CASES BHUMIKA SUTHAR 3 rd YEAR RESIDENT DEPT

CASES BHUMIKA SUTHAR 3 rd YEAR RESIDENT DEPT. RADIODIAGNOSIS S. S. G. H 10/10/08

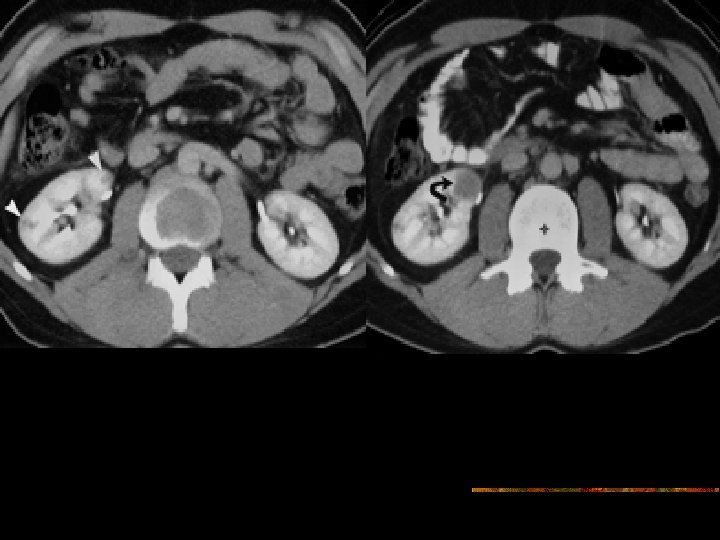
CASE 1 n A 41 -yr-old HIV-positive man presented With abdominal pain & hematuria, underwent CT scan of the abdomen.
 NCCT mid-abdomen shows a soft-tissue mass (arrowhead) in region of great vessels, a")
(a) NCCT mid-abdomen shows a soft-tissue mass (arrowhead) in region of great vessels, a finding that is suspicious for retroperitoneal adenopathy. Kid do not demonstrate any abnormality in contour(b) CECT scan of midabdomen shows bilateral soft-tissue renal masses. Note that these masses do not deform contour of kid. The paraaortic retroperitoneal adenopathy (arrowhead) is much more clearly depicted than in a.

n CT guided biopsy was suggestive of the RENAL LYMPHOMA.

n Extranodal spread of lymphoma often affects GUT, with the kidneys being the most commonly involved organs. n Unless the renal lesions manifest in the setting of widespread lymphoma, imaging-guided percutaneous biopsy is indicated to differentiate lymphoma from metastases, hypovascular RCC, uroepithelial carcinoma, with US routinely being used to guide the procedure. n Current immunohistochemical techniques allow accurate diagnosis and characterization of renal lymphoma. n Radiologists should be familiar with both typical and atypical manifestations of renal lymphoma to avoid

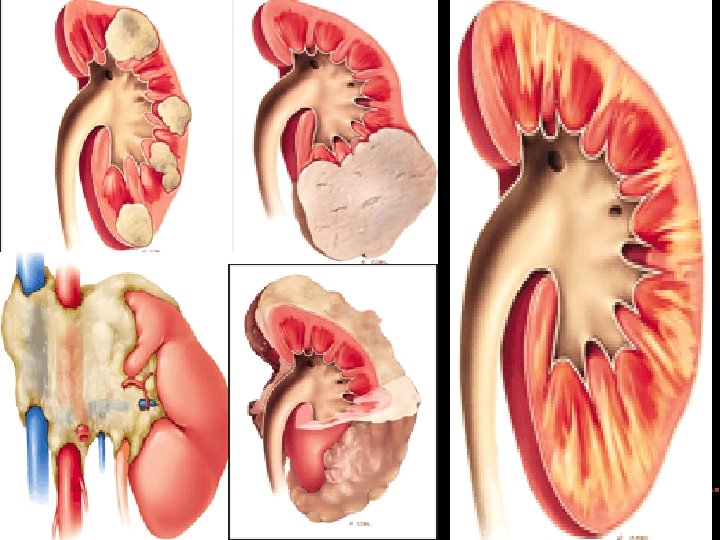
Tumor Growth and Mechanism of Spread n Hematogenous involvement --bilateral distribution of tumor foci within the renal cortex. n Tumor proliferation begins within the interstitium underlying nephrons, collecting ducts, blood vessels. n Infiltrative growth results in preservation of the parenchymal structures with preservation of renal contour. n n formation of expansile masses --As lymphomatous tumors enlarge, surrounding renal parenchyma is compressed and destroyed. n Nonuniform growth --masses extend beyond renal contour and displace collecting system, resembling primary renal neoplasms

n Clinical Details n Asymptomatic. n nonspecific signs and symptoms, including flank pain, weight loss, hematuria, or a palpable mass, back pain. n surrounds renal vascular pedicle, No vascular compromise n tumor mass can obstruct urine flow causing hydronephrosis. n occurs in widespread NHL, typically B-cell type intermediate and high-grade tumors or American Burkitt lymphoma. n no racial/sex predilection. occurs in all age groups, average age: 60 y often seen in with multisystemic, disseminated lymphoma or as tumor recurrence. n n

n Immunocompromised patients are at significantly higher risk. n Because involvement of kidneys usually indicates disseminated disease, in absence of proper clinical treatment, prognosis is poor. The disease may present with progressive renal failure. n With appropriate treatment, renal lesions may completely regress, often with minimal scarring within renal parenchyma. n Recurrence in the kidney is associated with an increased mortality rate.

RADIOLOGICAL INVESTIGATION n n n 1. Intravenous urography 2. ultrasonography 3. CT scanning & PET-CT 4. MRI 5. nuclear medicine

n Intravenous urogram obtained during the excretory phase in a 52 year-old woman with non-Hodgkin lymphoma who presented with flank pain. This image reveals a near-normal renal collecting system, with slightly enlarged kidneys and minimal narrowing of the proximal ureter that are suggestive of an external mass effect.

ULTRASOUND n Involvement of collecting system, function of kidneys, severity & F/UP of HN for guidance of percutaneous biopsy. n helpful When intravenous iodinated contrast material is CI n n SMALL LESION: may appear normal single or multiple renal masses that have low-level echoes n LARGE LESION: homogeneous hypoechoic n hydronephrosis-compression of renal hilum - by LN or obstruction of ureters. n perirenal hypoechoic halo -characteristic of perirenal lymphoma n d/d large lesions from a simple /complicated cyst is difficult. Color/power Doppler -displacement of N renal vessels, little vascularity within lesions. n

Sagittal sonogram in a 15 -yr-old male adolescent with NHL shows nearnormal architecture of the left kidney. Both kidneys were normal and no indication of HN was noted. Axial sonogram in a 22 -year-old woman with known lymphoma depicts a large kidney with heterogeneous echotexture and poorly defined areas of hypoechogenicity. A mild degree of HN is noted.

a 62 -yr man who presented with palpable flank masses demonstrates perirenal lymphoma without retroperitoneal adenopathy. kid shows no a mass or HN, a hypoechoic but solidappearing area surrounds kidney. USG - represent a perirenal complicated fluid collection or edema; perirenal lymphoma should be considered. Because of underlying renal disease, echotexture is increased throughout the kidney.

Computed Tomography n Imaging modality of choice for diagnosis, staging, monitoring, to determine response to therapy n depicts the renal lesions, extension to adjacent anatomic structures such as perirenal space , retroperitoneum, determine systemic spread of disease. n Nephrographic (venous) phase of CE - detection of subtle /small lesions, particularly in medullary portion of kidney. n Lymphomatous deposits are hypovascular, enhance poorly. n small masses that do not deform renal contour can be mistaken for unenhanced normal medulla and are less conspicuous on early images obtained in CM phase of enhancement. n CM phase - optimal depiction of renal vessels, is imp. for d/d renal lymphoma from hypervascular primary renal tumors.

n If the tumor is central & affects hilar region or collecting system appears to be involved, excretory phase imaging is necessary. n evaluation of perirenal lymphoma, which can be indistinguishable from the underlying kidney or mistaken for a large primary renal mass on unenhanced images. n low-attenuating perirenal masses or nodules almost always represent renal lymphoma. n CECT - lesions have attenuation values higher than those of simple fluid.

Positron Emission Tomography n Emerged as a very useful technique for the staging of lymphomas and the detection of recurrent disease. n detect increased metabolic activity within lymphomatous deposits. n more sensitive and specific than conventional anatomic imaging in detecting additional small tumor deposits. n Combined PET-CT is emerging as a powerful tool that demonstrates the metabolic activity of tumors as well as anatomic details, a combination that allows precise localization and potential earlier detection of additional tumor foci

MRI n particularly useful When intravenous iodinated contrast is CI. n lymphoma displays low signal intensity on T 1 -WMRI. n isointense or moderately hyperintense on T 2 -W images. n Lymphomatous tissue may be minimally enhancing, but it does not enhance as much as normal renal parenchyma. n superior to CT in depicting involvement of the bone marrow
 shows a large heterogeneous left renal mass. Following IV")
T 1 -WGRE image (FLASH) shows a large heterogeneous left renal mass. Following IV Gd, the mass shows heterogeneous CE that is less than that of renal parenchyma.

NUCLEAR MEDICINE n gallium-67 citrate- higher degree of specificity in detection of lymphomatous infiltration of kidneys- used for diagnosing and staging lymphoma. n gallium is taken up by lymphomatous tissue in the kidneys, and it is also concentrated in inflammatory masses of the kidney. Therefore clinical history of patients is important. n FDG PET scanning has very high but not absolute specificity for malignant lymphoma. It has been reported that increased FDG uptake may also be observed without active disease. n 99 Tc-labeled antibody - advocated in imaging and staging lymphomas.

n Gallium scan in a 55 -yr F with known diffuse, poorly differentiated lymphoma. A sonogram revealed no HN. the echotexture of the kidneys was abnormal on th. USG, posterior view of kidneys (Post) obtained at 72 hours after injection of gallium-67 citrate shows multiple abnormal areas of increased uptake (arrows), particularly on right side (R). finding is consistent with renal involvement by lymphoma. Urinalysis results were normal, excluding underlying infection.

ANGIOGRAPHY n lymphoma is a hypovascular neoplasm; therefore, angiography cannot help in the diagnosis or staging of lymphomatous tumors. n with CECT scanning, lesions remain hypovascular compared with the renal parenchyma when the contrast material is delivered to the kidney, via either intravenous injection for CT scanning or direct arterial injection for angiography.

INTERVENTION n When a single mass with atypical imaging features is noted in a kidney, biopsy may occasionally be attempted to differentiate renal lymphoma from a primary renal cell carcinoma. n n biopsy is performed because treatments for the 2 neoplasms differ completely. In addition, in patients with another known primary malignancy, biopsy is often needed to differentiate metastasis to the kidney from renal infiltration by lymphoma. n Fine-needle aspiration with adjuvant flow cytometry is a useful technique for diagnosing and subtyping lymphomas. n Patients with renal lymphoma are treated with chemotherapy, and surgical intervention is not indicated. The lesions are treated with systemic chemotherapy, and the response is usually favorable. The tumors often completely respond to such treatment without residual disease in the kidneys.

Imaging Patterns n Renal lymphoma has a variety of CT appearances--- n Multiple masses Solitary mass Contiguous retroperitoneal extension Perirenal disease Infiltrative growth The renal sinus and collecting system are less frequently affected, except for obstruction caused by retroperitoneal adenopathy. n n n
 is that of multiple parenchymal")
1. Multiple Lesions n n M/C patternof renal lymphoma(60%) is that of multiple parenchymal masses of variable size, 1– 4. 5 cm in diameter. BIL>UNIL n NCCT: as soft-tissue lesions with slightly higher attenuation that of the surrounding parenchyma. Calcifications - rare. n Nephrographic phase CECT is essential because many lesions are small and affect medullary portion of kidneys, with relatively little cortical deformity. n Lymphomatous deposits enhance less than N renal tissue, appear as relatively homogeneous masses. n Heterogeneous/ cystic appearance is rarely seen and is typically a sign of tumor necrosis - undergoing chemotherapy. n Large lesions tend to be more heterogeneous. The presence of retroperitoneal adenopathy is an additional clue to diagnosis.
Transverse")
B-cell lymphoma in a 33 -yr-old man with progressive weakness of upper extremities. (a)Transverse US image of rit kidney shows multiple hypoechoic soft-tissue masses in parenchyma. Note that normal shape of kidney is preserved. Similar hypoechoic masses were seen in lt kidney(b)Sagittal color Doppler US image of rit kidney shows displacement of renal vessels by the masses.

D/D Multiple renal masses n Renal metastasis- lung cancer is the most common primary malignancy to spread to kidneys, followed by breast cancer, gastric cancer, and melanoma- usually clinically silent and detected incidentally with disseminated tumor. If no relevant clinical history, imaging-guided biopsy is indicated. n Multiple synchronous renal cell carcinomas are differentiated on the basis of their hypervascular enhancement pattern n Renal abscess n Acute pyelonephritis, n septic emboli to the kidneys n renal infarcts

2. Solitary Lesion - 10%– 25% n D/D: RCC, METASTASIS n US: LYMPHOMA- Hypoechoic, maintain renal contour, RCC tends to appear more echogenic/heterogenous. n CECT: renal lymphoma- Homogeneous & little CERCC-which enhances in arterial phase. n n some atypical RCC such as papillary and chromophobe variants, do not exhibit classic enhancement. n percutaneous biopsy is required for definitive diagnosis to exclude an atypical RCC or a solitary metastasis. n Associated thrombus in RV/ IVC is highly Suggestive of RCC. n H/O primary malignancy is essential for diagnosis of mets.
 CMphase CECT scan shows")
Papillary RCC mimicking lymphoma in a 57 -yr -old F(a) CMphase CECT scan shows a solitary hypovascular mass (arrow) in left kidney, (b) On an early excretory phase CECT scan, mass (arrow) remains hypoattenuating relative to renal parenchyma, despite minimal heterogeneous enhancement within mass. (c) On a sagittal US image of left kidney obtained at time of biopsy, mass (cursors) is mildly echogenic. finding would be atypical for lymphoma, which is generally hypoechoic.

3. cystic appearance n highly unusual n may contain large lowattenuation areas, related to necrosis, particularly during chemotherapy. n markedly hypoechoic at US and even exhibit some degree of enhanced through transmission, thereby mimicking a cystic mass Transverse US image of left kidney shows a complex, partially cystic renal mass (arrow). thick wall, multiple septa, and minimal through transmission (arrowheads).

Recurrent large B-cell lymphoma in a 61 -year-old man who had been treated with high-dose chemotherapy. (a) Venous phase contrast-enhanced CT scan shows a low-attenuation mass (arrow) in left kidney. The lesion has thick walls, there is stranding as well as subtle nodular thickening in perinephric space (arrowhead).

4. Direct Extension from Retroperitoneal Adenopathy n Contiguous extension to kidneys or perinephric space from large retroperitoneal masses is second M/C pattern (25%– 30% of cases). n usually have widespread disease with bulky tumors, many are immunocompromised. n At imaging, large retroperitoneal masses are seen invading or displacing adjacent kidney, envelops renal vasculature and invades the renal hilum. n usually demonstrate homogeneous attenuation n HN - entrapment of the ureters is common occlusion or thrombosis of major renal Vessels is rare. n
")
Burkitt lymphoma affecting retroperitoneal nodes, adrenal glands, kidneys in a 46 -yrold man (a) Sagittal US image - a large hypoechoic mass (arrows) displacing and infiltrating left kidney - mild left HN (arrowheads)(b) Trans. color Doppler US image shows mass encasing L renal Vessels. subtle hypoechoic masses - seen in Rt kid.

Burkitt lymphoma affecting the retroperitoneal nodes, adrenal glands, kidneys in a 46 year-old man.

5. Perinephric Disease n usually the result of direct extension from retroperitoneal disease or transcapsular spread of renal parenchymal disease. n isolated perinephric lymphoma is unusual (<10% of cases)disease can completely surround kidney without parenchymal compression or functional impairment-[virtually pathognomonic]. n US- Perirenal hypoechoic tissue of variable thickness. n CECT are invaluable for demonstrating a rind of homogeneous perinephric soft tissue may compressing normal parenchyma without causing significant impairment of renal function. n In less dramatic cases, findings are limited to thickening of the Gerota fascia or plaques and nodules in the perirenal space.
 NCCT -")
Perinephric disease in a 66 -y-old man with a left renal mass(a) NCCT - marked enlargement of L kidney. Left paraaortic lymph nodes (arrowhead) = encasing left renal vein (b) CM phase CECT scan shows a large hypovascular mass (arrows) located primarily in perinephric space. Note that there is no significant enhancement delay in L renal parenchyma relative to R kidney. Arrowhead indicates paraaortic lymph nodes encasing left renal vein (c) Sagittal US image obtained at time of biopsy shows a hypoechoic mass (arrows) surrounding and partially invading L kidney

n d/d: Perirenal involvement --- n direct extension from primary RCC/ metastasis from primary can. of lung/breast/from melanoma Inflammatory & nonneoplastic urinomas, pancreatitis, retroperitoneal fibrosis n n Secondary features and clinical history can usually help differentiate perirenal lymphoma from other entities. n Extensive, bulky adenopathy is a hallmark of lymphoma and often involves the kidneys by contiguous extension n large nodes can be seen with other tumors, most often metastatic adenocarcinoma from prostate, colon, unknown site. Adenocarcinomatous nodes - "hard, Discrete, obstruct renal vasculature, "softer", homogeneous conglomerate mass lymphomatous nodes encase and surround vasculature but do not typically result in occlusion. n n

6. Renal sinus infiltration, n Lymphoma can preferentially affect the renal sinus, although this is an uncommon occurrence. n At US, renal sinus lymphoma appears as a hypoechoic mass infiltrating the renal sinus. This type of lymphoma may be difficult to differentiate from heterogeneous renal sinus fat, since both conditions tend to have poorly defined borders and traversing hilar vessels. n n At CT, Vascular encasement is common; because of the pliable nature of the tumor, however, resulting hydronephrosis is often mild.
 CECT scan of shows a homogeneous")
B-cell lymphoma in a 70 -Yr F (a) CECT scan of shows a homogeneous soft-tissue mass in L renal sinus. Note lack of HN and presence of mesenteric and retroperitoneal adenopathy as well as splenomegaly (b) Sagittal US image of L kid shows a poorly defined in-filtrating mass in region of renal pelvis (c) color Doppler US, kidney is well vascularized and mass is hypovascular. diagnosis was established with US-guided biopsy of the mass.

7. Nephromegaly-Infiltrative Disease n Nephromegaly without distortion of normal shape of kidneys results from diffuse infiltration of renal interstitium by malignant lymphocytes. This appearance is more common in Burkitt lymphoma, either disseminated or limited to kidneys (primary renal lymphoma). n Diffuse infiltration is almost always bilateral n US - quite subtle and include globular enlargement of kidneys with heterogeneous echotexture of parenchyma and loss of normal echogenic appearance of renal sinus fat. n CECT - heterogeneous CE of kid, loss of CM differentiation in corticomedullary phase, infiltration of the renal sinus fat. n collecting system – encased, stretched rather than displaced. n Occasionally, lymphoma infiltrates & destroys renal parenchyma extensively and manifests as a large, nonfunctioning kidney.

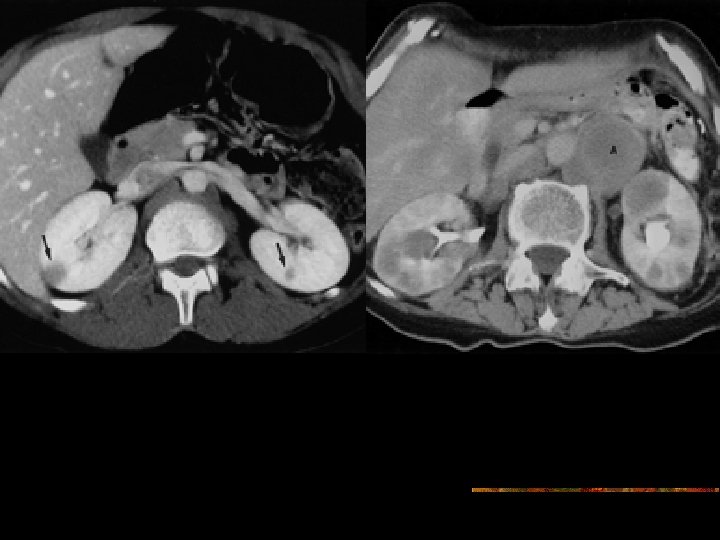
Primary renal lymphoma in a 41 -year-old HIV-positive man who presented with renal failure. Nephrographic phase CECT scan of kidneys shows bilateral renal enlargement. Heterogeneously decreased enhancement of renal parenchyma is also seen. The diagnosis of Burkitt-like lymphoma was established with renal biopsy.
")
TCC infiltrating right kidney in a 44 -yr-old man with right flank pain. (a) CM phase shows a mass (arrow) infiltrating right kidney. delayed right renal enhancement and paracaval adenopathy. (b) Sagittal US image of left kid shows a heterogeneous mass infiltrating renal parenchyma and sinus fat at upper pole. Note also the absence of hydronephrosis.

n d/d: An infiltrative growth pattern – n transitional cell carcinomas demonstrate expansile growth when they are confined to the renal collecting system; however, they can demonstrate an infiltrative growth pattern with parenchymal renal invasion n n inflammatory processes such as acute pyelonephritis or xanthogranulomatous pyelonephritis

Atypical CT Patterns in Renal Lymphoma n spontaneous hemorrhage necrosis heterogeneous attenuation cystic transformation calcification n often the result of prior treatment. n However, most lymphomatous kidney masses and nodules disappear following therapy, and the kidney resumes a normal CT appearance. n n

Lymphoma in Immunocompromised Pts n Increased prevalence of lymphoma has been described in immunocompromised patients e. g. with HIV infection, in immunosuppressed organ transplant recipients, common With cyclosporine therapy n immunodeficiency-related lymphoma often has an extranodal origin, with CNS, bone marrow, GIT, lung, heart, liver being the most common sites. n Patterns of renal involvement are similar to those seen in malignant lymphoma in the general population. n differentiation of lymphomatous involvement from infection can be difficult in immunocompromised, biopsy is sometimes needed for definitive diagnosis.


Case 2 n 65 -year-old man with right upper quadrant pain and features of obstructive jaundice underwent 3 D volume-rendered CT scan

65 -year-old man with right upper quadrant pain. 3 D volume-rendered CT scan in coronal projection reveals intrahepatic ductal dilatation (arrows). Gallbladder is also distended. Calcified stone (arrowhead) is identified in cystic duct. Axial CECT scan also reveals stone (arrow) in cystic duct, characteristic of Mirizzi's syndrome.

n MIRIZZI SYNDROME: n In 1948, P. L. Mirizzi described an unusual presentation of gallstones that, when lodged in either the cystic duct or the Hartmann pouch of the gallbladder, externally compressed the CHD, causing symptoms of obstructive jaundice. n A low insertion of the cystic duct into the CHD is a predisposing factor in the development of Mirizzi syndrome. In patients with a low insertion of the cystic duct, the ducts run parallel to each other. The CHD is at increased risk of compression by impacted calculi within the cystic duct
 in the Hartmann")
Pathophysiology n Impaction of a large gallstone (or multiple small gallstones) in the Hartmann pouch or cystic duct results in the Mirizzi syndrome in 2 ways: (1) chronic and/or acute inflammatory changes lead to contraction of the gallbladder, which then fuses with and causes secondary stenosis of the CHD, or (2) large impacted stones lead to cholecystocholedochal fistula formation secondary to direct pressure necrosis of the adjacent duct walls. n a 2 -stage classification based on the results of ERCP and PTC. -further subclassified into the following groups Type I - No fistula present n n n Type IA - Presence of the cystic duct Type IB - Obliteration of the cystic duct Types II-IV - Fistula present n n n Type II - Defect smaller than 33% of the CBD diameter Type III - Defect 33 -66% of the CBD diameter Type IV - Defect larger than 66% of the CBD diameter

type 1 Mirizzi syndrome. Panel A: An impacted stone in cystic duct or Hartmann's pouch of gallbladder obstructs CHD both by extrinsic compression and associated inflammation. Panel B: Treatment consists of cholecystectomy. type II Mirizzi syndrome. A) Protrusion of an impacted stone from the cystic duct into the CHD results in a cholecystocholedochal fistula. B) treatment of choice is partial cholecystectomy and cholecystocholedochoduodenostomy

C/F n no consistent or unique clinical features that distinguish it from other more common forms of obstructive jaundice. n recurrent cholangitis, jaundice, right upper quadrant pain, abnormal hepatic serum biochemical findings n Acute presentations include pancreatitis and cholecystitis; in a patient with persistent jaundice and a right upper quadrant mass, the presence of carcinoma may be mistakenly inferred. n an increased coincidence of GB carcinoma & Mirizzi syndrome. Generally, distinguishing between Mirizzi syndrome and other causes of obstructive jaundice is not possible with physical examination alone. Radiologic studies are required. n USG is a first-line diagnostic examination. CT may also be used. n

Differential diagnosis n n n Biliary atresia Cholangiocarcinoma Cholelithiasis
 impacted calculus in Hartmann pouch or cystic duct")
ULTRASOUND n Ultrasonographic findings n (1) impacted calculus in Hartmann pouch or cystic duct (2) dilatation of the CHD above level of the impacted stone (3) narrowing of the CHD at level of impaction n. Mirizzi (4) normal caliber of CBD below the impaction. syndrome mimicking a Klatskin tumor. (a) Sagittal US scan through porta hepatis shows a large gallstone (S) in region of CBD and common hepatic duct dilating the latter (cd).

plain Radiograph n not useful in diagnosing Mirizzi syndrome. n may shows radiopaque gallstones that contain sufficient amounts of calcium.
 dilatation")
CT SCAN n Typical diagnostic findings of Mirizzi syndrome on CT n (1) dilatation of the biliary system, including the CHD, distal to the level of the gallbladder neck (2) an impacted calculus in the neck of the gallbladder; (3) a contracted gallbladder; (4) a normal diameter of the CBD below the level of the stone n n nonspecific Signs of cholecystitis or pericholecystitis may also be present. n Some authors maintain that CT should be used primarily to exclude malignancies—namely, liver metastases invading the biliary system and carcinoma of the porta hepatis—from the differential diagnosis
 Axial CT scan of abdomen shows")
Mirizzi syndrome in a 66 -year-old man (a) Axial CT scan of abdomen shows dilated intrahepatic bile ducts (arrowheads). (b) Axial CT scan of abdomen shows a 2. 2 -cm cystic duct stone with a calcified rim (arrow) overlying the location of the extrahepatic bile duct and resulting in biliary dilatation.

n ERCP n direct cholangiography in any patient with suspected Mirizzi syndrome after the initial evaluation with ultrasonography and/or CT. n ERCP is probably the criterion standard, and it is also useful in temporarily relieving stenosis of the CHD by means of stent placement. n PTC may also be used for diagnosis, especially if ERCP findings fail to help. n Common signs include (1) visible calculus in the expected position of the cystic duct (2) smooth, lateral, and extrinsically compressed CHD n n

npt presented with acute cholecystitis, as confirmed at imaging, pain resolved over a few days, but mildly elevated bilirubin levels persisted. ERCP shows smooth narrowing of bile duct (arrow) at site of insertion of cystic duct (Mirizzi syndrome). Note the small calculus in the cystic duct.

MRCP n n n n high sensitivity and specificity in the detection of gallstone and bile duct stenosis. Typical MRCP findings of Mirizzi syndrome include (1) an impacted stone in the gallbladder neck, a gallstone in the cystic duct, (2) compression of the common hepatic duct, (3) dilatation of the biliary system above the level of impaction (4) a contracted gallbladder with wall-thickening. Additional sequences should be used to exclude the presence of malignancy.
 Coronal MRCP 1. 2 -cm calculus")
Mirizzi syndrome in a 46 -year-old woman. (a) Coronal MRCP 1. 2 -cm calculus (arrow) resulting in biliary dilatation. Gallbladder calculi are also noted (arrowheads). (b) Coronal MRCP obtained 5 mm anterior to a shows two calculi (arrowheads) in the dilated cystic duct, which parallels the extrahepatic bile duct. inferior calculus corresponds to the ductal calculus seen in a. This calculus eroded through wall of the cystic duct into the extrahepatic bile duct, bridging the two structures and resulting in compression and obstruction of the common hepatic duct(c) ERCP image demonstrates a calculus in cystic duct (arrowhead) as well as larger, more inferior calculus (arrow) resulting in obstruction of bile duct (bd).
 scintigraphy is useful in diagnosing")
NUCLEAR MEDICINE n hepatobiliary iminodiacetic acid–diisopropyl iminodiacetic acid (HIDA-DISIDA) scintigraphy is useful in diagnosing Mirizzi syndrome. n 3 highly sensitive and specific signs noted are (1) a nonvisualized gallbladder (2) moderate dilatation of the CHD (3) delayed excretion into the duodenum n n
 in 61 -yrold man with right upper")
n Cholescintigrap hy (1 -h initial images) in 61 -yrold man with right upper quadrant pain for 2 days. Note nonvisualization of gallbladder and small bowel activity. Lower activity is within urinary bladder
 of the same patient as")
Cholescintigraphy (3 -h delayed images in the anterior projection) of the same patient as in Image 2. Note persistent nonvisualization of the gallbladder and minimal activity within the small bowel.

INTERVENTION n treatment of choice for Mirizzi syndrome is surgical n electrohydraulic lithotripsy - only complication was a perforation that was treated conservatively. When surgical treatment is used, the technique depends on the classification of the patient's Mirizzi syndrome, which occasionally is not discovered until the procedure has begun. n preoperative cholangiography - to determine if CD is present and to ensure that CBD is free from calculi. any stones in cystic duct should then be manipulated back into GB. GB should be incised at its fundus n type I (compression without a fistula) - treated as minimally as possible. partial cholecystectomy, leaves neck of GB in place. n types II-IV (ie, fistula present) require more complex interventions. with either cholecystectomy and closure around a T-tube or partial cholecystectomy with in situ T-tube placement

CASE 3 n 23 yr old female with a 6 month history of headache without any neurological deficit.

Densely enhancing linear structure coursing frontal horn of Rt lateral ventricle to the inner table.

Arterial angiogram is normal Venous phase shows multiple draining veins in the frontal region with small vessels draining into the venous structure

Diagnosis n Venous Angioma

Discussion n M/C type of angiomas & are composed of radially arranged anomolous veins that converge on centrally located dilated transcortical venous trunk. n This trunk courses transcerebally or transcerebrally to terminate in a cortical vein, dural venous sinus or deep venous sysyem. n No arterial component are seen to the lesions & veins are separated by normal neural tissue. n Cerebellar angiomas have more propensity to bleed than supratentorial lesions & should be included in the D/D of cerebellar bleed [ Third only to HT & AVM ] n most commonly supratentorial ( Frontal lobe ) & IInd most common location is cerebelum.

n NCCT – Normal n CECT – Tuft of vessels near ventricle with dilated draining vein n Angio – Caput Medusa appearance with enlarged draining vein n MRI -Tubular or stellate vessels without any mass effect or oedema unless complicated by Hge.

Venous angioma. Post Gd T 1 W image demonstrates a focus of linear enhancement in right frontal region with typical appearance of central dilated vein & associated dilated medullary veins.

Venous angioma Linear flow void in Rt cerebellar hemisphere Angio – Large vein draining the cerebellar hemisphere

n Cavernous angiomas : - No normal brain in lesion. It is n Location – Frontal & temporal lobes – M/C- Deep cerebral white matter, CM junction & basal ganglia - common supratentorial locations- Pons & posterior fossa- common posterior fossa locations. n Age – 20 – 40 yrs n Angio – Normal NCCT – Iso / Hyperdense, calcification CECT – Minimal or no enhancement, No edema or mass effect. MRI – Mixed signal with hemosiderin / ferritin rim {Popcorn like} - Multiple lesions in 50 % - T 2 WI & GRE–Low SI rim becomes prominent (Blooms) Extraaxial cavernous angiomas – Resemble meningiomas & are of hyperintense SI on T 2 & show strong homogenous enhancement after contrast. n n lobulated collection of dilated endothelial lined spaces.

NCCT CECT Cavernous Angioma T 1

T 2 GRASS Blooming of the lesion on GRE images

THANK YOU
- Slides: 79