CASES BHUMIKA SUTHAR FIRST YEAR RESIDENT SSGH BARODA

CASES BHUMIKA SUTHAR FIRST YEAR RESIDENT SSGH BARODA

Case - 1 l A young boy of 11 years presented with c/o wrist pain WITHOUT any significant soft tissue swelling.




Radiographic Findings: Wrist Films: l Lobulated lytic lesion of the distal radius abutting the articular surface and extending from the epiphysis into the proximal metaphysis. l matrix calcification are seen. MR: l The lesion demonstrates low signal on T 1 weighted images and high signal on T 2 weighted images with rings and arcs compatible with chondroid matrix. l No extra-osseousoft tissue mass is seen.

Diagnosis l Chondroblastoma

PAEDIATRIC EPIHYSEAL LYTIC BONE LESIONS l l CHONDROBLASTOMA GCT BRODIE’S ABSCESS FIBROUS DYSPLASIA

CHONDROBLASTOMA l Age : 5 -25 years l monostotic. COMMON SITES: long bones - femur, humerus, tibia. Arise in an epiphysis May extend into the metaphysis. l l A thin sclerotic rim may separate the tumor from the adjacent normal bone. l Matrix mineralization (60%) typically punctate and less commonly in a pattern of rings and arcs. Periostitis, Soft tissue masses, pathologic fractures are rare. l

Tibia epiphyseal, rounded lytic lesion presenting well defined, regular margins, without surrounding sclerosis with central gross calcification.

Lucent area with well-defined margins in region of epiphysischondroblatoma in 11 yrs old boy Coronal reconstructed ct Coronal t 1 confirmsmetaphyseal weighted extension

PAEDIATRIC EPIHYSEAL BONE LESIONS l l CHONDROBLASTOMA GCT BRODIE’S ABSCESS FIBROUS DYSPLASIA

GCT

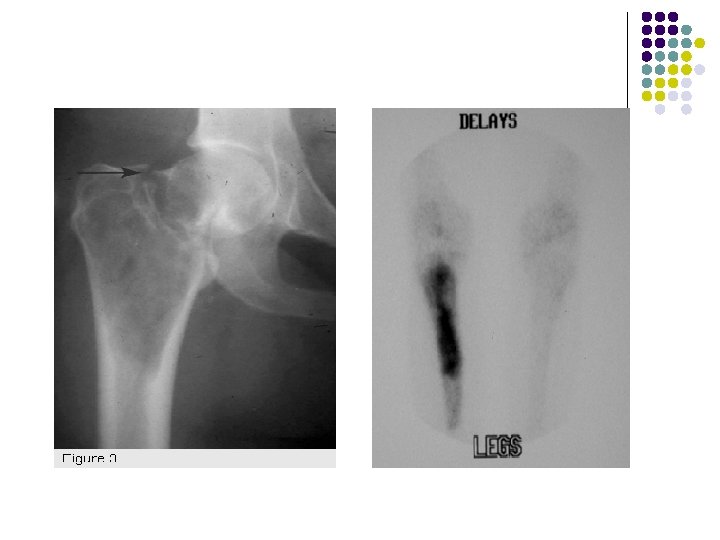
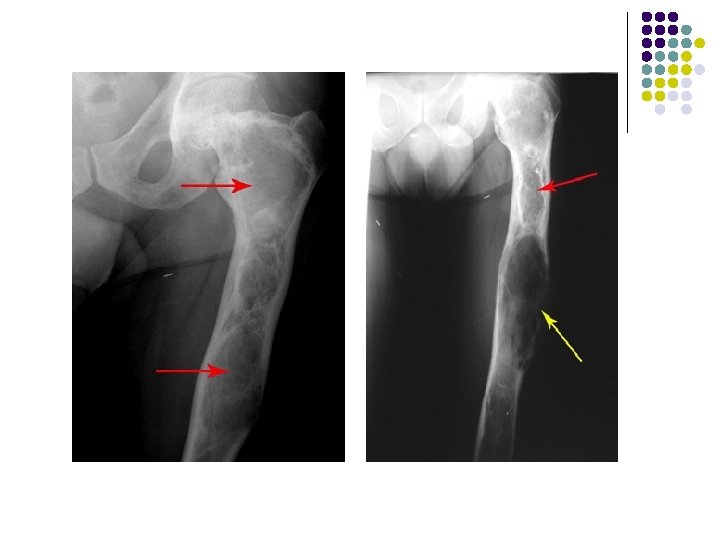
PLAIN RADIOGRAPH l l l l Expansile , Solitary lytic bone lesion Closed epiphyses No reactive sclerosis /No periosteal reaction May break through cortex with cortical thinning Soft-tissue invasion (25%) Pathologic fracture (5%) May cross joint space in long bones (exceedingly rare)

AP radiograph of the left wrist shows an expanded solitary lytic lesion involving closed epiphyses subarticular position of the distal ulna without rim of sclerosis or periosteal reaction which is typical for a giant cell tumor

Giant cell tumor of distal radius is eccentric and extend to the end of the bone
 l")
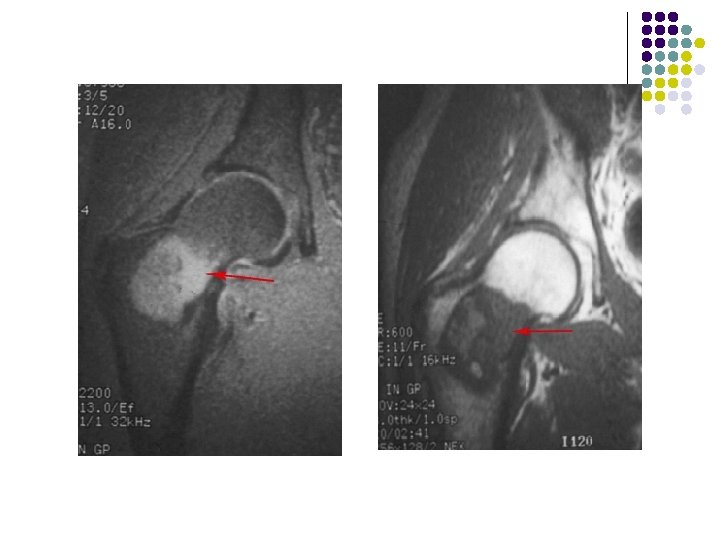
CT: l Tumor has soft-tissue attenuation (May contain foci of low attenuation (hemorrhage/necrosis) l Well-defined margins WITHOUT rim of sclerosis MRI l Heterogeneous signal intensity with low to intermediate intensity on T 1 WI & T 2 WI due to collagen and hemosiderin content.

Axial ct of proximal leg-Soft tissue attenuation with well defined margins and foci of low attenuation within due to h’age or necrosis. Coronal CT scan of a giant cell tumor of the distal ulna show soft tissue attenating lesion.

T 2 -weighted coronal MRIs of the wrist show a giant cell tumor located in a subarticular position in the distal radius. The lesion is heterogeneous and hyperintense.

NUCLEAR MEDICINE IMAGING l Diffusely increased uptake l May have "doughnut" sign of central photopenia (cold lesions with increased uptake around the rim) ANGIOGRAPHY: Hypervascular lesion

Bone scintigraphy shows hyperconcentration of tradiotracer in diastal radius due to GCT

PAEDIATRIC EPIHYSEAL BONE LESIONS l l CHONDROBLASTOMA GCT BRODIE’S ABSCESS FIBROUS DYSPLASIA

BRODIE’S ABSCESS

RADIOGRAPHIC APPEARANCE l l l Well demarcated Geographic lucency beneath epiphyseal plate. A channel extending to the growth plate is almost diagnostic for infection. No bone destruction/periosteal reaction Early-soft tissue swelling Late: irregular bone destruction On occasion, the lesion appears to become tethered to the growth plate and cavity progressively elongates with growth extending from the epiphysis into the diaphysis in snakelike fashion (the serpentine sign)

l AP and lateral radiographs of the distal tibia depicting an eccentrically located radiolucent lesion crossing the epiphyseal plate


SERPENTINE SIGN

Sagittal T 1 -weighted image of the left ankle depicts a well-defined lesion of decreased signal intensity in the anterior aspect of the distal tibial metaphysis, which extends into the adjacent growth plate and epiphysis.


PAEDIATRIC EPIHYSEAL BONE LESIONS l l CHONDROBLASTOMA GCT BRODIE’S ABSCESS FIBROUS DYSPLASIA

l FIBROUS DYSPLASIA

X-rays: l l An abnormal area of bone that typically has an appearance similar to that of "ground glass. " There frequently is expansion of the involved area of bone. May be deformity of the bone that is usually seen as bowing. CT scan: l see fractures and determine the weakness of the bone. MRI: l l show the involved area of bone may be helpful to determine whether or not areas have become cancerous. BONE SCAN: l A "hot spot" in the areas of involved bone.

PAEDIATRIC EPIHYSEAL BONE LESIONS CHONDROBLASTOMA <30 YRS OPEN EPIPHYSES THIN SCLEROTIC RIM MATRIX MINERALISATION MRI: LOW TO HIGH BRODIE’S ABSCESS Geographic lucency Beneath epiphyseal plate C/F Soft tissue swelling Irregular bone destruction GCT • CLOSED EPIHYSES • ABUT ARTICULAR SURFACE • NON SCLEROTIC MARGIN • SHARPLY DEFINED ZONE OF TRANSITION • ECCENTRIC • MRI: HETEROGENOUS FD Ground glass appearance Bone expansion Bone deformity fractures

CASE 2 l A 17 YEARS OLD FEMALE PRESENTED WITH PAINLESS ANTERIOR MIDLINE NECK MASS. O/E: l Swelling moves on deglutition and on protrusion of tongue.
 shows a cystic anechoic structure just below")
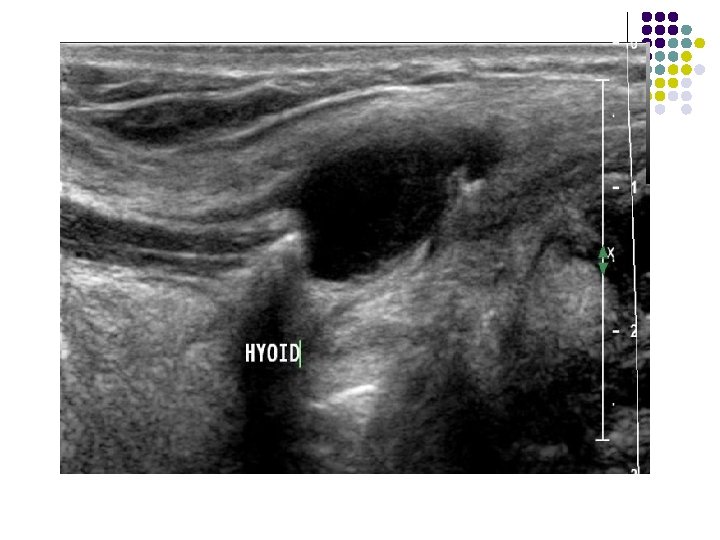
FINDINGS: sagittal ultrasound image (left is superior) shows a cystic anechoic structure just below the level of the hyoid bone. A small beak of the cyst can be seen passing superiorly over the hyoid.
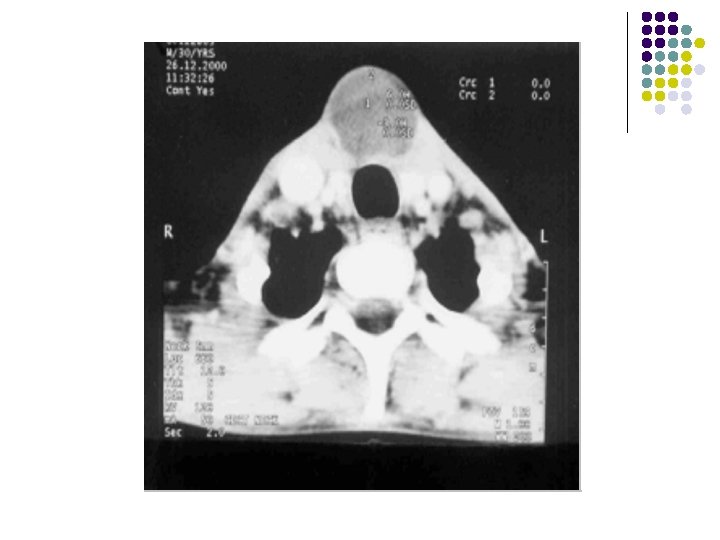

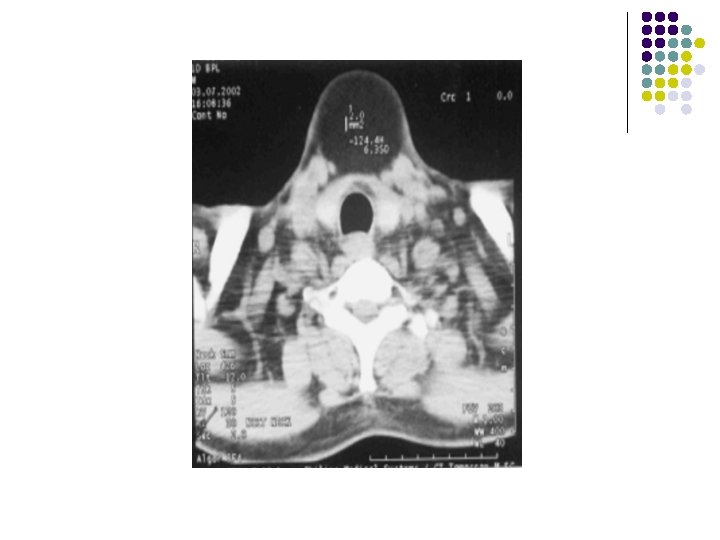
Findings: l Soft tissue density lesion in midline below the level of hyoid bone embedded within the strap muscles.

Differential diagnosis for cystic anterior neck mass. l l l Thyroglossal duct cyst Dermoid Lipoma Branchial cleft cyst Lymphadenopathy Abscess ( if complex mass )

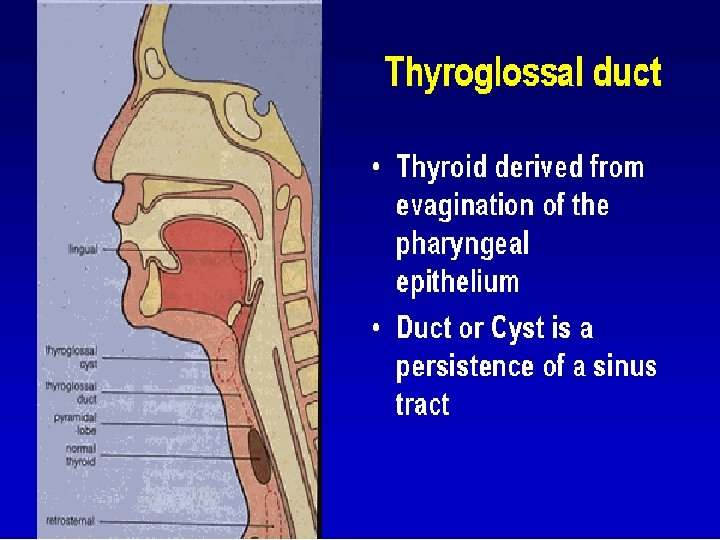
Thyroglossal Duct Cyst l l Most common congenital neck mass. The second most common benign neck mass after benign lymphadenopathy. l An epithelial lined tubular structure which originates at the foramen cecum located at the base of the tongue. l l The duct then descends through the musculature of the tongue through the mlyohyoid muscle. By 7 weeks gestation, the thyroid gland has traversed the duct and is positioned anterior and lateral to the proximal trachea. l The duct usually involutes and disappears by 10 weeks.

l Thyroglossal duct cysts develop anywhere along the course of the duct remnant, from the base of the tongue to the suprasternal region. l Frequently located in the region of the hyoid bone. l Cysts located above the level of the thyroid cartilage are usually midline, while cysts located below the level of the thyroid cartilage are off midline. l Presents as an asymptomatic, mobile mass in the anterior triangle of the neck WHICH MOVES ON DEGLUTITION AND ON PROTRUSION OF TONGUE. l Patients present in their teens or twenties because of enlargement and/or infection.

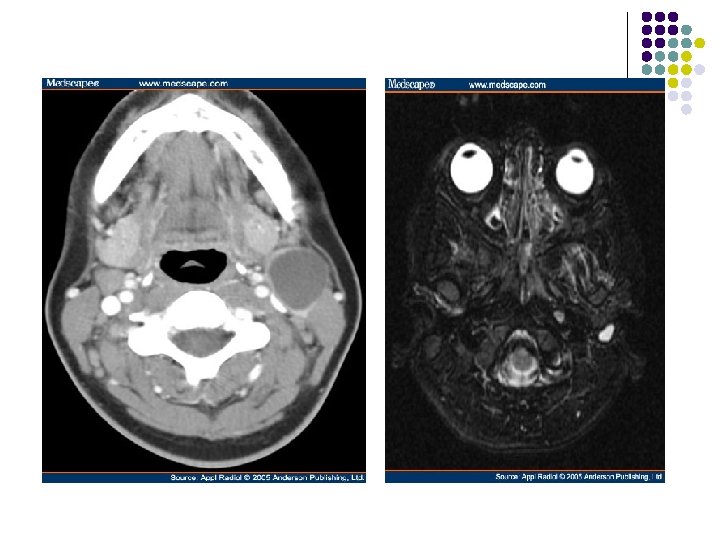
IMAGING FEATURES: l On ultrasound, they appear as hypoechoic masses with few septae and internal echoes. l CT scan : They are hypodense and well defined with minimal enhancement of the margins on contrast scans. l MR can also be used for superior soft tissue evaluation. The lesions are hypointense on T 1 W images and hyperintense on T 2 W images. l l These lesions usually lie medial to the sternocleidomastoid muscle, anterior to the carotid sheath and lateral to the thyroid gland.

Thyroglossal duct cysts location l l l Below the hyoid bone - 65% of cases At the level of the hyoid bone - 20% of cases Above the hyoid bone - 15% of cases

Thyroglossal duct cyst at & above the hyoid bone.

Infrahyoid & paramedian thyroglossal duct cysts
 and coronal (b) T")
Thyroglossal duct cyst in a 3 -year-old boy. Sagittal (a) and coronal (b) T 2 -weighted MR images show a hyperintense midline cystic mass of the foramen cecum.

T 1 -weighted sagittal image through the midline of the oropharynx and T 2 -weighted midline sagittal image. A cystic mass is identified at the junction of the myelohyoid muscle with the thyoid bone. This cyst lies just inferior and posterior to the hyoid bone.

Sagittal MR image illustrates the more typical midline homogeneously hyperintense, infrahyoid

DERMOID CYST

l Manifest - 2 nd and 3 rd decades of life with no gender predilection. l lateral eyebrow being the most common location. l About 11% of dermoid cysts of the head and neck are in the floor of the mouth, the second most common location USG l They appear as moderately thin-walled, unilocular masses, located in the submandibular or sublingual space.

US scan shows the mass with multiple echogenic foci and shadowing.

l On CT scans, the central cavity is usually filled with a homogeneous, hypoattenuating (0– 18 HU) fluid material. l It may appear to be filled with "marbles, " due to the coalescence of fat into small nodules within the fluid matrix. This "sack-of-marbles" appearance is virtually pathognomonic for a dermoid cyst in this location. l It may be heterogeneous on CT scans because of the various germinal components. Fluid-fluid levels with supernatant lipid are possible. l l The rim of these cysts often enhances following administration of contrast material.

Coronal CT scan shows the mass inferior to the mylohyoid muscle Axial contrast-enhanced CT scan shows a well-defined mass in the submandibular space with a sack-of-marbles appearance.

l MR imaging depicts the topographic relationship of these cysts to the mylohyoid muscle in the floor of the mouth and helps determine the surgical approach. l The coronal plane is optimal for determining the location. l T 1 -weighted images- variable signal intensity l T 2 -weighted images - hyperintense l The mass has a clearly demarcated rim but frequently has a heterogeneous internal appearance.

Coronal T 1 -weighted image shows the discrete intracystic foci, which have moderate hyperintensity. The mass displaces the left submandibular gland (g) inferiorly.

Dermoid cyst in a 15 -year-old woman with a 1 -week of neck swelling. Axial contrastenhanced CT scan shows a well-defined mass in the submandibularsubmental region with multiple discrete foci of hypoattenuation in the nondependent portion of the cyst.

LIPOMA

IMAGING FEATURES l l l l Well defined Encapsulated Insulates between surrounding structures Fat density No enhancement No solid component. Density of fat similar to normal body fat.

l SECOND BRANCHIAL CYST

l Second branchial cleft cysts are painless neck masses, located below the angle of the mandible, along the anterior border of the sternocleidomastoid muscle. l USG: They are cystic on ultrasound and do not usually contain internal septae. l CT scan: low density, well-circumscribed masses with rim enhancement. l They can occur at any age.

l First branchial cleft cyst. I. Contrast-enhanced axial CT at the level of the hyoid bone reveals an ill-defined, nonenhancing, water attenuation mass posterior to the right submandibular gland. l Second branchial cleft cyst. Contrast-enhanced axial CT at the level of the hyoid bone reveals a large, well-defined, nonenhancing, water attenuation mass on the anterior border of the left sternocleidomastoid muscle.

l Ultrasound of an uncomplicated branchial cyst. Note the absence of septations and the through enhancement. Axial contrast enhanced CT showing a right sided low attenuation branchial cyst.
 along the anterior border")
Axial T 1 -weighted image shows a well-defined mass (m) along the anterior border of the left sternocleidomastoid muscle (arrowhead), lateral to the carotid space (white arrow), posterior to the submandibular gland (black arrow)—the classic location for a second branchial cleft cyst. The cyst typically displaces the sternocleidomastoid muscle posteriorly or posterolaterally, pushes the vessels of the carotid space medially or posteromedially, and displaces the submandibular gland anteriorly. Increased signal intensity of the mass is due to either proteinaceous debris or prior hemorrhage. (b) Axial T 2 -weighted image reveals moderate to marked hypointensity of the mass (m), consistent with accumulation of proteinaceous debris or hemorrhage.

l Contrast-enhanced axial CT at the level of the hyoid bone reveals an ill-defined, nonenhancing, water attenuation mass (m) posterior to the right submandibular gland (g).

Contrast-enhanced axial CT at the level of the thyroid cartilage reveals a large, well-defined, nonenhancing, water attenuation mass (m) deep to the right sternocleidomastoid muscle (s), medially displacing the common carotid artery and internal jugular vein.

LYMPHADENOPATHY

ENLARGED LYMPH NODE Ultrasound of well defined hypoechoic enlarged lymph nodes

l EPIDERMOID INCLUSION CYST

l They are rare congenital lesions and are much less common than dermoid cysts in the head and neck. They appear earlier than dermoid cysts. l CT SCAN: fluid attenuation l MRI: hypointense on T 1 -weighted images hyperintense on T 2 -weighted images l An epidermoid cyst located entirely within the sublingual space.
 Axial contrast-enhanced CT scan shows")
Epidermoid inclusion cyst in a 13 -year-old woman. (a) Axial contrast-enhanced CT scan shows an encapsulated, hypoattenuated mass with partial adipose content. The coalescence of the lipid material produces a sack-ofmarbles appearance.

ABSCESS

l Usually rapidly developing and painful and may be associated with fever and leukocytosis. l Frequently involve the nodal groups draining the primary site of infection. l A third of cases of suppurative cervical lymphadenopathy are associated with pharyngitis and tonsillitis, a third with dental infection and a third with dermatologic and otologic infection. l Imaging distinguishes the ill-defined edema of cellulitis from the coalesced and cystic abscess requiring surgery. l IMAGING: Abscesses frequently have thick ring-configured enhancement and may be multiloculated.
 draining the site of an")
Enhanced CT demonstrates confluent, necrotic submandibular lymph nodes (asterisk) draining the site of an infected dental procedure. The subcutaneous fat is infiltrated (arrow) and the airway is encroached on.

CYSTIC ANTERIOR NECK LESIONS THYROGLOSSAL DUCT CYST DERMOID 2 ND BRANCHIAL CYST EPIDERMOID Medial to sternocled. Ant to carotid sheath Lateral to thyroid SUBMANDIBULAR /SUBLINGUAL DEBRIC/FAT Moves on deglutitiontoungue protrusion Sacks of marble appearance - Minimal rim enhancement Enhancing rim LYMPH NODE Multiple Hypoechoic with Echogenic hilum Intranodular flow Ant. Sernocle. Lateral-carotid sheath Post-SMG No septation Rim enhancement ABSCESS C/F Asso. LN Irregular wall Multiple septations Thick rim enhancement LIPOMA Well defined Encapsulated Insulates between surrounding structures Fat density No enhancement No solid component. Density of fat similar

IN OUR PATIENT… l l Midline ant. Neck mass which moves on protrusion of toungue. Anechoic cystic lesion in infrahyoid region with beak extenmding in suprahyoid region on usg. on. Ct. . Low density lesion with mininmal rim enhancement and in classical location. DIAGNOSIS: THYROGLOSSAL CYST

CASE 3 l A 17 YEARS OLD PATIENT PRESENTED WITH H/O RECURRENT RITHT LOWER ABDOMINAL PAIN.
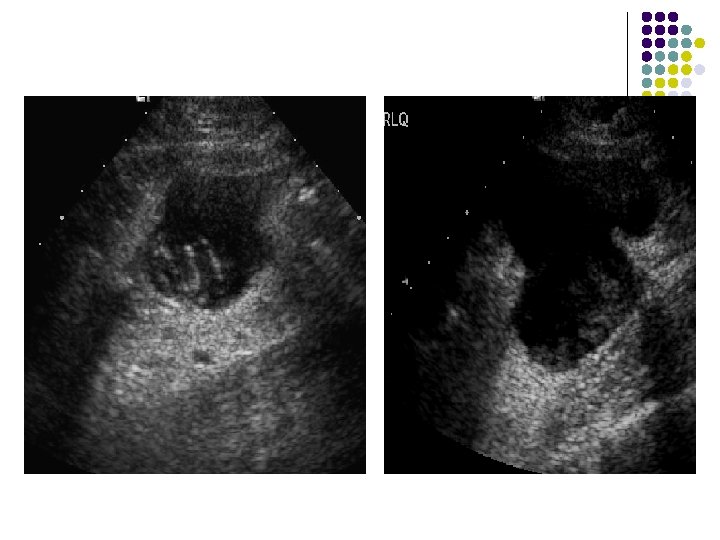

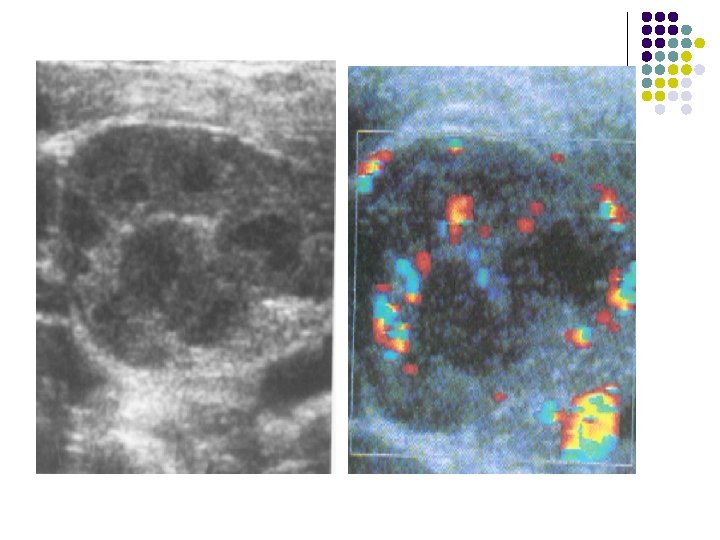
ULTRASOUND: l A well-defined, hypoechoic, cystic structure with posterior acoustic enhancement seen in right illiac fossa. l There is debris posteriorly within this cystic structure.
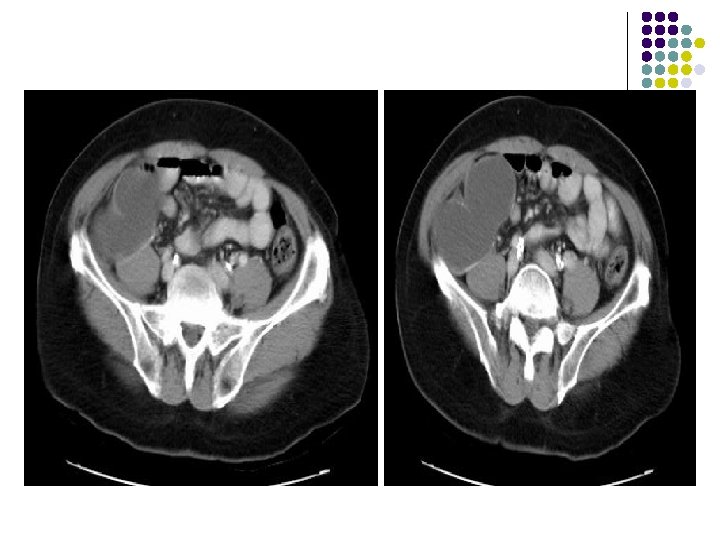
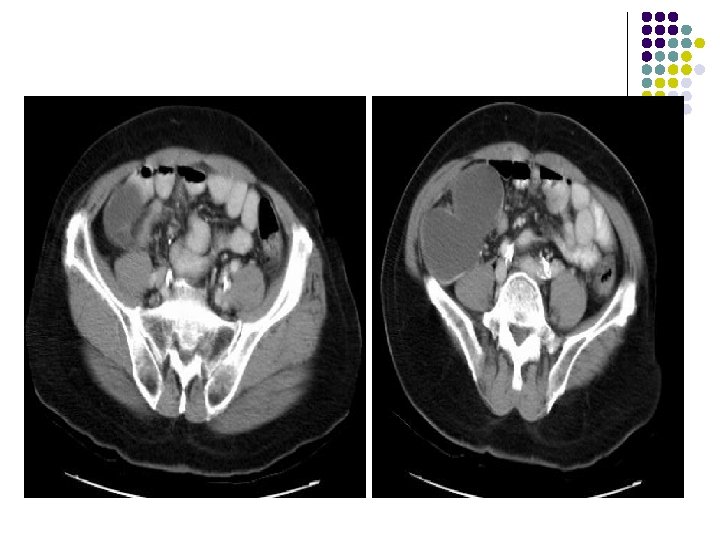

CT: l There is a bilobed, thin-walled, fluidattenuation mass in the right iliac fossa. l There is some calcification in the posterior wall of this lesion. l l The mass abuts the cecum The appendix is not visualized separately.

Diagnosis: l MUCOCELE OF APPENDIX

DISCUSSION l It is a rare condition. 25% of mucoceles are asymptomatic. l Mucocele is a descriptive term indicating that the appendix is dilated due to intraluminal mucinous secretions. l It develops slowly and appendix may become quite large. l l CAUSES: Obstructing lesions…. post-appendicitis scarring, carcinoma of appendix, cecum or ascending colon and appendiceal volvulus. Rupture of a mucocele leads to pseudomyxoma peritonei.

IMAGING FEATURES l Plain abdominal film: A well-defined right lower quadrant mass. l Contrast enema: Smooth indentation of the medial aspect of the cecum & non-opacification of the appendix. l Ultrasound: Completely anechoic or hypoechoic with variable internal echogenicity and Whorled appearance is characteristics due to internal contents May have posterior acoustic enhancement. with variable wall thickness and calcification.

l CT: Cystic structures with thin well-defined walls. Contents are usually of homogenous fluidattenuation. Calcification may be noted in the wall. l MR: If the mucocele contains predominantly fluid it will have low signal intensity on T 1 weighted images and high signal intensity on T 2. If, however, the mucocele contains a significant amount of mucin, it will appear hyperintense on both T 1 and T 2 weighted images.


CASE 4 l. Four-week-old premature infant with abdominal distension.
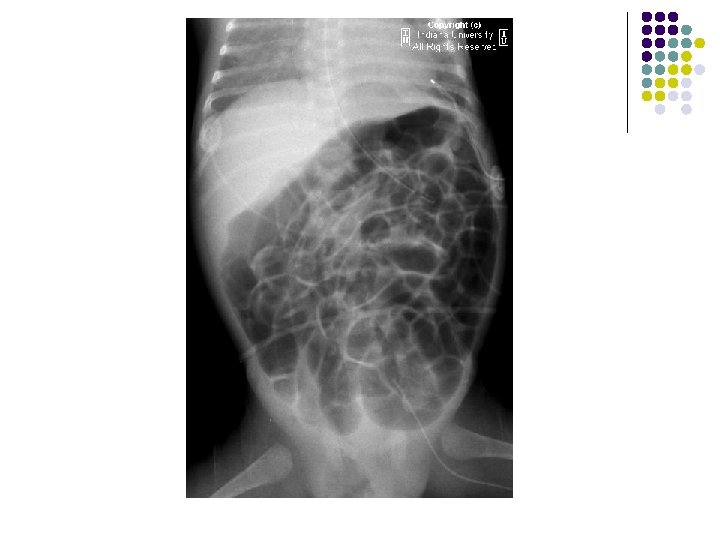
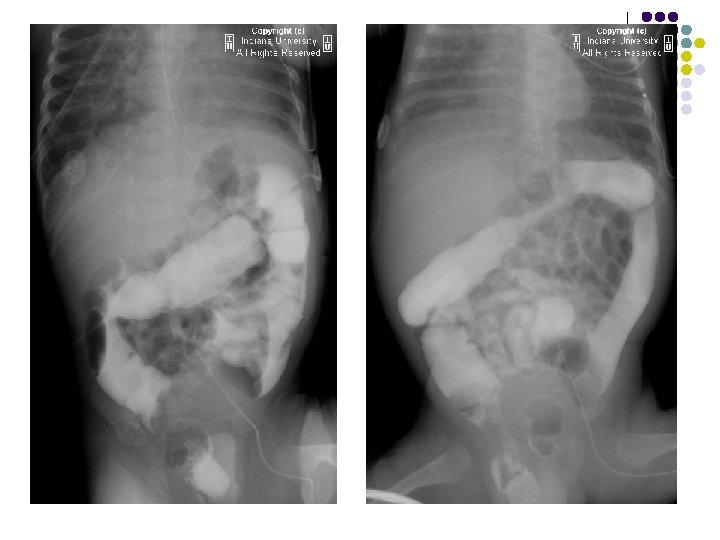

FINDINGS l Supine AP radiograph of the abdomen reveals a normal abundant bowel gas pattern with no evidence of obstruction. l However, gas is seen within a small bowel loop in the right inguinal region. l Delayed supine AP images of the abdomen from a small bowel series demonstrates contrast within a small bowel loop within the right hemiscrotum.

DISCUSSION l A protrusion of bowel from the abdomen into the groin through a weakness in abdominal musculature (direct) or through a patent processus vaginalis (indirect). l 99% of inguinal hernias in children are indirect. l The processus vaginalis is a thin layer of peritoneum travels with the testis as they descend into the scrotal sac during the seventh month of gestation. l The processus vaginalis does not begin to obliterate until around nine months gestational accounting for the higher incidence of inguinal hernias in premature and low birth weight infants l More commonly right sided , M: F - (9: 1) , l As a bulge or swelling in the groin or scrotum.

RADIOLOGICAL FEATURES: ON PLAIN RADIOGRAPH: l A loop of air filled bowel will be seen outside the expected location of the abdomen/pelvis. l Occasionally, bowel will be visualized within the scrotum. l Further imaging is usually not needed. SMALL BOWEL FOLLOW THROUGH: l Contrast within a small bowel loop in the right inguinal canal. l Ultrasound is the imaging modality of choice in adults. A loop of bowel demonstrating peristalsis within the inguinal canal is diagnostic. The exam is performed at rest and with the valsalva maneuver in order to diagnose easily reducible hernias.

CASE 5 l Forty-year-old male with retrosternal pain.
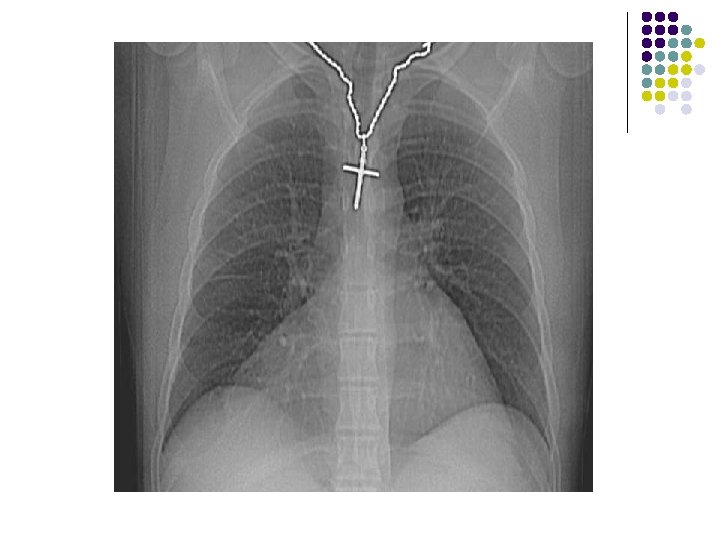

CHEST X-RAY: l A large smooth bordered opacity projecting in the right cardiophrenic angle. l Vessels and the right heart border can be seen through the opacity, which may be of fat density.


CT FINDINGS: l A large amount of fat density adjacent to the right heart border which contains multiple small vessels and is in continuity with abdominal fat in the mesentery. l A portion of the transverse colon lies within the inferior portion. l There is no evidence of bowel obstruction

CASE 4 l. Four-week-old premature infant with abdominal distension.

case 1 l A young patient presented with c/o Ankle pain

- Slides: 108