CMV infection in HSCT recipients Current trends and











 l l - Belongs to a new class of compounds (a")


















 l")








 CMV EBV Ad. V BKV HHV-6 CR + PR 94 (16/17)")




- Slides: 46
CMV infection in HSCT recipients; Current trends and perspectives Prof. Per Ljungman Center for Allogeneic Stem Cell Transplantation Karolinska University Hospital and Karolinska Institutet Stockholm, Sweden
Disclosures l l l Advisory boards: Ai. Curis; Merck, Oxford Immunotech Investigator: Merck, Astellas, Oxford Immunotech DSMB/DRC: Shire
Timing of management options Viral load Treatment of established disease Viral disease Pre-emptive therapy Diagnosis of viral infection Prophylaxis Time
Treat established CMV disease l l A failure of strategy Associated with significant mortality in the most severely immunosuppressed patients
What is the risk for CMV disease today? Placeboarms in prospective randomized studies Author Journal Year N Incidence Marty et al Lancet ID 2011 227 2. 4% Marty et al N Engl J Med 2013 59 3. 0% Chemaly et al N Engl J Med 2014 33 0% Marty et al N Engl J Med 2017 170 1. 8%
Patients in and outside of clinical trials
Real life probability of CMV disease Green et al: Lancet Haematol 2016
CMV Following Hematopoietic Cell Transplantation Current Strategies Infection Universal prophylaxis ‘Risk-adapted’ prophylaxis To prevent CMV infection/reactivation in high-risk subgroups Pre-emptive (A)symptomatic CMV infection detected by a screening assay Therapy CMV disease Disease J. Maertens 2018
The fight! Prophylaxis Preemptive therapy
CMV replication is associated with mortality! Retrospective analysis of seropositive patients monitored by q. PCR. Effect of detection of any level of viremia Multivariate Cox model All cause mortality Non-relapse mortality Day 0 – 60 2. 6 (1. 4 – 5. 0) Day 61 – 365 1. 7 (1. 2 – 2. 4) 1. 3 (0. 9 – 2. 0) 1. 8 (1. 2 – 2. 6) Green et al Lancet Haematol 2016
Prophylaxis – previous studies l Aciclovir/valaciclovir are not effective enough l Ganciclovir and foscarnet are effective but toxic in HSCT l Valganciclovir effective in SOT l Resistance / intolerance remains as problems l Immune globulin is not effective in HSCT l Failure of phase III studies for maribavir, brincidofovir, and CMV DNA vaccine
Letermovir (AIC 246) l l - Belongs to a new class of compounds (a 3, 4 -dihydro-quinazoline 4 -yl-acetic acid derivative) Inhibits CMV through a novel mechanism involving the viral terminase complex l Potent CMV activity in vitro & in vivo l No effect on other herpesviruses l No cross-resistance with drugs currently used in treatment of CMV
Time to Clinically Significant CMV Infection Primary Efficacy Population; Patients without Detectable CMV DNA at Randomization Cumulative Rate of Clinical Significant CMV Infection (%) 60 50 Letermovir vs. Placebo Stratified log-rank test, Two-sided p=0. 0005 Placebo 40 30 20 Letermovir 10 0 0 2 6 10 14 18 24 254 77 212 70 Post-Transplant Week Letermovir 325 Placebo 170 320 169 299 135 279 96 270 85 Subjects at risk 14
Time to Clinically Significant CMV Infection Primary Efficacy Population; Patients without Detectable CMV DNA at Randomization High Risk Stratum Low Risk Stratum 60 Log-rank two-sided p<0. 0001 Cumulative Rate of Clinical Significant CMV Infection (%) Placebo 50 50 40 40 Placebo 30 30 20 20 10 10 Letermovir 0 0 0 2 4 6 8 10 12 14 16 18 20 22 24 Post-Transplant Week 15
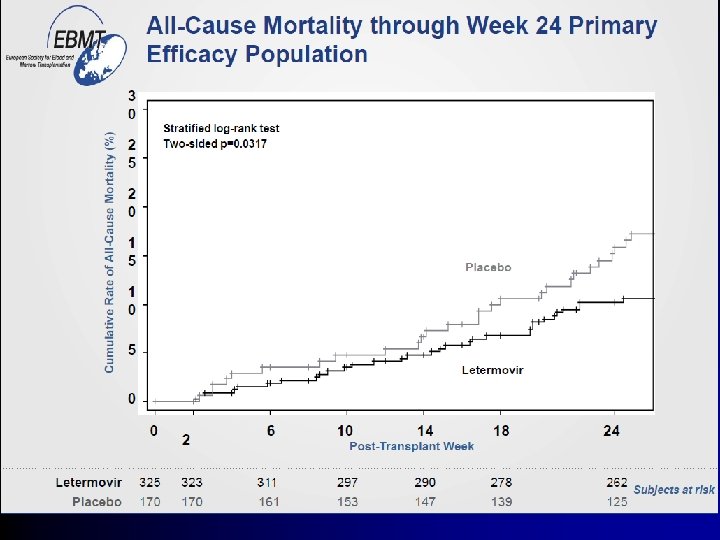
All-cause mortality through w. 24 Letermovir Placebo Patients with CS-CMVi 17. 7% 29. 5% Patients without CS-CMVi 19. 7% 18. 3% Letermovir neutralizes the negative effect of significant CMV replication
Real life experience l Implemented at some centers at all seropositive patients. Some centers have been using it in ”high risk” patients only Some resistance is developing. Break-throughs with disease have been seen l Secondary prophylaxis have also been used (off label) l l l
Prophylaxis in allogeneic HCT; Antiviral drugs ECIL 2017 Drug Grading References Comment Aciclovir CI Prentice, Lancet 1994 Milano, Blood 2011 Less efficient than valaciclovir Valaciclovir BI Ljungman, Blood 2002 Winston CID 2003 Milano, Blood 2011 Association with preemptive strategy Ganciclovir/ CI Winston, Ann Intern Med 1993 Goodrich , Ann Intern Med 1993 Montesinos, BBMT 2009 Cord blood SCT Valganciclovir CIIh Foscarnet DIIu Ordemann, Ann hematol 2000 Bregante et al, Bone Marrow Transplant 2000 Letermovir AI Marty et al, NEJM 2017 Ljungman et al; Lancet Infect Dis; in press 2019
How far have we come?
What is the rationale for monitoring and preemptive treatment A sensitive diagnostic test is available CORRECT – Many studies A positive result is predictive for development of disease Partly CORRECT – Not for all types of disease Early intervention can prevent disease CORRECT An effective (and safe) antiviral drug is available YES AND NO
Testing issues l All PCRs are not created equal!! • • • Starting materials DNA extraction methods Primer/probe selection Variability International standard!!
The variability in CMV DNA results reported on individual samples have been reduced by the international standard, but ongoing clinically relevant variability persists, preventing meaningful interassay result comparison CID 2017
CMV viral load cut-off values l There is major variability between patients l There is still variability between assays l It is therefore not possible (or meaningful) to give a standard cut-off reocmmendation to be used at different centers (outside clinical trials)
First line preemptive therapy – ECIL 2017 • The only data available for preemptive therapy of asymptomatic patients exists in allogeneic HSCT recipients. • Preemptive antiviral therapy based on detection of CMV nucleic acid (or antigen) is effective for prevention of CMV disease (AI) • Either iv ganciclovir or foscarnet can be used for first line preemptive therapy (AI) • Valganciclovir can be used in place of iv ganciclovir or foscarnet (except in patients with severe GI GVHD); AIIu) • The combination foscarnet+ ganciclovir is not recommended (DIII) • The choice of drug depends on time after HSCT, risk of toxicity, and previous antiviral drug exposure Ljungman et al; Lancet Infect Dis; in press 2019
Repeated CMV reactivations l l Common in high risk patients Frequently poor activity/tolerability of existing antiviral drugs l Associated with poor T-cell control of CMV l Increased risk for resistant strains
Second and third line preemptive therapy • The alternate drug of ganciclovir/valganciclovir or foscarnet can be considered for second line pre-emptive therapy (AIIu) • Cidofovir can be considered for second/third line pre-emptive therapy (3 -5 mg/kg/week) but careful monitoring of the renal function is required (BIIu). • The combination of ganciclovir and foscarnet might be considered for second/third line pre-emptive therapy (CIIu) • Reduce immunosuppression if possible (BIII) • No recommendation can be given for the antiviral drugs in development • Leflunomide or artesunate can be considered in patients resistant/refractory to available antiviral drugs (CIII) • Addition of iv immune globulin for preemptive therapy is not recommended (DIII) Ljungman et al; Lancet Infect Dis; in press 2019
How common is antiviral resistance in HSC recipients? Varies between patient populations Ganciclovir resistance 0% 0% in a prospective randomized study (Boeckh et al Ann Intern Med 2015) in auto and allo SCT non-haplo recipients in a large prospective cohort study 9. 6% in haploidentical allo SCT recipients (Shmueli et al JID 2013
CMV genes and antiviral drugs
Most “resistance” is clinical!
Causes for “clinical” resistance l If you give oral therapy, does the patient take the drug? l Vomiting? l Does the patient absorb the oral drug? l What are the drug levels? TDM for ganciclovir l Viral replication kinetics l Poor T-cell function
Response to antiviral therapy takes some time! Mattes et al JID 2005
When to Suspect Drug Resistance l High risk clinical setting (severe T-cell immunodeficiency) l Prolonged drug exposure (usually > 6 weeks) l l Rising viral load or persistent culture positive >2 weeks after full dose therapy (GCV/VGV) Progressive disease after prolonged therapy
Treatment of resistant/refractory patients l l l Increase dose of ganciclovir/TDM Foscarnet Cidofovir l Maribavir Letermovir/ Brincidofovir l T-cells l l Leflunomide Artesunate
Foscarnet/cidofovir l Standard second line therapies l Most ganciclovir resistant patients can be managed l Multidrug resistance is rare l However, toxicity problems are common (renal toxicity, electrolyte disturbances, cystitis)
Maribavir l Sucessful phase II study for prophylaxis l Failed phase III studies for prophylaxis l Case series on refractory patients. l Phase II study of refractory patients finalized. l Phase III studies ongoing
Maribavir for Treatment of CMV Resistant or Refractory to Ganciclovir or Foscarnet: A Phase 2 Trial Screening Study drug administration (maximum 24 weeks) Weeks 1 -3 Weeks 3 -6 Follow-up (post-treatment weeks 1 -12) Weeks 6 -24 MBV 400 mg twice daily • HCT or SOT recipient • R/R CMV • ≥ 1, 000 CMV DNA copies/m. L MBV 800 mg twice daily Week 1 Week 4 Week 8 Week 12 MBV 1200 mg twice daily Randomization MBV doses blinded At week 3 and week 6 visits, minimum virologic responses are required for study drug treatment to continue PCR CMV testing Day 1, weekly to week 6 Papanicolaou G, et al. BMT Tandem 2017. Abstract 45. Clinical. Trials. gov identifier: NCT 01611974. Study evaluations/PCR CMV testing Every 2 weeks to week 12; weeks 16, 20, and 24 G. Papanicolaou 2018
Time to Undetectable Plasma CMV DNA was Similar Across all Maribavir Doses Papanicolaou G, et al. BMT Tandem 2017. Abstract 45. Clinical. Trials. gov identifier: NCT 01611974. G. Papanicolaou 2018
Letermovir l l l No data in children Likely to be tested in refractory/resistant situations (off label) Dose not determined. Very limited published data Resistance found in vitro and in vivo. Unclear clinical relevance as of today
Adoptive T-cell therapy l l In develpment for 30 years Major advances in technology have been achieved over time Most (almost all) data are from phase I – II type studies In practice, it is still far away from routine therapy/ available for most centers
Effect of CTL Uhlin et al CID 2012
Response, % (n/N) CMV EBV Ad. V BKV HHV-6 CR + PR 94 (16/17) 100 (2/2) 71 (5/7) 93 (14/15) 100 (2/2)‡ CR 65 (11/17) 100 (2/2) 71 (5/7) 33 (5/15) 0 (0/2)‡ Safety: grade 1 skin GVHD, n = 1 (resolved); chronic skin GVHD flare, n = 3 (immunosuppression discontinued); transient fever, n = 2 Tzannou I, et al. J Clin Oncol. 2017; 35(31): 3547 -3557.
How do I treat very difficult CMV problems? The numbers game l In real life, this is quite rare l 1 -2 patients/year at my center l Individual management based on transplant history, GVHD, tolerability of drugs, possibility to use immune therapy.
One size doesn’t fit all
A look into the situation in 2022 Or………………
Since transplanters are innovative "The person who takes medicine must recover twice, once from the disease and once from the medicine. " - William Osler, M. D.