CHEILO GNATO PALATOSCHISIS Clefts are the congenital defects







































- Slides: 43
CHEILO – GNATO PALATOSCHISIS
• Clefts are the congenital defects that may cause severe functional and aesthetic problems. • The prevalence has increasing tendecy. While at the beginning of this century it was about 1 in 1600, in 1940 it was 1: 770 and in 1990 1: 500. • The prevalence varies between racial groups. The clefts are very rare among the Negroes and the most frequent are in chinese, japanese and american indian population.
• • • 1. 2. 3. 4. 5. 6. There is often a history of clefts within a family the mode of inheritance is not simple Many enviromental insults to the embryo infectious diseases corticosteroids mechanical and chemical insults alkohol drugs X-rays can produce clefts in animals but whether these are of any significance in human population is uncertain.
• Many classifications of clefts have been proposed but none is entirely satisfactory. Nowadays the classification based on embryological principles is used.
DEVELOPMENT OF THE FACE Development of the face starts from ventral part of the head process of an embryo and the first branchial arch. The face develops mainly between the 4 th and 8 th weeks. By the end of the embryonic period ( eight weeks ) the face has an unquestionably human appearance.
DEVELOPMENT OF THE FACE The first branchial arch develops two elevations called the “ maxillary prominence” and “mandibular prominence”. In the 4 th week the five facial primordia are around the stomodeum ( primitive mouth ): • The large “frontonasal prominence” constitutes the cranial boundary of the stomodeum. • The paired “maxillary prominences” of the firsth branchial arch form the lateral boundaries and • the paired “mandibular prominences” of the same arch constitute the caudal boundary of the stomodeum.
Early formation of the face about 24 days after conception
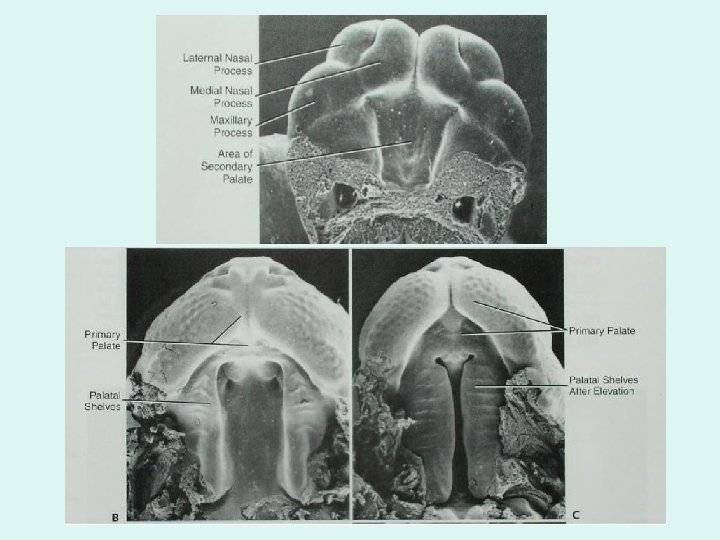
Bilateral oval-shaped thickenings of the surface ectoderm, called “nasal placodes”, develop on each side of the caudal part of frontonasal elevation Horseshoe-shaped “medial and lateral prominences” develop at the margins of the nasal placodes. As a result, the nasal placodes lie in depressions called “nasal pits”.
The maxillary prominences grow rapidly and soon approach each other and the medial nasal prominences. During the 6 th and 7 th weeks the medial nasal prominences merge with each other and the maxillary prominences.
• Diagrammatic representation of the structures at the beginning of the 5 th week when fusion is just beginning. • Relationship at the beginning of the 6 th week, when the fusion is well – advanced. • Schematic representation of the contribution of the embryonic facial processes to the structures of the adult face
DEVELOPMENT OF THE FACE As the medial nasal prominences merge with each other, they form an “intermaxillary segment” of the maxilla. This segment give rise to: • the middle portion of the upper lip called the philtrum • the premaxillary part of the maxilla and its associated gingiva • the primary palate The lateral parts of the upper lip, most of the maxilla and the secondary palate form from the maxillary prominences. These prominences merge laterally with the mandibular prominences
DEVELOPMENT OF THE FACE The mandibular prominences merge with each other in the fourth week and the groove between them disappears before the end of the fifth week. The mandibular prominences give rise to: • the mandible • lower lip and • the inferior part of the face The frontonasal prominence forms the forehead and the dorsum and apex of the nose. The sides of the nose are derived from the lateral nasal prominences.
DEVELOPMENT OF THE PALATE The palate develops from the: : • the primary palate and • the secondary palate Although palatogenesis begins toward the end of the 5 week, fusion of the palate´s parts is not complete until the 12 week.
DEVELOPMENT OF THE PALATE The primary palate – or median palatine process, develops at the end of the fifth week from the innermost part of the intermaxillary segment of the maxilla. It forms a wedge-shaped mass of mesoderm between the maxillary prominences of the developing maxilla.
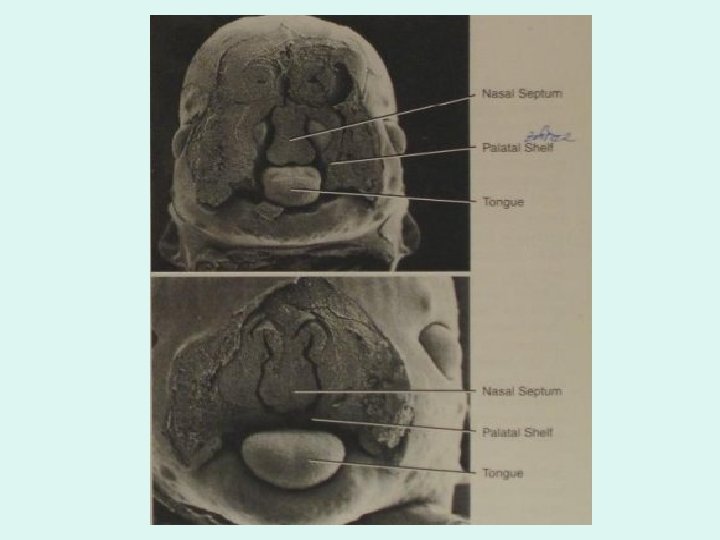
DEVELOPMENT OF THE PALATE The secondary palate – develops from two internal projections from the maxillary prominences, called the lateral palatine processes. These shelflike structures inicially project inferomedially on each side of the tongue. As the jaws develop, the tongue moves inferiorly and the lateral palatine processes gradually grow toward each other and fuse. They also fuse with the primary palate and nasal septum.
The fusion of the palatal processes begins anteriorly during the 9 th week and ends posteriorly in the region of the uvula by the 12 th week. The palatine raphe indicates the line of fusion of the lateral palatine processes. The posterior portion of the lateral palatine processes do not become ossified. They extend beyond the nasal septum and form the soft palate and uvula.
CLASSIFICATION OF THE CLEFTS : The embryological classification divides clefts in four groups: 1. Clefts of the primary palate: may involve only the lip or the lip and alveolar process as far back as the incisive foramen. 2. Clefts involving both the primary and secondary palate. 3. Clefts of the secondary palate: may involve the soft palate only or the soft palate and hard palate as forwards as the incisive foramen. 4. Special clefts of the face: this group is not based on embryology but on the topography. It involve: medial cleft of the upper lip, medial cleft of the nose, aplasia of the ala nasi, unilateral or bilateral oblique cleft of the face, transverse cleft of the face, cleft of the lower lip, cleft of the mandible. These clefts are very rare.
MECHANISMS OF CLEFT FORMATION : • A cleft is formed because the epitelium or the mesoderm failed to unite the various processes. • A cleft also may be caused by inadequate mesoderm, or mesoderm that may have had insufficient migrating potential. • It is thought that clefts of the primary palate result from failure of mesenchymal consolidation whereas clefts of the secondary palate may arise if the palatal processes fail to come into contact.
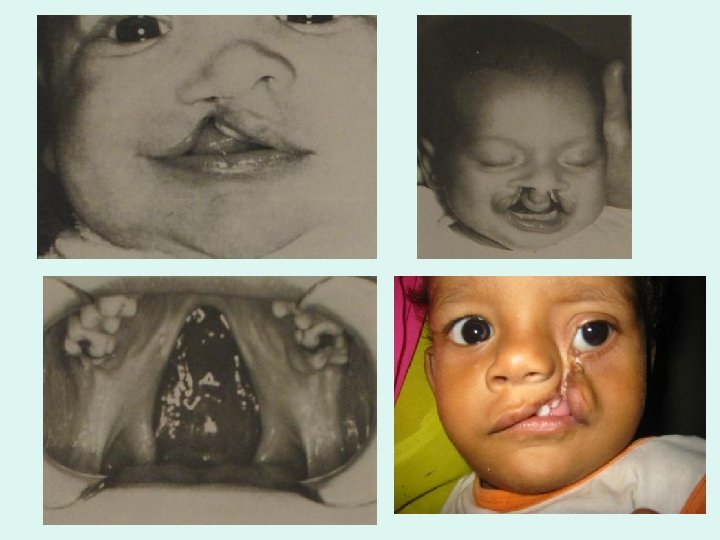
CLEFT OF THE PRIMARY PALATE • The deformity varies from notching of the lip to a complete lip cleft with alveolar involvement. • It may be unilateral or bilateral. • The most striking clinical feature of the unilateral cleft is the distortion that occurs due to the major segment of the alveolus moving away from the cleft side. Thus, the major segment is on the noncleft side, and the minor segment on the cleft side. The lip is distorted, and the nose is always flattened on the cleft side.
CLEFT OF THE PRIMARY PALATE • The alveolar cleft is in the lateral incisor area so the anomalies of this tooth are often seen : it may be absent or poorly developed and/or malpositioned, or there may be dichotomy of the lateral incisor with one small pegshaped tooth on either side of the cleft line. The central incisor on the side of the cleft is often rotated and hypoplastic. Normally the arch form is good.
CLEFT OF THE PRIMARY PALATE • In the cases of bilateral cleft there is abnormal position of the primary palate, or premaxilla, which is rotated and everted out of the oral cavity. Thus the two major segments form the lateral aspect of the mouth, and the minor segment protrudes extraorally in the midline.
CLEFT OF THE PRIMARY AND SECONDARY PALATE • These may be unilateral ( if primary palate involved on one side only) or bilateral ( if primary palate involved on both sides ). • In cases of unilateral cleft there if a major segmet that consist of the lip, premaxilla, frontal and one lateral part of alveolar process, one half of the hard palate which is connected with womer and nasal septum. The minor segment comprise of the rest of lip, alveolar process and hard palate. There may be wide gap between the segments or they may collapse.
CLEFT OF THE PRIMARY AND SECONDARY PALATE • In the cases of bilateral cleft the premaxilla with womer and nasal septum form an independent segment which protrudes extraorally in the midline or wedges inside the oral cavity. These cases present the greatest problems: surgical, dental, orthodontic and speech.
CLEFT OF THE SECONDARY PALATE • These vary from a submucous cleft of the soft palate to a complete cleft of the soft and hard palate as far forward as the incisive canal. • The submucosus cleft means that there is diastasis of the soft palate muscles and space between them is filed by membrane.
TREATMENT OF CLEFTS : • In order to improve the function and appearance of the various parts of the face and oral cavity many different specialists have to work in close collaboration. • A great deal of consideration must be given to the parents who may be under severe psychlogical stress. The mother in particular is often under considerable stress. • Parents must be povided with adequate information about the future treatment and management of their child because almost all of them have the same concerns and questions. Before surgery it is helpful to warn parents about how the child will look immediately after surgery. • In addition it is helpful for the parents and the child to attend a clinic where there are other children with similar defects and problems.
PRESURGICAL MANAGEMENT • careful management of the neonate is important for presurgical preparation. • Because feeding is a major problem, it is essential to establish a satisfactory feeding technique as soon after birth as possible. It must be remembered that these babies take longer to feed than normal childs. The mother should be encouraged to breast feed the child whenever possible. • sometimes the baby may not be able to generate adequate physiological reflexes to stimulate mother milk to flow. Bottle feeding may be difficult too because of inability to generate adequate suction. To overcome this problem, a long nipple or nipple with a flange is used. It has the effect of filling the cleft and directing the milk into the pharynx. A diagonal cross cut in the nipple prevents milk flowing unless the nipple is squeezed. Throughout bottle feeding the child should be in a semiupright position to prevent choking.
PRESURGICAL MANAGEMENT In order to cover the roof of the mouth and fill the space a feeding plate can be made. It fills the defect so that food and liquids do not enter the nasal cavity. At first an impression of the palate is taken using a specially constructed impression tray. After making a study cast the area of the defect is filled and hard acrylic plate is fabricated. The plate should be checked immediately after fitting and regurarly afterward at approximately 4 -week intervals.
PRESURGICAL MANAGEMENT In some cases a presurgical orthopaedic treatment is necessary to make surgery easier. In the infant with a unilateral cleft of lip and palate the greater and lesser segments may be malrelated: they may be widely separated or over-lapping or somewhere in between. Some surgeons consider that the surgical repair is easier to do if the segments are aligned before surgery. Presurgical orthopaedic treatment is performed by fitting either a hard or a soft acrylic plate. The plate is designed to mold the gum pads into right position and is usually supported by a headcap – alveolar molding
PRESURGICAL MANAGEMENT • In bilateral cases the premaxilla is often far forwards of the lateral segments. In theese patients the headcap may be used to apply distal traction to the protruding premaxilla. Soft acrylic plates are trimmed on the palatal surfaces to allow the segments to aline as growth takes place.
SURGICAL MANAGEMENT • Surgery usually begins at approximately 3 month of age and involves repair to the lip. The alveolar defects may also be repared at this time. • Clefts of the hard and soft palate are usually repared at about 18 months of age. • Surgical treatment is performed: 1. to improve appearance 2. to facilitate eating and drinking without nasal spillage 3. to reduce the likelihood of recurrent middle ear infections, which may lead to deafness and reduction in speech quality Some surgeons prefer to operate at an earlier age (6 -12 months) before the child develops adaptive speech habits. Others repair the soft palate at 18 months but delay the hard palate repair until further maxillary growth has taken place.
SURGICAL MANAGEMENT The correction of the cleft defect is not simply. There is a total absence of tissue in the cleft region. Closure of the defect must be made on both the oral and nasal sides with the minimum of tension. Even with the best surgical techniques available, the scar tissue that result from the repair may adversely affect the anteroposterior and transverse development of the palate and whole maxilla
SURGICAL MANAGEMENT • the upper arch is often narrow with the result that some crowding and a crossbite ( uni- or bilateral ) may be present. • The anteroposterior deficiency of the maxilla gives rise to a Class III skeletal pattern and often to a Class III incisor relationship. • The skeletal malrelationships become more severe as the child grows. • For adolescents with severe discrepancies in jaw sizes in the anteroposterior plane, major facial surgery can significantly improve the aesthetics and function
SURGICAL MANAGEMENT Repairs of the lip and palate are the two major surgical procedures. However, as the child grows other problems must be solved: • Often small or even large oronasal fistula develops. • The nose is frequently distorted and needs surgical revision. • Scar tissue in the lip gives it an uneven appearance. So the child often has to undergo secondary operations to the nose, lip or palate. This must be taken into account in planning the dental management.
ORTHODONTIC TREATMENT • The objectives of treatment are the same as those of surgery : that appearance, speech and function should be as good as the circumstances allow. • No orthodontic treatment is advised until the permanent incisor erupt. • The extent of a malocclusion is usually less apparent in the primary dentition and the level of cooperation is fairly limited. • The child should be seen at regular intervals for routine dental checks and treatment.
ORTHODONTIC TREATMENT Discrepanties in arch alignment and relationships are beginning to worsen by the mixed dentition phase. Anterior teeth are frequently malformed, hypoplastic, erupt in ectopic positions or they may even be missing. It is difficult to be sure if these problems have been caused by the cleft defect only or also by the surgical repair. At this stage should be carried out : • Correction of lingually placed permanent incisors • Supernumerary or malposed teeth may have to be removed surgically. Lateral expansion of the narrow upper arch should not be undertaken at this stage as it will not be stable.
ORTHODONTIC TREATMENT At early permanent dentition stage a full diagnosis and treatment plan must be formulated. Treatment varies according to the severity of the case. 1. Where there are reasonable arches with minimal anteroposterior and transversal discrepanties , orhtodontic treatment, ideally followed by bridgework to replace missing or malformed teeth, is indicated.
ORTHODONTIC TREATMENT 2. Where the discrepancy in arch relationship is moderate or the patient is not suitable for complex appliance treatment, it is often best to remove poorly formed and malpositioned teeth and to fit a metal denture to give a reasonable appearance without damaging the soft tissues. 3. In severe cases where orthodontic and prosthetic techniques alone will not give a satisfactory aesthetic result, surgery to improve the patient´s profile may be indicated. This will usually involve the maxilla and sometimes a combined maxillary/mandibular operation. Surgery may be preceded or followed by the orthodontic treatment and finaly restorative procedures
Speech therapy : Cleft palate patients have also speech problems, in part because the soft palate tends to be rather short and lacking in mobility, so that during the speech there is a nasal escape of air. Many also have hearing defects due to middle ear infections. Speech therapy is an important part of the total treatment.