Carotid Trials in Progress and Predictions on Outcomes










 All Stroke - Stenting Trials for High Risk")








 Carotid artery stenosis >/=")

")

 Randomisation to Stenting or Surgery Funded to 2014 -")

 Centre open Joining Newcastle Hospitals Sunderland Royal Infirmary")













- Slides: 49
Carotid Trials in Progress and Predictions on Outcomes Kenneth Rosenfield, MD, FACC, FAHA Section Head, Vascular Medicine and Intervention Massachusetts General Hospital Boston, Massachusetts, U. S. A.
Kenneth Rosenfield, MD Conflicts of Interest • • Consultant – Abbott Vascular – Baxter – Harvard Clinical Research Institute – Micell – Complete Conference Management – Vortex – Endospan Equity – Icon – Cardio. MEMs – Medical Simulation Corporation – Vortex – Primacea • Research or Fellowship Support – Abbott Vascular – Cordis – Lutonix/Bard – Boston Scientific – Baxter – Atrium – IDEV • Board Member – VIVA Physicians • www. vivapvd. com
Carotid Trials – Where have we come from?
Stroke Prevention by Intervention Summary of what evidence we have… RCT’s: CEA vs. OMT Symptomatic High-risk Asymptomatic High-risk None Symptomatic Standard-risk NASCET ECST completed* None Asymptomatic Standard-risk VA Trial ACAS ACST 1
ACST - Early vs. Deferred Carotid Endarterectomy in Asymptomatic Patients with ICA Stenosis Any Stroke or Perioperative Death Time (years) Benefit of medical Rx with revascularization over Med Rx alone ACST Investigators. Lancet 2004; 363: 1491 -1502
RCT’s: CAS vs. OMT for stroke prevention Symptomatic High-risk Asymptomatic High-risk None Symptomatic Standard-risk Asymptomatic Standard-risk None In absence of “head to head” trials vs. OMT, can only infer ability of CAS to prevent stroke based on: a) registry studies of CAS and b) RCT’s comparing it to CEA!
Carotid Artery Disease RCT’s: CAS vs. CEA completed* SAPPHIRE * Symptomatic High-risk None Asymptomatic High-risk KENTUCKY * Symptomatic Standard-risk ongoing None Asymptomatic Standard-risk EVA 3 s, SPACE 1 * ACT 1, SPACE 2, ACST 2 CREST
SAPPHIRE >50% Stenosis Sx ³ 80% Stenosis Asx One or More Comorbidity Conditions Physician Team: Neurologist, Surgeon, Interventionalist CONSENSUS: 747 pts enrolled SURGICAL REFUSAL RANDOMIZED 334 INTERVENTIONAL REFUSAL TREATED 310 Stent Registry n=409 We should have refused more CEA n=151 patients! Surgical Registry n=7 STENT n=159
SAPPHIRE Trial: 1 -Year Outcome sxatic and asxatic high surgical risk patients Cumulative Percentage of MAE 30 25 Carotid Endarterectomy 20 20. 1% p=0. 048 15 Nitinol Stent 10 12. 0% 5 0 0 30 60 90 120 150 180 210 240 270 300 330 360 Time after Initial Procedure (days)
SAPPHIRE 3 -Year Outcomes Freedom from MAE N Engl J Med 2008; 358: 1572 -9
30 Day Event Rates (2000 --->2008) All Stroke - Stenting Trials for High Risk Surgical Patients Factors: embolic protection, experience, case selection
Protect Stroke and Death 1. 8%
Carotid Disease - Natural History Unanswered Questions • Effect of. . . – Sxatic status – Degree of narrowing – Morphology and consistency – Location – Patient substrate – standard or high surgical risk patient • Clinical consequences – Benign or not (stroke, MI, death)
Carotid Disease - Revascularization Unanswered Questions • Effect of. . . – Patient substrate • Standard or high surgical risk patient • Sxatic status • Age – Lesion status • Degree of narrowing • Location • Morphology and consistency
Carotid Revascularization Unanswered Questions • Optimal lesion characterization – Severity • DUS • CTA • MRA • Angiography – Embolic potential (risk stratification) • DWI • Plaque characterization (e. g. ulceration) • Biological plaque imaging –
Carotid Revascularization Unanswered Questions • Selection of optimal revascularization modality – CEA – Stenting
Carotid Stenting Unanswered Questions • Equipment – Embolic protection • Proximal • Distal – Stent • Closed-cell • Open-cell • Covered or “meshed” • Access site – Femoral – Upper extremity – Direct carotid - cutdown or puncture
Carotid Disease Adding to the evidence base… Randomized Controlled Trials in Progress • SPACE 2 • ACST 2 • ACT 1 Randomized Controlled Trials Planned • CREST 2 Single Arm Trials and Registries • NCDR CARE and SVS • Gore and MDT Prox protection
SPACE 2 – “Stent-protected angioplasty in Asymptomatic Carotid Artery Stenosis” • • Funding – German Research Council Start date – original 1/07; revised 11/09 Countries – Austria, Germany, Switzerland Hypothesis – Superiority of revasc (CAS or CEA) c/t OMT – CAS not inferior to CEA • Primary Outcome – Death or any stroke w/n 30 days – Ipsilat stroke within 5 yrs. • Design – RCT – three open arms – OMT plus CAS – OMT plus CEA • Inclusion – <86 y. o. ; 6 mos w/o sx’s
SPACE 2 Asymptomatic (no ipsilateral symptoms within previous 180 days) Carotid artery stenosis >/= 70% Ultrasound proven by certified study personal Informed consent Randomisation CEA n=1550 Procedure within 30 days CAS n=1550 Procedure within 30 days conservative n=540 Optimal medical treatment up to 5 years
SPACE 2 – “Stent-protected angioplasty in Asymptomatic Carotid Artery Stenosis” Progress • # Pts to be randomized - 3523 patients • Currently – <300 (after two years) • Randomization scheme altered to: From: Asx patient <86 y. o. To: Asx patient <86 y. o. * CAS CEA * Best Medical Tx Revasc- either CEA or CAS Best Medical Tx
The HTA/BUPA Foundation ACST-2 • A large simple randomised trial of CEA (carotid endarterectomy) vs CAS (carotid stenting) for the prevention of stroke • Aims to randomise 5000+ patients with asymptomatic carotid stenosis in whom intervention is thought to be clearly needed, but where there is substantial uncertainty as to which procedure is best
ACST-2 • Subjects in whom CEA and CAS are anatomically suitable are randomized 1: 1 to CEA or CAS. • The main outcomes are 1 -month stroke/MI/death and long term stroke (5 or more years). • Randomization and 1 -month evaluations are performed by the study doctor, and long term follow up is primarily though direct contact from the ACST office.
Asymptomatic Carotid Stenosis Trial (ACST-2) Randomisation to Stenting or Surgery Funded to 2014 - Plans • 200 centres to randomise at least 5000 patients • Experience with more devices, longer follow up, determine groups who may/ may not benefit Since randomisation started (2 years) • 45 Centres (16 countries) have entered patients • 127 centres have joined or are joining
16 Countries Randomising in ACST-2 Belgium Czech Republic France Germany Greece Ireland Israel Italy Netherlands Norway Poland Serbia Slovenia Spain Sweden United Kingdom
ACST-2 UK 25 centres (Mar 2010) Centre open Joining Newcastle Hospitals Sunderland Royal Infirmary James Cook Hospital Royal Preston Hospital Univ Hospital North Durham Bishop Auckland General Hospital Univ Hospital of South Manchester Royal Infirmary Hull Royal Infirmary Sheffield Vascular Institute Norfolk and Norwich Univ Hospital Queens Medical Centre, Nottingham Addenbrookes Hospital Southend Univ Hospital of North Staffordshire St Mary’s London Sandwell and West Birmingham St Georges, London Bristol Royal Infirmary Belfast Bournemouth East Kent and Canterbury Royal Sussex, Brighton
Centre Recruitment 125 62 Mar 2010
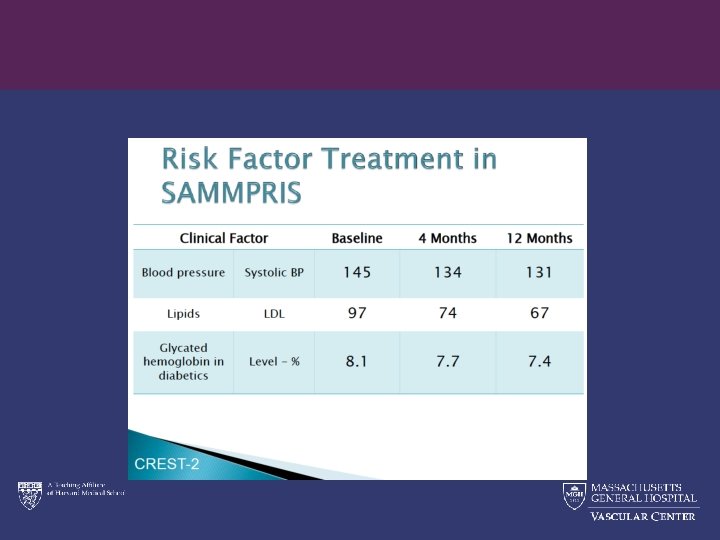
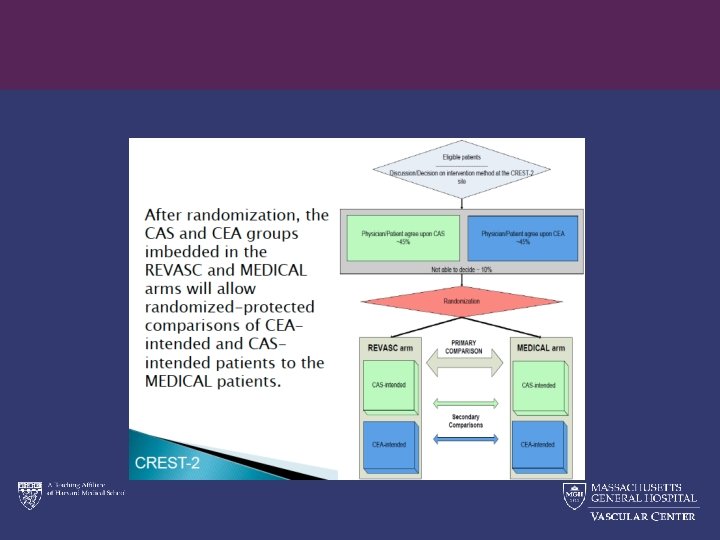
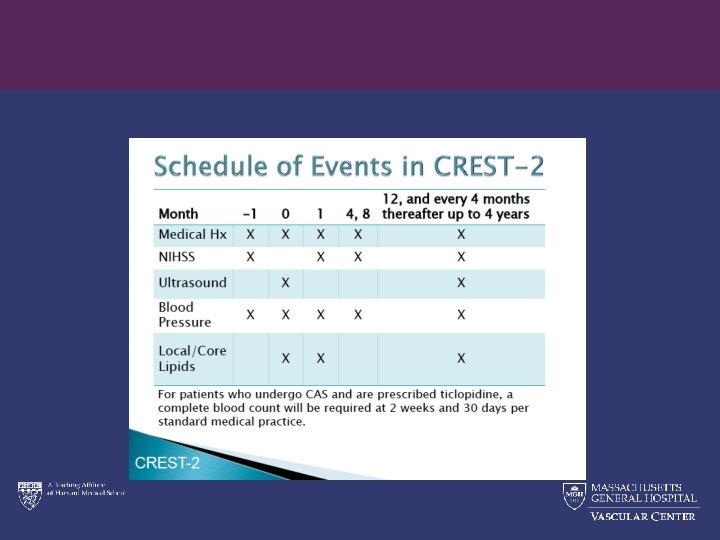
CREST 2 • 950 patients at ~70 centers • Power ~90% to detect 4. 8% treatment difference (1. 2% per year) • Primary Endpt – Composite of stroke or death within 30 days or ipsilat stroke up to 4 years • SAMMPRIS – style Intensive medical management • Criteria – >35 y. o. ; asymptomatic for 180 days – >70% stenosis (det by DUS, CAT, MRA, CBA) – Series of exclusion criteria each for CEA and CAS
Asymptomatic Carotid stenosis, stenting versus endarterectomy Trial Carotid stenting is not currently approved by the FDA for asymptomatic patients who are at standard risk for surgery. CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use. 39 AP 2928021 Rev A Confidential: This information is confidential and is intended for distribution to ACT I Study Site participants ONLY. This document contains Abbott Laboratories and Abbott Vascular proprietary information and shall not be duplicated, disclosed to others, or used for purposes other than to carry out the intent for which this material is delivered. © 2008 VIVA 2008 ( Las Vegas, NV) nd
Summary - ACT 1 Focus only on asymptomatic patients – excludes high risk for CEA--protocol defined – excludes high risk for CAS--protocol defined – surgeon and interventionalist criteria are strict and verified (IMC and SMC) – Independent neuro assessment – embolic protection required – central core labs, independent audit
ACT I: Study Design • Prospective, randomized, 2 -arm, multicenter trial • 3: 1 randomization CAS to CEA • Lead-in enrollment of up to 400 subjects • Maximum of 1658 pivotal subjects • Followed at 1, 6, 12 months & annually for 5 yrs • Contemporary medical therapy for all patients VIVA 2007 ( Las Vegas, NV) th
Key Inclusion Criteria • Subject > 18 and 80 years of age. • Subject asymptomatic – no stroke or TIA (hemispheric or ocular) within 180 days prior to procedure – neurologist must confirm status • Carotid stenosis >70% and <99% by carotid duplex (accredited lab) or angiography (visual estimate)
Key Exclusion Criteria Clinical • Bilateral significant carotid stenosis (contralateral stenosis > 60% by duplex or angiography) • High risk surgical candidate • Known cardiac sources of emboli
Primary Endpoint Composite • Any stroke*, myocardial infarction and death during 30 -day post procedural period • Ipsilateral stroke* between 31 and 365 days post procedure *Independent neurologic assessment
Summary - ACT 1 • ACT 1 will focus on evaluating CAS in asymptomatic patients – excludes high risk for CEA--protocol defined – excludes high risk for CAS--protocol defined – surgeon and interventionalist criteria are strict and verified – standardized protocol: embolic protection – central corelabs, independent audit
ACT 1 - Enrolling Sites as of September 2008 Deaconess Medical Center University of Rochester William Beaumont Hospital Oregon Health & Science University NYU Medical Center Albany Medical Center Rush University Medical Center Our Lady of Lourdes St. John’s Hospital / Prairie Medical North Central Heart Institute El Camino Hospital Hoag Memorial Hospital Presbyterian Kaiser Foundation Hospital – San Diego St. Joseph Hospital Wellness Center St. Luke’s Hospital, Phoenix Hospital of Univ. of Pennsylvania Allegheny General Hospital Cleveland Clinic Foundation Parkview Hospital Wellmont Holston Valley Berks Cardiology Stern Cardiovascular Center Chesapeake General Hospital St. Mary’s Hospital/ VA Cardiovascular Specialists Presbyterian Heart Institute-Dallas St. Luke’s Episcopal Hospital, Houston Wake Medical Center Providence Medical Center Duke University Westlake Medical Center th Washington Hospital Center Riverside Methodist Hospital Harrisburg Hospital / Pinnacle Health Austin Heart P. A. VIVA 2007 ( Las Vegas, NV) Lenox Hill Hospital Columbia Presbyterian Millard Fillmore Hospital Detroit Medical Center Northwestern University Memorial Hospital Kaiser Permanente Hawaii Massachusetts General Hospital St. Francis, NY St. Luke’s Milwaukee Dartmouth Cardiovascular Inst. of the South Ochsner Clinic Foundation Baptist Hospital of East Tennessee Forsyth Medical Center BCVI
ACT I: Outcomes Lead In Patients Event 30 days, N=180 Death, Stroke and MI 1. 7% (3/180) All Stroke and Death 1. 7% Major Stroke and Death 0. 0% All Stroke 1. 7% Major Stroke 0. 0% Minor Stroke 1. 7% MI 0. 0% 31 -365 days, N=157 Ipsilateral Stroke 47 0. 0%
Therapy for Carotid Stenosis Conclusions IV The Future - better definition of patients appropriate for… • Medical Therapy • CEA only • Stenting only • Patients in “gray zone” between revasc or no revasc • Patients who could benefit equally from either CEA or CAS and are appropriate for both