involve the injured part in pounding movementse. g. swimming Use exercises & corrective devices that improve body mechanics if caused by biomechanical factors
THERMOREGULATION This is the process that regulates and maintains the body’s temperature
A young athlete’s temp. regulation system is not as developed as adults. They: – Produce more heat when exercising – Have less perception of the need for rest and hydration – Have less blood volume – Have smaller sweat glands – Lower hemoglobin concentration – Lower cardiac output – Acclimatize slower.
Measures to take to address thermoregulation: Consider weather conditions when scheduling training and games Encourage appropriate clothing Incorporate water breaks and encourage around-the-clock hydration Be aware of warning signs of heat stress
MATCHING OF OPPONENTS (Growth and Development, Skill Level) Most sporting codes match young athletes according to age, and sometimes skill level, strength, size, etc.
Advantages of Disadvantages matching by age of matching by age -Equal -Differences in: experience -Size -Mental maturity -Weight strength -Equal skill -Self-esteem -Playing with issues peers -Convenience -Avoids health risks
APPROPRIATENESS OF RESISTANCE TRAINING Resistance training for adolescents usually focuses on their own body weight. There are safe and widely known exercises that can be used. (push ups, bridges, sit ups).
When can a child start weight training? This depends on: The child’s training base Ability to learn new techniques Their stage of growth Equipment available Quality of supervision What type of training best suits
Guidelines should include: Correct breathing and safe lifting techniques Appropriate warm up and cool down Progressive overload, but progress should be conservative Balance between muscle groups Low resistance with high reps; no max lifts Supervision Should not be competitive & strength specialisation should be avoided
ADULT AND AGED ATHLETES
HEART CONDITIONS As people age: Blood vessels lose elasticity Blood pressure rises The heart may weaken Maximum stroke volume decreases.
Some aged athletes may have heart attacks or heart-related problems Pre-screening is essential and work intensity needs to be lower Regular aerobic exercise can maintain or lower the loss of cardiovascular functioning Progress must be gradual Activity needs to be of moderate intensity
FRACTURES/BONE DENSITY Loss of bone density begins around 35 yrs of age. Regular aerobic and weight-bearing activities can reduce this loss. Osteoporosis sufferers should avoid activities, which involve a risk of falling, with focus on aerobic, low impact and safety with pain-free movement. Resistance training helps bone density
FLEXIBILITY/JOINT MOBILITY Joint pain, arthritis and tight muscles make flexibility training difficult. Regular, gentle flexibility exercises are essential. Stretch to strain, not pain. An increase in flexibility reduces injuries, reduces likelihood of falls and increases mobility
FEMALE ATHLETES
The following issues affect women and girls participation in sport. Sports trainers and coaches needs to be aware of how these issues impact on the females they coach. SPECIAL DIETARY NEEDS-increased iron & calcium requirements
EATING DISORDERS Anorexia Nervosa – Lack of nutrients in the blood – Degeneration of muscle mass – Characterized by selfstarvation and is potentially lifethreatening – Mainly affects teen females – They may exercises excessively Bulimia Nervosa – Binge eating and throwing up – Sufferers tend to use laxatives – Exercise excessively – Deprives body of nutrients – Leads to excessive weight loss – Damages the digestive tract
IRON DEFICIENCY Iron is an essential mineral for haemoglobin Deficiency leads to lethargy Affects performance and involvement Affects women more than men due to blood loss through menstruation If haemoglobin bellow 11 g per 100 m. L = anaemic
BONE DENSITY Quantity of calcium in the bones Can lead to fractures which result in poor mobility and pain Women need to be aware of osteoporosis after menopause. There is a need for adequate calcium intake and participation in regular weightbearing activities.
PREGNANCY Exercise is not only safe, but is recommended. Low impact, moderate exercise that includes adequate warm up and cool down can be beneficial in maintaining fitness levels, muscle tone, etc
MENSTRUATION Its affect on performance varies from person to person. Moderate exercise can help relieve menstrual stress. Heavy exercise may cause the absence of periods.
Focus Question 3 What role do preventative actions play in enhancing the well being of the athlete?
PHYSICAL PREPARATION
Pre Screening Pre-screening of participants prior to exercise is an important preventative measure. It involves assessing current fitness levels, medical history and conditions and previous injuries related to exercise.
SKILL AND TECHNIQUE Injuries can often result from poor skill and technique E. g. incorrect head positioning in a tackle
PHYSICAL FITNESS Being physically ready for sport reduces the chance of being injured. General fitness should be achieved before participating in most sports. For more specificity, physical fitness should be related to the sport, e. g. cardiovascular fitness for cross country runners, muscular strength and power for weightlifters, flexibility and muscular endurance for gymnastics. A lack of physical fitness places the athlete at risk of injury, e. g. participating in gymnastics with a lack of flexibility would increase the likelihood of a muscle tear, participating in a marathon with no cardiovascular fitness may result in a calf strain or a rolled ankle.
WARM UP An appropriate warm up should prepare the body for physical activity. Warm up routines need to be specific to the nature of the sport. For example, a warm up for a game of touch needs to include running with changes of direction, forwards and backwards running and ball passing. A good warm up gradually prepares the body for the demands that will be faced during participation in the sport.
COOL DOWN A cool down eases the body into recovery and reduces the severity of soreness. A cool down should not be as intense as a warm up.
STRETCHING Stretching is an essential part of any warm up and cool down. For warm ups, generally dynamic stretching is more effective. It gradually prepares the muscles and joints for activity and ranges of motion they may experience in the sport. Failure to stretch in a warm up may result in a muscular tear or joint sprain by forcing a joint beyond its range of motion. For cool downs, generally static stretching is most effective. Failure to stretch as part of a cool down will increase the incidence of soreness and affect further participation.
SPORTS POLICY AND THE SPORTS ENVIRONMENT
RULES OF SPORTS AND ACTIVITIES Rules assist the flow of play, create a safe environment for participation and protect from injury. Where a dangerous practice is identified a rule change may be able to reduce this risk. E. g. Spear tackle in Rugby League Appropriately accredited referees, umpires, etc should enforce rules.
MODIFIED RULES FOR CHILDREN Such modifications protect children from injury and ensure safety. They make allowances for the size and strength of young children. They often remove elements of the adult game that place participants at risk of injury. Examples include: Rugby leagues, mini footy and mod league. Minky Hockey, Roo Ball etc.
Modifications can include: Changes in size of playing field Changes in size or weight of playing equipment Changes in timing of games Changes in rules regarding numbers of players or inter change Others you can think of ? ? ?
MATCHING OF OPPONENTS This means that sport can be equitable for all participants and provisions may include divisions such as: – Weight – Age – Skill divisions Or as per Rugby Union smaller players may be able to weigh down a division
PROTECTIVE EQUIPMENT In most sports some form of protective equipment is used by players to ensure their safety during the game. Ground surrounds and equipment must also be made safe. Sometimes this involves use of protective equipment as well. E. g. Goalpost pads
APPAREL AND PROTECTIVE EQUIPMENT FOR HEAD AND NECK, EYES, BODY, TEETH AND FEET Some examples of these may include: – Neck braces – Goggles – Glasses – Arm guards – Gloves – Mouth guards – Sport-specific shoes – Headgear – Shoulder pads
SAFE GROUNDS AND FACILITIES Surfaces must be level and free from any protruding objects that may cause harm or injury Barriers must be in place to maintain spectators and separate the game from the crowd. If playing at night adequate lighting should be provided Any hard objects (goal posts, etc) should be padded. Others you can think of? ?
SAFE EQUIPMENT Any equipment used must be safe and not pose any hazard to any participants All individual equipment must be kept in good condition and checked before each game.
Most sports make provisions for the use of protective equipment. All protective equipment must: Adequately protect the wearer and others Allow freedom of movement Allow airflow Be comfortable Be of acceptable quality
ENVIRONMENTAL CONSIDERATIONS
THERMOREGULATION Thermoregulation is the process of maintaining core body temp
TEMPERATURE REGULATION Core body temp should be maintained at 37. 5 degrees Celsius. It is controlled by hypothalamus in the brain. Hypothermia: abnormally LOW body temp. Hyperthermia: abnormally HIGH body temp.
44 Upper limit of survival 42 Heat stroke – brain damage 40 Fever 37 Normal 36 Shivering and Co ordination 34 Violent Shivering 32 30 Semi – Consciousness 28 Body unable to regulate 26 Temperature IT IS INTERESTING TO NOTE THAT OUR THERMAL DEATH POINT IS ONLY 7 DEGREES EITHER SIDE OF OUR REFERENCE TEMPERATURE – 37 DEGREES C
Thermoregulation occurs in four ways: Convection: the transfer of heat away from the body by moving air currents. Radiation: the transfer of heat away from the body to a cooler environment. Conduction: the transfer of heat away from the body to something else (e. g. ice). Evaporation: heat loss through sweat.
CLIMATIC CONDITIONS Climatic conditions including temperature, humidity, wind, rain, altitude and pollution need to be considered prior to performance. The combination of high temperature and high humidity increase the level of risk of hyperthermia, particularly in relation to endurance performances. The combination of cold weather and wind increase the likelihood of hypothermia. Think about wind chill factor, effect of different climates, (dry heat vs humid) etc.
GUIDELINES FOR FLUID INTAKE Appropriate hydration is one of the main issues regarding temperature regulation and maintaining athletic performance. Fluid replacement before, during and after exercise is extremely important as even a small loss of fluid can affect an athlete's performance.
League. Safe DEHYDRATION ALWAYS THINK PREVENTABLE Drink water …. cool to cold. Drink before … during … after training and playing. Special care in hot/hot humid conditions. Thirst is a poor indicator of the need for fluid replacement What type of drink is the best ? Alcohol - NO High sugar/caffeine - NO Sports Drinks - YES WATER - YES, YES WEIGH PLAYERS
FLUID REPLACEMENT SAFE HYGIENIC PRACTICES ARE ESSENTIAL WITH WATER CONTAINERS AND THE DELIVERY OF WATER TO PLAYERS – PROTOCOL? DRINKS HIGH IN CAFFEINE AND SUGAR? (DISCUSS)
ACCLIMATISATION Acclimatisation involves preparing the body to perform in the climatic conditions that will be experienced during an event, e. g. heat, altitude, cold. It is an important factor in preparing for any event and contributes to preventing injury.
TAPING AND BANDAGING
PREVENTATIVE TAPING Refers to the application of adhesive or non-adhesive strapping or bandages to a joint area to protect, support or strengthen the joint during movement. In some sports that require high amounts of explosive movements there is considerable potential for injury. Taping in this situation is called PREVENTATIVE or PROPHYLACTIC taping
TAPING FOR ISOLATION OF INJURY Taping is often required after an injury and may be necessary during the rehab process. Injuries may be taped when returning to play for physical and psychological support. A player may use this until their body is fully accustomed to activity again.
BANDAGING FOR IMMEDIATE TREATMENT OF INJURY Bandaging is more commonly used for the treatment of soft tissue injuries. Bandaging can help reduce swelling, support a joint or muscle and restrict movement. Generally, elastic bandages or slings are used. To be effective, the correct technique and firmness need to be applied to the injured area.
Taping Principles: Non-elastic taped for support Begin with anchors Ensure evenness of tension Overlap each application Maintain even pressure Reapply if circulation is cut Avoid creases
Avoid continuous taping Always tape in the direction to tighten Completely cover skin with no gaps Finish with locks Remove with blunt scissors
TAPING ALWAYS THINK EFFECTIVENESS Give support without limiting function. Does the player really need taping? IF SO Decide why. Know the anatomy involved. Decide how. Know materials to use. REMEMBER Rehabilitation first – consult physiotherapist. TAPING SHOULD ONLY BE APPLIED BY PERSONS TRAINED TO USE TAPING TECHNIQUES!
Explore the following links for demonstrations on taping an ankle, wrist and thumb. Ankle http: //emedicine. medscape. com/article/86495 -overview http: //www. elastoplastsport. com. au/Injury/Taping. Techniqu es. aspx http: //www. physioadvisor. com. au/11244150/ankle-tapingankle-strapping-physioadvisor. htm Wrist http: //www. physioadvisor. com. au/11376450/wrist-tapingwrist-strapping-strap-wrist-phy. htm Thumb http: //www. physioadvisor. com. au/12460050/thumb-taping -thumb-strapping-strap-thumb-phy. htm
HOW IS INJURY REHABILITATION MANAGED?
REHABILITATION PROCEDURES
PROGRESSIVE MOBILISATION After treatment it is essential for movement to be restored ASAP. It involves gradually extending the range of movement May initially be passive until active movement can be restored
GRADUATED EXERCISE • STRETCHING • CONDITIONING • ACHIEVING TOTAL BODY FITNESS
STRETCHING To reduce scarring, stretching is important. The most appropriate are proprioceptive neuromuscular facilitation (PNF). Initially, movement should be within pain barriers and gradually increased as strength increases
CONDITIONING It involves adapting the body to a range of strength, agility and power skills to ensure full function This is followed by exposure to noncompetitive situations where full movement is required.
TOTAL BODY FITNESS It is regaining pre-injury fitness Must involve all principles of training, particularly progressive overload. Programs should involve all muscle groups and energy systems. Adaptations should include: – – – – Hypertrophy of muscles (increased size) Increased capillarisation and blood flow Strengthening of ligaments and tendons Increased elasticity of fibres Increased joint mobility Absence of pain Full confidence in the injury Fully restored balance and coordination
TRAINING With total body fitness restored, full training can commence. The athlete will be expected to train fully with no pain. This involves warm up, conditioning, drills, skills, development exercises, tactics and cool down.
USE OF HEAT AND COLD The application of heat and cold to an injured site is important in the healing process. Cold is used for the immediate treatment of injury as it prevents swelling due to internal bleeding. It can be applied by using ice packs, ice contained in plastic and wrapped in a towel or cool water/ice baths and immersion for short periods. Cold will also be useful after exercise and training when the injured area has been through a workout. Heat should not be used in the early stages of injury while bleeding at the injured site is still occurring. It may help in promoting movement and blood flow and relaxing the muscles through rehabilitation.
RETURN TO PLAY
INDICATORS OF READINESS TO RETURN TO PLAY ELASTICITY: flexibility returned STRENGTH: new tissue is strong and able to support body in stressful movements PAIN FREE: if there is no visible or communicated pain, the athlete has passed this condition of readiness to return to play MOBILITY: the joint where the injury was sustained must have a suitable range of movement and mobility to suit the playing conditions BALANCE: able to balance on injured limb
MONITORING PROGRESS Pre test and post-test: the progress of the athlete must be monitored before and after a fitness test to ensure that there is no damage or harm done during the test which may delay the return to play.
PSYCHOLOGICAL READINESS After an injury, an athlete may feel quite anxious about returning to play. Even if the athlete is physically recovered from an injury, they may not be psychologically ready to return to elite competition. In this case, a coach may play them in a lower division until they are back to their best
SPECIFIC WARM UP PROCEDURES After injuries, it is sometimes necessary to have a specific warm up where the focus is on preparing the injury site for the proceeding impacts of play. A specific warm up may include: – Extra or varied stretches – Strength work – A more concentrated warm up
RETURN TO PLAY POLICIES AND PROCEDURES Individual sports will have their own specific return to play policies and procedures. The athlete's wellbeing should be central to any return to play policy. Contact sports usually have a policy about returning to play after a head injury.
ETHICAL CONSIDERATIONS
PRESSURE TO PARTICIPATE Many coaches will put pressure on valuable players to return early so that their playing roster is bolstered. The more professional the sport, the more intense the pressure becomes. This also carries risks, such as: – – – Long term health problems Arthritis Early retirement
USE OF PAIN KILLERS Some elite players have injuries heavily strapped or painkillers injected so that they can return ASAP. Irrespective of financial gain, it is unwise to return early Pain indicates tissue damage and is a warning that rehab is necessary. Painkillers de-sensitize the area and leave it susceptible to further injury, prolonging the healing process and may lead to permanent damage.