CASES DR HIRAL THAKKAR IIND YEAR RESIDENT DEPT













 Axial proton-density–MR image shows a")

 draining the site of an")
































 is a solitary benign")







 • Fibrous dysplasia is a benign fibro-osseous developmental anomaly of")


 and may be associated")
 • Disruption of dentition • ‘ground-glass’ or")








 An expansile, lobulated lesion is present involving the metaphysis and proximal humeral")












 and fetal (B) vascular watershed, or")














 actinomycosis • is caused by rupture and surgery of")

- Slides: 101
CASES DR. HIRAL THAKKAR IIND YEAR RESIDENT DEPT. OF RADIODIAGNOSIS
CASE 1
• A 4 Year old male presented with complaint of painless neck mass. • CT Scan was performed
Cystic mass with multiple septations located anterior to the right sternocleidomastoid muscle and extending inferiorly from the level of the hyoid. There is mild displacement of right carotid and jugular vessels as well as the
Differential diagnosis: Of submandibular space lesions include • Congenital lesions – – – cystic hygromas, branchial cleft cysts, dermoid & epidermoid, thyroglossal duct cysts. lymphadenopathy – Ranula • Abscesses
DERMOID CYST • It usually manifest during the 2 nd and 3 rd decades of life with no gender predilection. • Only 7% of dermoid inclusion cysts occur in the head and neck, with the lateral eyebrow being the most common location. About 11% of dermoid cysts of the head and neck are in the floor of the mouth, the second most common location & the most common cervical location of a dermoid cyst. • Clinical signs and surgical approach are determined by the relationship of the cyst to the musculature of the floor of the mouth. • This information is crucial for optimal preoperative planning. 6
• They appear as moderately thin-walled, unilocular masses, located in the submandibular or sublingual space. • On CT scans, the central cavity is usually filled with a homogeneous, hypoattenuating (0– 18 HU) fluid material. • It may appear to be filled with "marbles, " due to the coalescence of fat into small nodules within the fluid matrix. This "sack-ofmarbles" appearance is virtually pathognomonic for a dermoid cyst in this location. • It may be heterogeneous on CT scans because of the various germinal components. Fluid-fluid levels with supernatant lipid are possible. • The rim of these cysts often enhances following administration of contrast material. 7
Axial CECT scan shows a well-defined mass in the submandibular-submental region with multiple discrete foci of hypoattenuation in the nondependent portion of the cyst. Coronal CT scan shows the mass inferior to the mylohyoid muscle (arrowheads). 8
• MR imaging depicts the topographic relationship of these cysts to the mylohyoid muscle in the floor of the mouth and helps determine the surgical approach. • The coronal plane is optimal for determining the location of the mass with respect to this muscle pair. • Dermoid cysts have variable signal intensity on T 1 -weighted images. They may be hyperintense (because of the presence of sebaceous lipid) or isointense relative to muscle on T 1 -weighted images. They are usually hyperintense on T 2 -weighted images. • The mass has a clearly demarcated rim but frequently has a heterogeneous internal appearance. 9
Coronal T 1 W 10
EPIDERMOID CYSTS • They are rare congenital lesions and are much less common than dermoid cysts in the head and neck. They appear earlier than dermoid cysts, with most lesions evident during infancy • They have fluid attenuation on CT scans and are hypointense on T 1 -weighted images and hyperintense on T 2 -weighted images, following the signal intensity of fluid. • An epidermoid cyst located entirely within the sublingual space may be difficult to distinguish from other cystic lesions in the floor of mouth (e. g. , a simple ranula) on the basis of imaging criteria alone 11
• The essential difference between a dermoid cyst and an epidermoid cyst lies in the presence of skin appendages (e. g. , sebaceous glands, hair follicles) within the wall of the dermoid cyst and the absence of these features in the epidermoid cyst. • A teratoid cyst may also contain tissue of other major organ systems (e. g. , nervous, gastrointestinal, respiratory).
TERATOID CYSTS • 5% of teratomas in newborns situated in the lateral and anterior cervical region. • CT may show a hypoattenuating, thin-walled unilocular mass. • At MR imaging, they are hypo- to isointense on T 1 -weighted images and hyperintense on T 2 weighted images. 13
Mature neck teratoma in a 9 -month-old boy. (a) Axial proton-density–MR image shows a hyperintense subcutaneous mass in the right side of the neck (arrow). (b) Coronal T 2 -weighted MR image shows multiple cysts with heterogeneous signal intensity (arrowheads). PD AXIAL IMAGE CORONAL T 2 W IMAGE 14
ABSCESS • Abscesses are usually rapidly developing and painful and may be associated with fever and leukocytosis. • Abscesses frequently involve the nodal groups draining the primary site of infection. • A third of cases of suppurative cervical lymphadenopathy are associated with pharyngitis and tonsillitis, a third with dental infection, and a third with dermatologic and otologic infection. • Imaging distinguishes the ill-defined edema of cellulitis from the coalesced and cystic abscess requiring surgery. • Abscesses frequently have thick ring-configured enhancement and may be multiloculated. Untreated infection may dissect along fascial planes. 15
Enhanced CT demonstrates confluent, necrotic submandibular lymph nodes (asterisk) draining the site of an infected dental procedure. The subcutaneous fat is infiltrated (arrow) and the airway is encroached on. 16
THYROGLOSSAL CYST • Most common congenital anomaly of the neck – 2 -4% of all neck masses • Over half present in the first decade of life but may also be seen in adults • There is an equal gender distribution, and they are usually asymptomatic. • Pyramidal lobe of the thyroid is the most common remnant of the thyroglossal tract (50% of population)
• Etiology – Represents a persistent epithelial tract during the descent of the thyroid from the foramen cecum to its final position in the anterior neck. – Normally this duct obliterates by week 10 of development. • Histologically – Well-defined cyst with an epithelial lining composed of either squamous or respiratory epithelium – There can sometimes be islands of thyroid tissue lying in the walls of the cysts – Cysts are filled with mucoid or mucopurulent material, depending on whether the cyst has been infected
• Types of thyroglossal duct cysts – Infrahyoid type • 65% and is mostly found in the paramedian position – Suprahyoid type • Nearly 20% and is positioned in the midline – Juxtahyoid cysts (15% ), Intralingual location (2%), Suprasternal variety (10% ), Intralaryngeal (Very rare ) • Clinical – Nontender and mobile masses – Infected cysts may manifest as tender masses with • Dysphagia, Dysphonia, Draining sinus, Fever, Enlarging neck mass – Often appear after an upper respiratory tract infection – Airway obstruction possible, especially with intralingual cysts – The pathognomonic sign is that the cyst moves with tongue protrusion
• Radiologic Features: • On all radiologic images, a thyroglossal duct cyst manifests as a cyst like mass either in the midline of the anterior neck at the level of the hyoid bone or within the strap muscles just off the midline. • At US, the finding of an anechoic mass with a thin outer wall in this characteristic location easily establishes the diagnosis of a thyroglossal duct cyst. However, this "classic" appearance is seen in less than half of the cases. 20
• More commonly, these cysts manifest as hypoechoic masses, often with increased through-transmission. • They may be either homogeneous or heterogeneous in appearance with variable degrees of fine to coarse internal echoes. • Heterogeneity seen in thyroglossal duct cysts on sonograms is more likely due to the proteinaceous content of the fluid secreted from the cyst wall rather than to infection. • Preoperative sonographic visualization of normal thyroid tissue is sufficient to exclude a diagnosis of ectopic thyroid tissue and obviates routine thyroid scintigraphy. 21
• On CT scans, usually appears as a smooth, wellcircumscribed mass anywhere along the vertical course of the vestigial thyroglossal duct. • The mass has a thin wall and homogeneous attenuation, the values of which correspond to those of fluid (10– 18 HU). • Elevated attenuation values of the fluid cyst reflect its increased protein content and generally correlate with a history of prior infections. • Peripheral rim enhancement is usually observed on contrast-enhanced scans. 22
• On MRI, an uncomplicated thyroglossal duct cyst has low signal intensity on T 1 -weighted images and is hyperintense on T 2 -weighted images, findings that reflect its fluid content. • The rim will be non-enhancing unless inflammation is present. • In case of infection or hemorrhage, a thick irregular rim may be visualized, and the signal intensity of the fluid becomes variable from the presence of proteinaceous debris. 23
Thyroglossal duct cyst at & above the hyoid bone. 24
Infrahyoid & paramedian thyroglossal duct cysts 25
• Complications – Infection is probably the most common complication – Local growth and invasion is extremely uncommon – Carcinoma is extremely rare • Occurs in about 1% to 2% of patients – Thyroid ectopia • Fewer than 5% of these cysts actually have ectopic thyroid tissue
2 ND BRANCHIAL CLEFT CYST • Over 90% of branchial anomalies arise from the second branchial apparatus, with a predominance of cysts. • Most second branchial cleft cysts are located in the submandibular space, at the anteromedial border of the sternocleidomastoid muscle, lateral to the carotid space, or posterior to the submandibular gland. • They appear as painless fluctuant masses adjacent to the anterior border of the sternocleidomastoid muscle at the mandibular angle. 27
• The cysts usually occur in patients between 10 and 40 years of age, but fistulas or sinuses are more commonly found during the 1 st decade of life. • There is no gender predilection. • The walls of the cysts are usually lined with stratified squamous epithelium overlying lymphoid tissue and occasionally with columnar respiratory epithelium. The intracystic fluid may contain cholesterol crystals. 28
• USG • It is seen as a sharply marginated, round to ovoid, centrally anechoic mass with a thin peripheral wall that displaces the surrounding soft tissues. • The mass is compressible and shows distinct acoustic enhancement. • Occasionally, fine, indistinct internal echoes, representing debris, may be seen. 29
• CT & MRI: • Typically well-circumscribed, homogeneously hypoattenuated masses surrounded by a uniformly thin wall, typically do not enhance. • They are hypo- to isointense on T 1 -weighted images and is hyperintense on T 2 -weighted images. • The mural thickness may increase after infection. • The "classic" location of these cysts (at either CT or MR imaging) is at the anteromedial border of the sternocleidomastoid muscle, lateral to the carotid space, and at the posterior margin of the submandibular gland. 30
• The cyst typically displaces the sternocleidomastoid muscle posteriorly or posterolaterally, pushes the vessels of the carotid space medially or posteromedially, and displaces the submandibular gland anteriorly. • Extension of the mass between the external and internal carotid arteries is very suggestive of a second branchial cleft cyst regardless of its relation to the sternocleidomastoid muscle. 31
INFECTED BRANCHIAL CYST 32
AXIAL T 1 W IMAGE AXIAL T 2 W IMAGE 33
RANULAS • They are sublingual salivary gland retention cysts and by definition arise in the sublingual space. • Simple ranulas are confined to the floor of the mouth. • Plunging ranulas dehisce either through or posterior to the mylohyoid muscle and spill into submandibular and parapharyngeal spaces. • Magnetic resonance imaging is ideally suited for characterizing floor of the mouth cystic lesions. The MRI appearance of ranulas is usually cystic; however, signal intensity varies with the protein or hemorrhagic contents of the ranula. 34
CECT shows bilobed thin walled cystic arising in the Lt sublingual space & extending into the submandibular space. 35
CYSTIC HYGROMA • It is the most common form of lymphangioma and constitutes about 5% of all benign tumors of infancy and childhood. • The majority (about 80%– 90%) are detected by the time the patient is 2 years old. No gender predilection has been reported. • In children, the most common location is the posterior cervical space, followed by the oral cavity. • They are characteristically infiltrative in nature and do not respect fascial planes. Consequently, they may extend inferiorly from the posterior cervical triangle into the axilla and mediastinum or anteriorly into the floor of the mouth and the tongue. If the mass is very large, it may extend across the midline. 36
• On US scans, most cystic hygromas manifest as a multilocular predominantly cystic mass with septa of variable thickness. • The echogenic portions of the lesion correlate with clusters of small, abnormal lymphatic channels. • Fluid-fluid levels can be observed with a characteristic echogenic, hemorrhagic component layering in the dependent portion of the lesion. 37
• On CT images, cystic hygromas tend to appear as poorly circumscribed, multiloculated, hypoattenuated masses. • They typically have characteristic homogeneous fluid attenuation. • Infected lesions commonly show higher attenuation that seen in simple fluid. • Usually, the mass is centered in the posterior triangle or in the submandibular space It is not uncommon for some of these lesions to extend from one space in the neck into another as a result of their infiltrative nature. 38
39
• MR imaging allows the best differentiation between lymphatic malformations and the surrounding soft tissues, with the former demonstrating low or intermediate signal intensity on T 1 -weighted images and hyperintensity on T 2 -weighted images. • The walls of the septa may enhance after intravenous injection of gadopentetate dimeglumine. • Infrequently, it may be hyperintense on T 1 -weighted images, a finding associated with clotted blood or high lipid (chyle) content. In the case of hemorrhage, fluid levels may be observed. 40
T 2 -w MR images and an axial fat-saturated post Gd T 1 -w image obtained show a multiloculated cystic mass in the left posterior triangle of the neck (arrow). The cysts are hyperintense on the T 2 -weighted images and demonstrate peripheral wall enhancement on the T 1 -weighted image. 41
DERMIOD CYST 2 & 3 RD decade of life On CT: central cavity with homogenous hypoattenuating fluid material with sack of marbles appearance which is pathognomonic. MRI: hyperintense but hetrogenous. ABSCESS Rapidly developing and painful lesion Ass. With fever and leucocytosis Thick ring configured enhancement and may be multiloculated EPIDERMOID CYST Rare Infant age group On CT homogeonous fluid attenuating ON MRI: hypointense on T 1 and hyperintense on T 2 THYROGLOSSAL DUCT CYST C’n location is midline 1 st decade On CT: smooth well defined circumscribed mass along the vertical course of vestigeal TGD with thin wall, homogenous fluid attenuation and peripheral rim enhancement. RANULA Seen extending into sublingual space 2 ND BRANCHIAL CLEFT CYST 3 & 4 th decade of life Classic location: anteromedial border of SCM muscle, lateral to carotid space & posterior to SM gland. On CT: homogenous hypoattenuating mass with thin wall whiach typically do not enance. CYSTIC HYGROMA Most c’n form of lymphangioma < 2 yrs of age Infilterative in nature Multilocular cystic lesion with fluid – fluid levels if there is haemorrhage
• Thus in our case Cystic mass with multiple septations located anterior to the right sternocleidomastoid muscle and extending inferiorly from the level of the hyoid. There is mild displacement of right carotid and jugular vessels as well as the trachea.
Most likely DIAGNOSIS is: CYSTIC HYGROMA
CASE 2
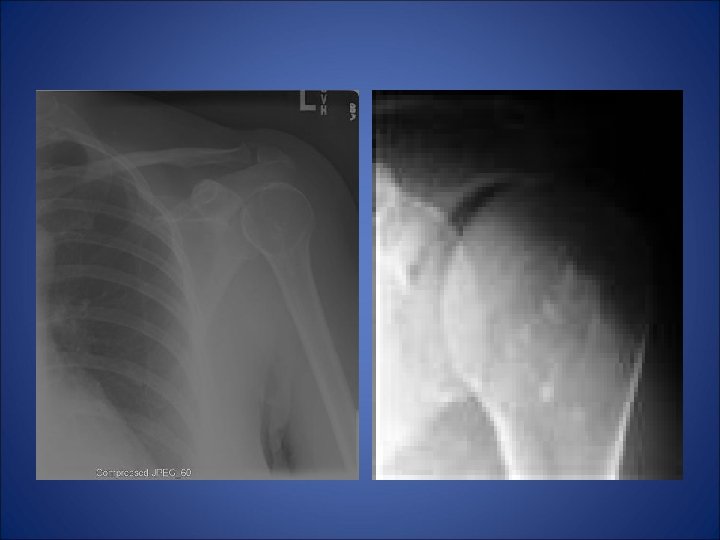
• A 26 yrs old male presented with complaint of pain in left shoulder after lifting a heavy weight. • His x-ray of left shoulder was taken which revealed…
Shows slightly expansile, septated lytic lesion is present involving the proximal 1 /3 rd of the left humerus. The margins are not sclerotic. The epiphysis appears uninvolved.
The most likely differentials would be: • Unicameral bone cyst • Aneurysmal bone cyst • Enchondroma • Fibrous dysplasia • Myxoid fibroma.
ANEURYSMAL BONE CYST • Aneurysmal bone cyst (benign bone aneurysm) is a solitary benign osteolytic lesion expanding a long bone or within a vertebra, consisting of blood-filled spaces, and separated by fibrous tissue containing multinucleated giant cells causing swelling, pain, and tenderness. • ABC predilects 5 - 20 years old individuals. • The most common locations include: Posterior elements of the spine, Clavicle, Metaphysis of long bones • There are two types of ABC’s: primary and secondary • Primary has no known cause or association with it. • Secondary type occurs in conjunction with another lesion or from trauma.
RADIOGRAPHIC APPEARANCE: Radiographs: -The classical lesion is an eccentric expanding lytic lesion in the metaphysis of a child, -aneurysmal expanded appearance of cortex is contained by periosteum & thin egg- shell covering of expanded cortex over the surface of the lesion. -Lesion rarely penetrates the articular surface or growth plate; -cyst often shows apparent trabeculation usually due to over riding of endosteal cortex. -In diaphysis, an intracortical or subperiosteal site is sometimes seen producing a superficial blister. • Spine: • radiographs demonstrate loss of pedicle of involved vertebrae and some displacement of the soft tissues by the mass; in the spine ABC’s usually involve one side of vertebral arch. posterior elements of the vertebrae are a frequent location;
• CT scan & MRI: • Demonstrates cyst within periosteal membrane no calcification of matrix with clear defination from surrounding tissues. • Look for multiple fluid - fluid levels (blood / serum); ABC has a density of about 20 hounsfield units; Bone Scan: • - shows intense uptake in the margin of the lesion, with normal background -or decreased uptake in its center;
Radiolucent lesion with expanded cortex arising in medullary canal of metaphysis of humerus -aneurysmal expanded appearance of cortex is contained by periosteum & thin shell of bone; -Marked cortical thinning and erosion and periosteal elevation
• Pathogenesis: • The most widely accepted pathogenetic mechanism of aneurysmal bone cysts involves a local circulatory disturbance leading to markedly increased venous pressure and the development of a dilated and enlarged vascular bed within the affected bone area. • Treatment • Curettage and bone grafting has a 20 -40% recurrence rate; Marginal excision or wide excision w/ bone grafting is preferable; In inaccessible areas, such as vertebrae, x-ray therapy is effective;
ENCHONDROMA • Enchondromas occur in any bone formed from cartilage and may be central, eccentric, expansile or non-expansile. • They invariably contain calcified condroid matrix, except when in phalanges. • There is no periostitis or pain • Age: c’n in 2 n and 4 th decades • Site: 50% cases affect hands and feet. And rest of them affect appendicular skeleton.
• RADIOLOGICAL FEATURES: ON PLAIN FILMS: - most enchondromas arise in the medulla of the phalanges and less often, the metacarpals. - they are eccentric, mostly solitary, well-circumscribed, round or oval lytic lesions, expanding the cortex. - although essentially lytic, flecks of calcification may be seen in the chondroid tissue, which is the differentiating point from less common benign lesions. - sometimes a purely medullary lesion consisting of wellformed circular, curvilinear or nodular calcific densities (popcorn calcification) without focal lytic areas may be present.
• MRI: • Shows characteristic features appearing on T 2 weighted MRI as hyperintense, lobulated lesions with hypointense rim and apparent septations. • Matrix mineralization is seen as punctate areas of signal void. • Enhancement of the internal septa may also be seen. • • Other less common varieties: Juxta cortical (subperiostesl, parosteal) chondroma: Multiple chondromas (Ollier’s disease) Enchondromatosis with haemangiomas (Maffucci’s syndrome)
FIBROUS DYSPLASIA (JAFFE-LICHTENSTEIN DISEASE) • Fibrous dysplasia is a benign fibro-osseous developmental anomaly of unknown origin, most common in the first two decades of life. • The prevalence is equal among males and females with a nongenetic inheritence. • There are two subtypes: monostotic and polyostotic. The radiographic and pathologic appearance of the two is nearly identical for any given lesion.
• • CLINICAL: Deformity and pain related to the involved bones Pathological fractures Hypophosphataemic osteomalacia or rickets • PATHOGENESIS: • Normal bone is replaced by abnormal fibrous tissue that contains small, abnormally arranged bony trabeculae. • It progresses until bone growth ceases, and 75% occur before the age of thirty.
• The monostotic form occurs in 75 -85% of the cases, not associated with any other anomalies, and is often asymptomatic. • The most common areas affected are the ribs, proximal femur, tibia, and craniofacial bones. Jaw lesions are discovered later. • RADIOLOGY: • Monostotic forms show a lytic lesion with thick rind like margin with ground glass density in the adjoininig bone. • On MRI lesions are hypointense on T 1 WI and either hypointense or hyperintense on T 2 WI. Internal septation, hypointense rind, cystic change and soft tissue extension may be seen. On intravenous contrast medium either uniform or septal enhancement is seen.
• The polyostotic form occurs less frequently (15 -25%) and may be associated with endocrine dysfunctions, such as precocious puberty, hyperparathyroidism, acromegaly, Cushing's syndrome, and diabetes mellitus. The association of Polyostotic FD, patchy café-au-lait skin pigmentation and sexual precocity in girls, constitutes the Mc. Cune-Albright syndrome • The disease primarily affects the lower extremities, and is predominately unilateral. Common areas include the femur, tibia, and pelvis. • RADIOLOGICAL FEATURES: • Skull often shows asymmetrical thickening of the vault with sclerosis at the base: with multiple rounded areas of radiolucency. • Obliteration of the para nasal air sinuses
• Marked facial deformity (leontiasis ossea) • Disruption of dentition • ‘ground-glass’ or radiolucent area of trabecular alteration in the long bones associated with patchy sclerosis and expansion, with cortical thinning and endosteal scalloping • Pathological fractures and deformities due to softening e. g. shepherd’s crook femoral neck. • Localized or asymmetrical overgrowth • Secondary spinal stenosis.
CHONDROMYXOID FIBROMA • This is a benign tumour and fairly rare. • The peak incidence is 20 -30 years with an equal sex incidence. • It is usually metaphyseal and eccentric within the medulla resulting in thinning and expansion of the cortex. 2/3 of cases are found around the knee, usually proximal tibia
• Radiology: • It appears an eccentric, lobulated lesion involving cortex and medulla. • A sclerotic endosteal border is characteristic. • Periosteal reaction and soft tissue extension are uncommon and calcification of matrix is seen rarely. • It may show a soap bubble or trabeculated appearance due to endosteal ridging. • Histologically: • the tissue is loose myxomatous tissue plus scattered collagen or aggregate multinuclear cells.
UNICAMERAL BONE CYST • The unicameral or simple bone is a common lytic bone lesion. • It has been suggested in the past that the lesion results from prior trauma, infection, or neoplasia. Current theories suggest that the lesion results from venous obstruction during bone growth. The fluid within simple bone cysts has a composition similar to serum. • Simple bone cysts are asymptomatic unless complications such as fracture arise. • They are usually found in young people in the first few decades of life and are more common in males (M: F 3: 1).
• The most common locations are in the metaphyseal regions of long tubular bones, especially the proximal aspects of the humerus and femur and the tibia, which account for 60 -75% of cases. • Diaphyseal involvement is uncommon and epiphyseal extension is exceedingly rare. The axial skeleton is uncommonly involved. • Simple bone cysts are very rarely multiple within the same patient. On serial radiographs the lesion may enlarge with time. • Complications of simple bone cysts include fractures, cementation with fibrous material and a change in their radiographic appearance, and possibly malignant transformation to chondrosarcoma, liposarcoma, or osteosarcoma.
• RADIOLOGY: • Plain film: Characteristic location as described above. The classic plain film location is of a centrally located, mildly expansile, lytic lesion. • Some simple bone cysts may appear multiloculated and a thin sclerotic margin is usually present. With pathologic fracture the "fallen fragment" sign is a classic. • CT: May better delineate the extent of the lesion. Reports of gas within cysts detected at CT have occurred ("pneumatocysts") with gas-fluid levels. • Tc 99 Scintigraphy: Heterogeneous increase in activity involving the proximal third of the left humerus. • MRI: (HUMERUS) An expansile, lobulated lesion is present involving the metaphysis and proximal humeral shaft. The signal is T 1 WI dark and T 2 WI bright, uniformly and there is no evidence of enhancement.
MRI: (HUMERUS) An expansile, lobulated lesion is present involving the metaphysis and proximal humeral shaft. The signal is T 1 WI dark and T 2 WI bright, uniformly and there is no evidence of enhancement.
Tc 99 Scintigraphy: Heterogeneous increase in activity involving the proximal third of the left humerus.
• Thus in our case… • Metaphyseal expansile lytic lesion which is centrally located and a multiloculated appearance not involving epiphysis without any calcification with surrounding normal bone in the proximal end of humerus in a 26 yrs old male … • Mostly likely diagnosis is • UNICAMERAL BONE CYST
CASE 3
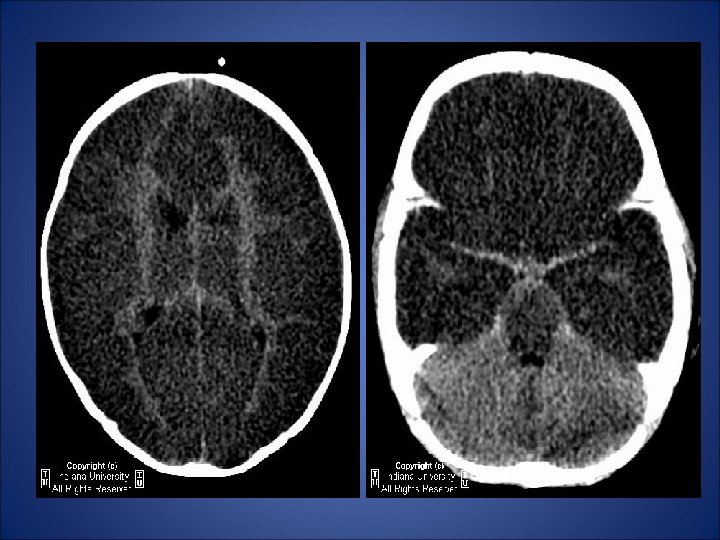
• A three month old boy in emergency room • Who survived a cardio-pulmonary arrest • NCCT scan of brain was performed …
• Reversal of the gray/white matter densities is noted diffusely, with decreased density of cerebral cortical gray matter and relatively increased density of the thalami, brainstem, and cerebellum. The ventricles appear relatively decompressed, with diffuse loss of sulcation, compatible with diffuse cerebral edema. The suprasellar cistern appears effaced, suggestive of downward transtentorial herniation.
DIAGNOSIS: DIFFUSE HYPOXIC-ISCHEMIC CEREBRAL INJURY
HYPOXIC ISCHAEMIC ENCEPHALOPATHY • Hypoxic-ischemic episodes may be caused by circulatory or respiratory arrests or inhalation of toxic substances. • The degree of severity is proportional to the severity and duration of the event as well as the susceptibility of the involved tissues to hypoxia / anoxia. • Most events are usually combinations of hypoxic and hypotensive changes. • Discrepancies between the clinical history and the severe insult should raise the possibility of non accidental trauma.
• It is the result of global rather focal brain injury. • PATHOLOGY: • Two basic patterns are seen in HIE: 1. Arterial or border zone infarcts 2. generalized cortical (pseudo laminar) necrosis.
• Ischaemic changes in HIE are concentrated primarily along the arterial border zones between the major carebral and cerebellar artery territories. • The most frequently and severely affected area is the parietooccipital region at the confluence between the ACA, MCA and PCA territories. • The basal ganglia and parasagittal areas are common sites for HIE. • In premature infants the border zone in the deep periventricular white matter and HIE manifestations are those of periventricular leukomalacia
• In generalized cortical laminar necrosis, the third, fifth and sixth cortical layers are affected. • The caudate nucleus and putamen are also often involved.
Sagittal T 1 weighted MR scan in a patient with laminar cortical necrosis following an hypoxic ischaemic episode. Subacute haemorrhage is seen in the cortex and basal ganglia.
• IMAGING: • The most common abnormality observed on NECT scans in HIE is low density band at the interface between major vascular territories. • The basal ganglia and parasagittal areas are most frequent sites. • MRI studies show border zone area hyperintensies on T 2 W 1. Enhancement after contrast administration can be striking. • Because cortical laminar necrosis is often hemorrhagic, MR scans in subacute cases may show serpentine, gyriform foci that are typically high signal on T 1 WI.
Anatomic drawings depicts location of the adult (A) and fetal (B) vascular watershed, or “border zone”, areas. In adult the watershed is peripheral and sagittal; in the fetus it lies in the deep periventricular white matter.
Hypotension with changes of hypoxic encephalopathy are demonstrated on axial CECT scans. There is selective infarction in the basal ganglia and in both parieto-occipital areas along the MCA-PCA watershed zone seen as low density foci.
• Axial and coronal post-contrast T 1 -weighted MR scans obtained 10 days after carbon monoxide inhalation show gyriform cortical and focal basal ganglionic enhancement.
• Term infants suffering profound perinatal asphyxia show a characteristic sequence of imaging findings. • Initial CT scans may be normal or minimally abnormal. • Severe generalized cerebral edema ensues over 24 to 48 hours and is seen as diffusely low density brain, often with a “reversal” sign. • Here, the cerebellum appears hyperdense compared to the abnormally low density cerebral hemispheres. • Gray-white matter differentiation is lost. • Hemorrhagic cortical necrosis with secondary calcification can often be observed within a few days after the hypoxicischaemic insult. • Severe atrophic changes are common in surviving infants.
1. Initial axial CECT scan 24 hours after delivery shows diffuse low density in the cerebral hemispheres. The cerebellum appears comparatively hyperdense, the so called- reversal sign. 2. NCCT scan after 5 days shows enlarged ventricles and low density hemispheres without gray-white matter differentiation.
NECT scan at 2 weeks following birth shows striking cortical and basal ganglionic calcifications. The lateral ventricles are enlarged, reflecting volume loss in the surrounding brain. At 1 month the calcific have largely resolved. The enlarged ventricles are surrounded by few remnants of remaining brain, seen as high density areas. Axial T 2 weighted MR scan also obtained 1 month after delivery shows the shrunken, severely encephalomalacic brain with diffuse gyriform and white matter low signal foci.
• MR scans show high signal on T 1 WI in the basal ganglia, particularly the posterior lateral lentiform nuclei and ventrolateral thalamus. • Multicystic encephalomalacia is seen in severe cases.
Key Points: • Hypoxic-ischemic cerebral injury is a major cause of morbidity in children • CT reversal sign - represents diffuse, anoxic/ischemic cerebral injury. – Diffusely decreased density of cortical gray and white matter with decreased or lost gray/white matter interface (reversal of gray/white matter densities – Relatively increased density of thalami, brainstem, and cerebellum. • Carries poor prognosis and indicates irreversible brain damage. • Particularly susceptible tissues to hypoxic-ischemia include the neocortex, basal ganglia nuclei, portions of cerebellar cortex, and brain stem. • Discrepancies between clinical history and severe insult should raise possibility of nonaccidental trauma.
Thank you…
A Forty-year old female presented with complaint of abdominal pain and sepsis-like symptoms. Clinical history reveals only that she is allergic to peanuts, and she uses an IUD for birth control. Pt had a chest X Ray which showed diffuse focal opacities. CT Scan of chest & abdomen was performed
• There are perfusion defects in the liver, primarily right lobe. Some of the defects are spherical in shape, others are more wedge shaped. There is also a linear, low-attenuation abnormality seen in the upper aspect of the liver that tracks toward the hepatic venous confluence. Myriad pulmonary nodules are present, some of which have undergone cavitation.
It can be due to: • • Neoplastic Infectious Autoimmune Toxic ingestion Most likely differentials can be; • • • Tuberculosis Muramycosis ACTINOMYCOSIS HCC of liver with lung mets Wegener’s granulomatosis
ACTINOMYCOSIS • Actinomycosis is caused by Actinomyces israelii, a gram-positive anaerobic pleomorphic small bacterium with proteolytic activity, superficially resembling the morphology of a hyphal fungus. • The organism normally inhabits the oropharynx and the GI tract. • Individuals with very poor dental hygiene and immunosuppressed patients are predisposed to infection.
Typical locations in order of decreasing frequency: • mandibulofacial • intestinal • lung Mandibulo- and cervicofacial actinomycosis is relatively common and is caused by poor oral hygiene. Clinical presentation: • draining cutaneous sinuses • "sulfur granules" (actually colonies of organisms arranged in circular fashion) 1 -2 mm in diameter in sputum or drainage • osteomyelitis of mandible (most frequent bone involved) with destruction of mandible around tooth sockets and no new-bone formation. Infection can spread into soft tissues at angle of jaw and into neck
• Abdominal ( ileocecal) actinomycosis • is caused by rupture and surgery of appendix. • Abdominal actinomycosis is also associated with IUD use with transmission through sexual activity. • Clinical Presentation: • Location: initially localized to cecum and/or appendix with fever, leukocytosis, vomiting, and pain • associated with chronic sinus tract in groin • can cause intestinal fold thickening, ulcerations, and fistula formation resembling Crohn disease, as well as rupture of abdominal viscus (usually appendix) • Abscesses in liver, retroperitoneum, psoas
• Pleuropulmonary actinomycosis • can be causd by both hematogenous spread and inhalation • Clinical presentation: • • • Lung: draining chest wall sinuses with spread via fascial planes consolidation extending across interlobar fissures cavitary abscesses pleuritis and empyema • Vertebra and ribs: • destruction of vertebra with preservation of disk • small paravertebral abscess without calcification (in distinction to tuberculosis in which disk is destroyed and often a calcified abscess is formed) • thickening of cervical vertebrae around margins • destruction and/or thickening of ribs