SPORT INJURY OF KNEE Dr FARZAD RAVARI M


























- Slides: 30
SPORT INJURY OF KNEE Dr. FARZAD RAVARI M. D SPECIALIST ORTHOPEDIC SURGEON Cedars J. A int. Hospital
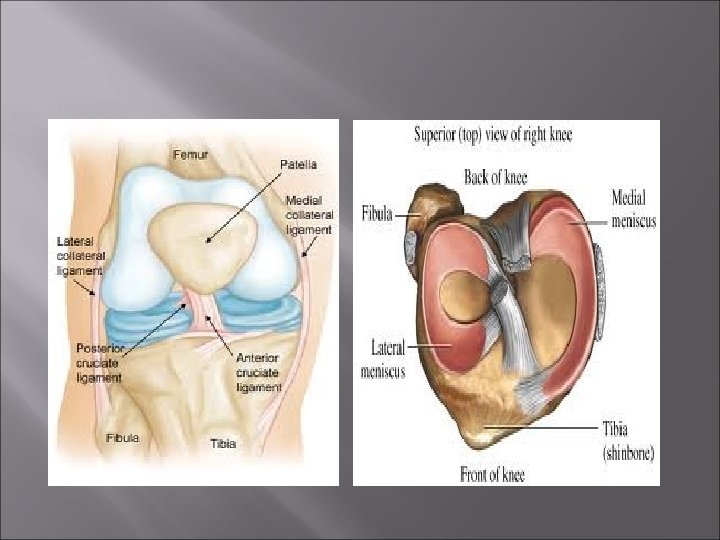
ANATOMY
FEMORAL CONDYLE Ant. Of Med Condyle =longer Med Condyle= Wider On medial= wheel on a flat On lateral=wheel on a dome PATELLA Wider in prox. pole than distal In Extension=distal portion of lat. patellar facet articulate with lat. Fem. condyle In Flexion=med. Facet with med. Condyle In 45’ flex=mid portion In full flex= both facet but most pressure over med. facet
EXTRA ARTICULAR SYNOVIUM CAPSULE CO-LAT LIG. MUSCLES Quardiceps rectus femoris vastus intermedius vastus lateralis vastus medialis -Gastrocnemious -Medial Hamestring pes-ancerinous: semi tendinosus gracilis sartotious Semi-membranous -Lat. Hamertring biceps femoris -Illiotibial band
MECHANICS OF KNEE JOINT=HING+PIVOT First 20 ‘ flex= rocking Range of motion=0’-140 flex 5 -10’ hyperextension In 90’ flex= 25 -30’ rotation tibia
MINISCUS Medial Miniscus: C shape, larger radius wider post horn attach to ACL , inter condylar eminence Lat Miniscus: small diameter thick prephery wide body more mobile
Miniscal repair Miniscus has: prepheral vasular area mid portion semi vascular central avasular area After injury: Fibrin clot fill the gap Healing =10 weeks Maturation = several months Regeneration only happen in vascular area
MECHANISM OF INJURY Rotation in semi flex Femur push miniscus toward center & post horn caught between femur & tibia then causes tearing
Type of miniscal tear -Longitudinal > med miniscus bucket handle -Transverse & oblique > in lat miniscus -Long+trans -Tear+ discoid miniscus -Tear+ cyst
Diagnosis -Locking+++ve some times only extension lag -lockong---ve giving way effusion atrophy of Q Tenderness over joint line Mc –Muray sign ++VE Re- Mc muray ++ve Apley test + ve
Treatment Conservative: Small tear < acm < 3 mm displacement Esp in prepheral area Protection 3 -6 wks will be healed Surgical Open minisectomy total miniesctomy Artheroscopic miniscal repair Artheroscopic partial or sub total minisctomy
Complication of total minisectomy Ant. post. Ridge of margin of fem condyle Flattening of condyle Decrease joint space Laxity of ligaments Osteo arthritis
Miniscal repair Acute, 1 -2 cm in peripheral zone
Miniscal Allograft Deep freeez Freez-drying cryopreservative
Miniscal cyst Lat miniscus>3 -10 med minis. Etiology: *contusion , Hematoma *Degenerative by age *Synovial cyst *Microscopic tear>> displacement of synovial cell into miniscus>>> secret Acid MPS P/E: *palpable ant. , prox. to fibular head *Piasani test++: small cyst disappear by knee flex. * large cyst can erode tibial condyle Treat: partial minisectomy+ decompression ofcyst
Miniscal cyst
Discoid miniscus Lat> med Cause snapping knee syn NORMAL
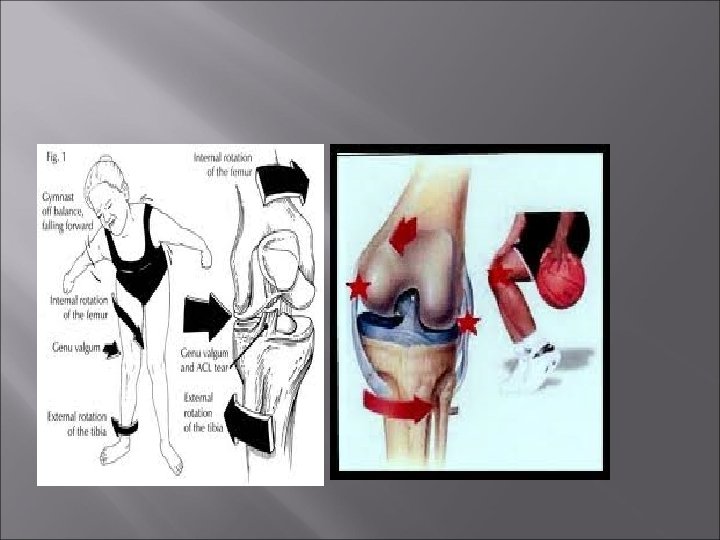
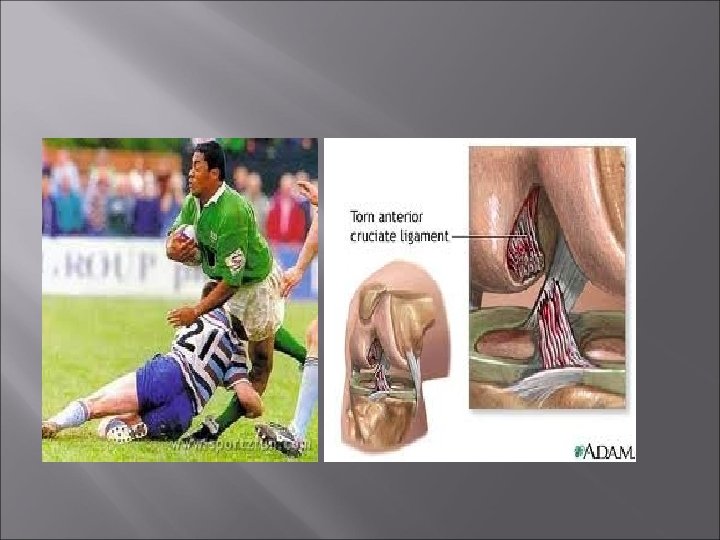
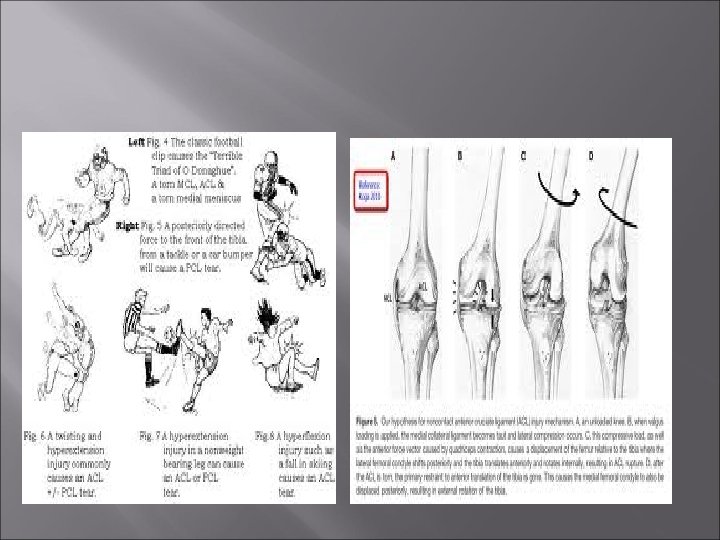
Mechanism of Ligament injury Abd+Flex+Int Rot femur on tibia 1 - med. Capsule injury 2 - ACL tear 3 - Med. Miniscus tear (Triad of O’Donoghue)
Mechanism of Lig. injury Add+ Flex+ Ext. Rot. 1 - Lat Capsule 2 - ACL 3 - Lat miniscus * Hyper- extension ACL * Ant –Post Displacement PCL
Med colateral Lig. Injury
Lat. Co lateral lig inj.
Muscle injury
Fractures
BURSA House maid knee Due to crawling , kneeling Some times infected
Treat of sport knee injury Rest Ice Compression Elevation