Welcome to Mental Health Training Darren De Lint










. Historical treatments (Aversion")










 Antelope House. Elmleigh. Parklands Leigh")










A patient who has attained the age of 16 years")




 husband or wife or civil partner;")
): (a) anyone")





 are part of")














- Slides: 70
Welcome to Mental Health Training Darren De Lint
Introductions Fire Smoking Loos
Programme Introduction What is Mental Disorder/illness? How are mental health services arranged in Southampton? Coffee The Mental Health Act Ancillary legislation. DOLs/MCA. The role of the Approved Mental Health Professional. Future challenges. Questions.
Quotes “O “One person's craziness is another person's reality. ” Tim Burton “I became insane, with long intervals of horrible sanity. ” Edgar Allan Poe “Inside every sane person there's a madman struggling to get out, " said the shop keeper. "That's what I've always thought. No one goes mad quicker than a t ota totally sane person. ” ― Terry Pratchett, The Light Fantastic.
What is Mental Disorder/illness? Bio/Psycho/Social model. Aetiologically non-specific. Social Construction? Cultural differences. Mechanism of control?
Biological Model Historically overseen by psychiatry. International classification of diseases. Diagnostic Statistical Manual. Use of pharmacological interventions (SSRI’s, Anti. Psychotics, mood stabilisers). ECT treatment. Historical frontal lobe lobotomy, Coma induced therapy with insulin etc.
Major Depressive Disorder Generic name Amisulpride Amitriptyline Amoxapine Agomelatine Bupropion Citalopram Clomipramine Desvenlafaxine Doxepin Duloxetine Escitalopram Fluoxetine Fluvoxamine Imipramine Lamotrigine Mirtazapine Moclobemide Nortriptyline Paroxetine Brand names Amazeo, Amipride, Amival, Deniban, Solian, Soltus, Sulpitac, Sulprix Tryptomer, Elavil, Tryptanol, Endep Asendin, Asendis, Defanyl, Demolox, Moxadil Valdoxan, Melitor, Thymanax Elontril, Wellbutrin Celexa, Cipramil, Talohexane Anafranil Norpramin, Pertofrane Pristiq Aponal, Adapine, Silenor, Sinquan, Sinequan, Zonalon Cymbalta Cipralex, Lexapro Fluctin, Fludac, Fontex, Foxetin, Lovan, Prodep, Prozac, Sarafem, Symbyax Luvox, Faverin, Fevarin Antideprin Lamictal, Lamictin, Lamogine Remeron, Avanza Aurorix, Manerix Aventyl, Pamelor Aropax, Paxil, Pexeva, Seroxat
DSM 5
Internet Gaming Disorder
Caffeine Use Disorder
Psychological Psychotherapy. CBT. Counselling. DBT. Improving Access to Psychological Therapies (IAPT). Historical treatments (Aversion therapy).
Rosenhan Experiment 1973 healthy associates or "pseudopatients“. who briefly feigned auditory hallucinations in an attempt to gain admission to 12 different psychiatric hospitals in five different states in various locations in the United States. All were admitted and diagnosed with psychiatric disorders. The second part of his study involved an offended hospital administration challenging Rosenhan to send pseudopatients to its facility, whom its staff would then detect.
Social Construction Model Most service users believe that a medical model based on deficit and pathology still dominates public and professional understanding of mental health issues, shaping attitudes and policy. The labelling and stigma following from a medical model of mental illness emerge as major barriers for mental health service users. Our unequal society and the costs of this to mental health; leads to an unequal distribution across population groups of mental health problems and in people’s ability to recover and lead fulfilling lives.
Victorian Reasons for admission
History of mental health legislation. 1808 County Asylums Act An Act for the better Care and Maintenance of Lunatics, being Paupers or Criminals in England “Whereas the practice of confining such lunatics and other insane persons as are chargeable to their respective parishes in Gaols, Houses of Correction, Poor Houses and Houses of Industry, is highly dangerous and inconvenient”, County JPs were given powers to construct asylums.
• 1828 Chancery Lunatics Property Act “An Act for extending the Acts passed in the forty-third and fifty- ninth years of the reign of his late majesty King George third, for the sale of mortgages of estates of persons found lunatics by inquisition taken in England Ireland, so as to authorise such sale and mortgage for some purposes; • 1832 Anatomy Act Allowed workhouses and hospitals to sell unclaimed bodies to accredited anatomy schools. Put a stop to the trade of the “resurrectionists” who robbed graves. • 1983 Representation of the People Act this allowed patients in mental hospitals to vote using an address that was not the hospital. The address requirement was to avoid having large mental hospitals like those in Hertfordshire deciding who the local MP was.
Anti-Psychiatry movement
The NHS structure explained
How to access secondary Care services? GP. Accident & Emergency. Nearest Relative referral to the AMHP service. Primary care professional, counsellor nurse etc. IAPT.
SHFT Pathways
Pathway’s continued
Inpatient Services Bluebird House (specialised services - secure adolescent) Antelope House. Elmleigh. Parklands Leigh House (specialised services - adolescent) Western Hospital Older Persons Mental Health. Ravenswood (specialised services - medium secure adult) Southfield (specialised services - low secure adult)
The Care Programme Approach 'Secondary mental health services' use CPA. This is the term used to mean mental health services that are more specialist than your GP. Care Coordinator. Established in 1990 NHS Community Care Act. The Care Programme Approach (CPA) is used to plan many people’s mental health care. Usually delivered by one of the core professional staff group.
Who gets help under the CPA? Problems with looking after yourself including: self-harm, suicide attempts, harming other people including breaking the law, a history of needing urgent help, not wanting support or treatment, and vulnerability such as financial difficulties, physical or emotional abuse or being open to exploitation. Severe distress at the moment or in the past Problems working with mental health services now or in the past
• Learning disability or drug or alcohol misuse as well as a mental illness • Services from a number of agencies, such as housing, physical care, criminal justice or voluntary agencies • Recently been ‘sectioned’ under the Mental Health Act 1983 or you are detained at the moment • Recently been put in touch with the Crisis Team or are getting their help at the moment
New SHFT Service redesign Three CMHT’s East, West and Central matching GP Cluster arrangements. Referrals from GP’s no longer undertaken by AAT. GP allocated to CMHT to process referral. H@H will become Acute Mental Health Team 24 hours. AOT will merge into the teams. EIP will remain separate service. Shared Care will remain. Psychiatric liaison operate later working hours + weekends.
Coffee
The Mental health Act 1983 Darren De Lint
What is a mental disorder? Section 1 “Mental Disorder” means any disorder or disability of the mind “Learning Disability” means a state of arrested or incomplete development of the mind which includes significant impairment of intelligence and social functioning Long term sections must have abnormally aggressive or seriously irresponsible conduct Dependence on alcohol or drugs is not considered to be a disorder or disability of the mind
Civil Sections Section 2 Section 3 Admission for assessment A patient may be admitted to a hospital and detained there for a period not exceeding 28 days beginning with the day in which he is admitted An application for admission for assessment may be made in respect of a patient on the grounds that He is suffering from a mental disorder of a nature or degree which warrants the detention of the patient in a hospital for assessment (or for assessment followed by medical treatment) for at least a limited period; and He ought to be so detained in the interests of his own health or safety or with a view to the protection of other persons Admission for treatment which can last for an initial period of up to six months An application for admission for treatment may be made in respect of a patient on that grounds that He is suffering from mental disorder of a nature or degree which makes it appropriate for him to receive medical treatment in a hospital; and It is necessary for the health or safety of the patient or for the protection of other persons that he should receive such treatment and it cannot be provided unless he is detained under this section; and Appropriate medical treatment is available
Section 2 and Section 3 Applications shall be founded on the written recommendations in the prescribed form of two registered medical practitioners, including in each case a statement that in the opinion of the practitioner the conditions set out in subsection (2) are complied with
Section 4 Admission for assessment in cases of emergency An emergency application may be made either by an approved mental health professional or by the nearest relative of the patient; and every such application shall include a statement that is of urgent necessity for the patient to be admitted and detained under Section 2 An emergency application shall be sufficient in the first instance if founded on one of the medical recommendations required by section 2 shall cease to have effect the expiration of a period of 72 hours from the time when the patient is admitted to the hospital
Section 7 Guardianship Order. (1)A patient who has attained the age of 16 years may be received into guardianship (2)A guardianship application may be made in respect of a patient on the grounds that— (a)he is suffering from mental disorder, F 1. . . of a nature or degree which warrants his reception into guardianship under this section; and (b)it is necessary in the interests of the welfare of the patient or for the protection of other persons that the patient should be so received.
Section 135 Warrant to search for and remove patients Reasonable cause to suspect that a person believed to be suffering from mental disorder has been, or is being, ill-treated, neglected or kept otherwise than under proper control, in any place within the jurisdiction of the justice, or being unable to care for himself, is living alone in any such place The justice may issue a warrant authorising any constable to enter, if need the by force, any premises specified in the warrant in which that person is believed to be, and , if thought fit, to remove him to a place of safety In the execution of a warrant a constable shall be accompanied by an approved mental health professional and by a registered medical practitioner A patient who is removed to a place of safety in the execution of a warrant issues under this section may be detained there for a period not exceeding 72 hours
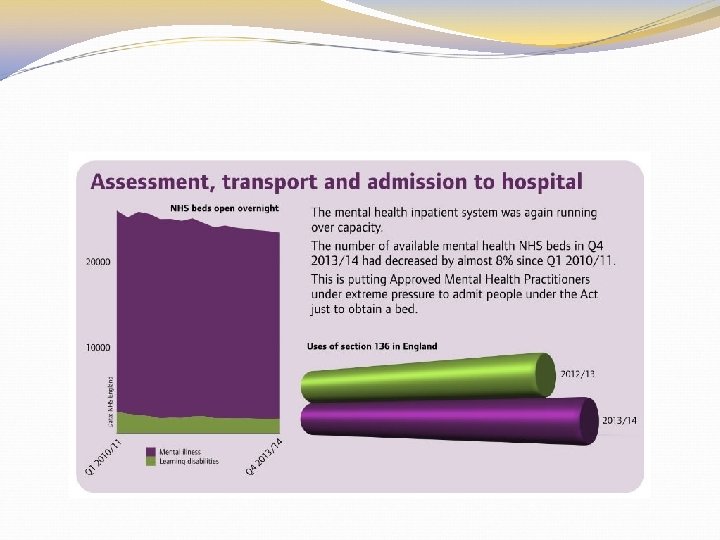
Section 136 Mentally disordered persons found in public places A person removed to a place of safety If a constable finds in a place to under this section may be detained there for a period not exceeding 72 which the public have access a hours for the purpose of enabling him person who appears to him to be examined by a registered suffering from mental disorder medical practitioner and to be in immediate need of interviewed by an approved mental health professional and of making any care and control, the constable may, if he thinks it necessary to do necessary arrangements for his treatment or care so in the interests of that person A constable, an approved mental or for the protection of other health professional or a persons, remove that person to a authorised by either of them take a place of safety within the meaning person detained in a place of safety to one or more places of safety of Section 135
s 117 Section 117 imposes a duty on health and social services to provide aftercare services to certain patients who have been detained under the Mental Health Act. Care Act clarifies the definition of aftercare. Must meet both the following requirements: (a) Meeting a need arising from or related to the person’s mental disorder; and (b) Reducing the risk of the person’s mental condition (and, accordingly reducing the risk of the person requiring admission to hospital again for treatment for mental disorder.
S 117 Eligibility For treatment under Section 3 Under a hospital order pursuant to Section 37 (with or without a restriction order) or Following transfer from prison under Section 47 or 48. However, Section 117 does not apply to: Patients detained in hospital for assessment under Section 2 Patients emergency under Section 4 Patients detained in hospital under Section 5(2) Patients who were not detained under any section (informal or voluntary patients).
S 26 Nearest Relative Order of precedence (a) husband or wife or civil partner; or where there is no marriage or civil partnership, or the husband/wife/civil partner is disqualified (see below), any person who has lived with the patient as husband/wife/civil partner for six months (s 26(6); (b) son or daughter; (c) father or mother; (d) brother or sister; (e) grandparent; (f) grandchild; (g) uncle or aunt; (h) nephew or niece; (i) any person, other than a relative, with whom the patient (ii) has ordinarily resided for at least 5 years (s 26(7))
Disqualified Persons Certain people are disqualified from being the NR (s 26(5)): (a) anyone not ordinarily resident in the UK, Channel Islands or Isle of Man - unless the patient is not so resident either (b) a husband or wife if there has been a permanent separation or desertion. (c) anyone under 18 years of age, except the husband, wife, father or mother of the patient
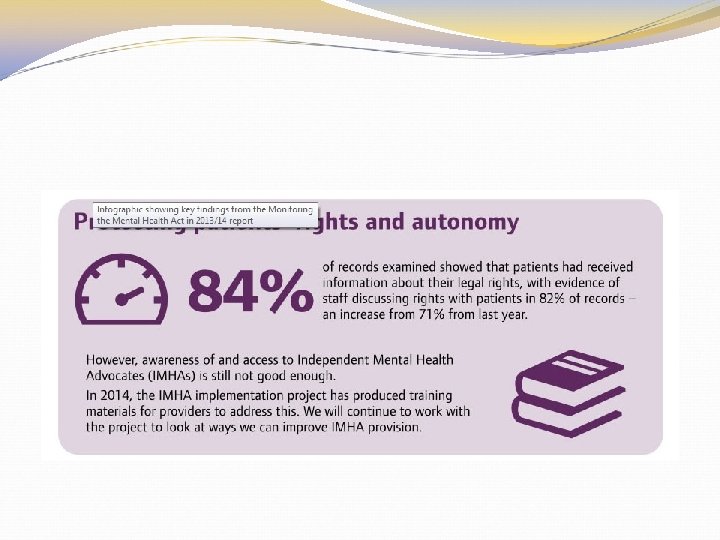
Rights of Nearest Relative apply for a section or a guardianship. object to the section and or placed under a guardianship. discharge if you are sectioned and apply to the Mental Health Tribunal if this is refused. ask for an independent advocate. To be consulted and/or given information. appoint someone else to act as nearest relative.
Mental Capacity Act 2005
Capacity For the purposes of this Act, a person lacks capacity in relation to a matter if at the material time he is unable to make a decision for himself in relation to the matter because of an impairment of, or a disturbance in the functioning of, the mind or brain. It does not matter whether the impairment or disturbance is permanent or temporary. A lack of capacity cannot be established merely by reference to— a person's age or appearance, or a condition of his, or an aspect of his behaviour, which might lead others to make unjustified assumptions about his capacity.
5 Principles A person must be assumed to have capacity unless it is established that he lacks capacity. A person is not to be treated as unable to make a decision unless all practicable steps to help him to do so have been taken without success. A person is not to be treated as unable to make a decision merely because he makes an unwise decision. An act done, or decision made, under this Act for or on behalf of a person who lacks capacity must be done, or made, in his best interests. Before the act is done, or the decision is made, regard must be had to whether the purpose for which it is needed can be as effectively achieved in a way that is less restrictive of the person's rights and freedom of action.
Making decisions to understand the information relevant to A person lacks capacity in the decision relation to a matter if at the material time he is unable to retain that information, make a decision for himself to use or weigh that in relation to the matter information as part of the process of making the decision, or to communicate his decision (whether by talking, using sign language or any other means).
Deprivation of Liberty Safeguards The Deprivation of Liberty Safeguards (Do. LS) are part of the Mental Capacity Act 2005. They aim to make sure that people in care homes, hospitals and supported living are looked after in a way that does not inappropriately restrict their freedom. The safeguards should ensure that a care home, hospital or supported living arrangement only deprives someone of their liberty in a safe and correct way, and that this is only done when it is in the best interests of the person and there is no other way to look after them
Mental Health Act or DOLS? 14. 19 situations where Act should be used instead of Do. LS 1. Valid and applicable advance decision to refuse necessary treatment 2. Conflict with decision of attorney, deputy, guardian or Court of Protection 3. Person objecting
14. 22 Reasons for using Act Fluctuating capacity and expectation of refusal once capacity is regained Restraint not justifiable as proportionate under Mental Capacity Act –e. g. risk to others Specific identifiable risk that person would not receive treatment without Mental Health Act
e of Practice 2015 establishes Using the Act - Principles o Least restrictive - emphasis on prevention - avoid blanket restrictions o Empowerment and involvement – (previously participation) encourage advance statements - Encourage patient to involve carers o Respect and dignity – includes not discriminating o Purpose and effectiveness – Care and treatment should be in accordance with up-to-date national guidance and/or current best practice o Efficiency and equity - applies to commissioners and organisations
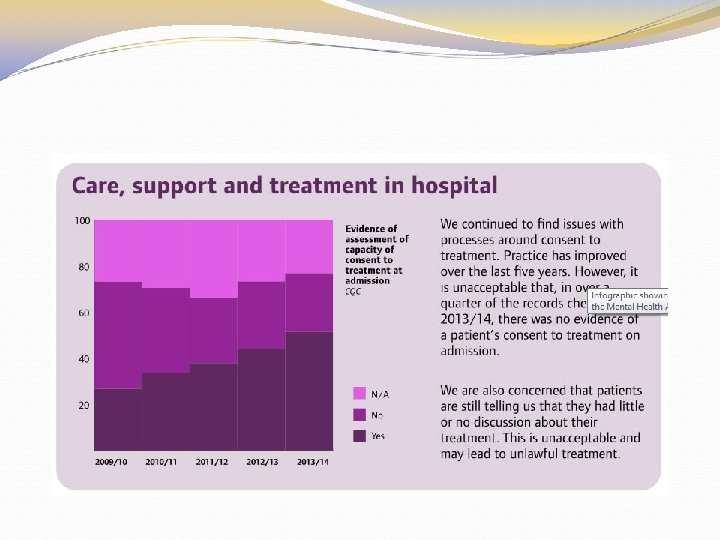
Chapter 24 Medical Treatment New: Wishes/ advanced statements/decisions should be taken into account New: Treatment should have strong evidence base “ 24. 17 Part 4 A patients, who have the capacity to consent to. . treatment, may not be given that treatment unless they consent. There are no exceptions to this rule, even in emergencies. . treatment can be given without their consent only if. . recalled to hospital. ” New: 24. 57 -24. 62 Promoting physical health e. g. Patients should have their nutritional state assessed on admission and at regular intervals. . using an accredited screening tool.
Chpt 16. Police powers and places of safety; Many similarities to the old code with some additions S. 135(1): 16. 4 “…a person should be told the reasons for removal before they are removed. . ” 16. 5 “…the intended place of safety should be identified, and the necessary arrangements made, before a warrant is applied for under section 135(1). . ” 16. 5 “…Proper planning should ensure that it is not necessary to use a police station as a place of safety for people removed under section 135(1)…”
s. 136 Slightly expanded guidance; 16. 18 ‘A place to which the public have access’ includes places to which members of the public have open access, access if a payment is made, or access at certain times of the day” 16. 23 “…the police may also benefit from seeking advice before using section 136 powers in cases where they are unsure that the circumstances are sufficiently serious for using these powers. Local protocols should set out how this advice can be provided and who the police should contact…”
Chapter 5 Nearest Relative Guidance on identification, appointment by county court, much almost identical to old Chapter 8 5. 2 if the NR is not the carer, professionals should also involve the carer 5. 6 If there is no NR, and the person lacks capacity to decide to apply, the AMHP should apply to the County Court to appoint.
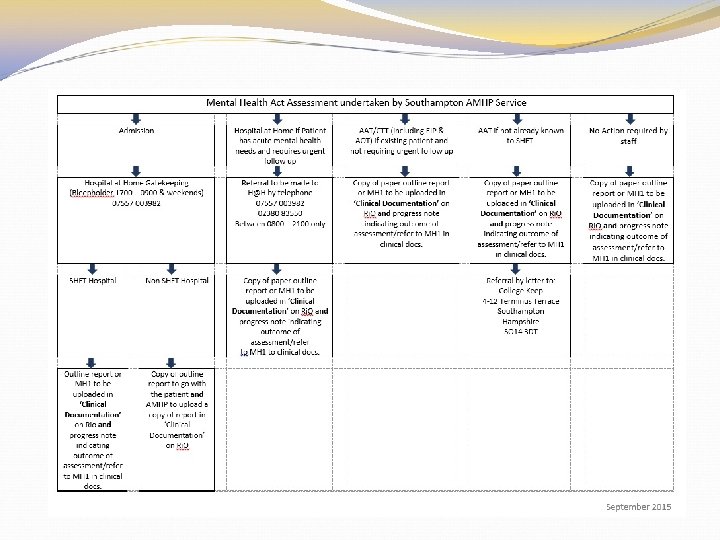
The role of approved AMHPs are responsible for organising, co-ordinating and contributing to Mental Health Act assessments. LA’s have a statutory obligation to ensure they have enough AMHP’s to provide cover for a 24 hour rota. S 114 of the MHAA LA’s are responsible for approving a person to act as an AMHP’s are the applicant’s in Mental Health Act Assessments (they have the final say!).
Professional Power Patient power Family and advocates Public good Care and treatment Human rights Civil liberties Role of the Approved Mental Health Professional
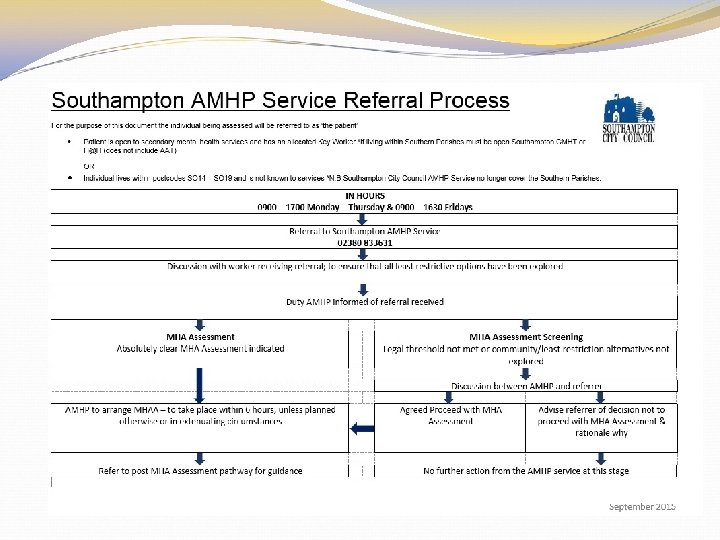
Southampton AMHP Service The Southampton City Council AMHP service covers 24 hours 365 days a year. Since August 2014 the Southampton City Council AMHP service has withdrawn from the s 75 agreement and is now wholly based and managed by the local authority. Based at HCH. Only cover postcodes SO 14 -SO 19. Annual Budget of 800 k.
Core Functions AMHP Team
Southampton AMHP Service Referrals to be made to Southampton AMHP Service directly; Monday to Thursday and 09. 00 - 17. 00 Fridays 09. 00 – 16. 30 02380 833631 OUT OF HOURS remains the same directly to the Duty AMHP mobile; 07795 564491 Referrals can be accepted via email on; amhpteam@southampton. gcsx. gov. uk
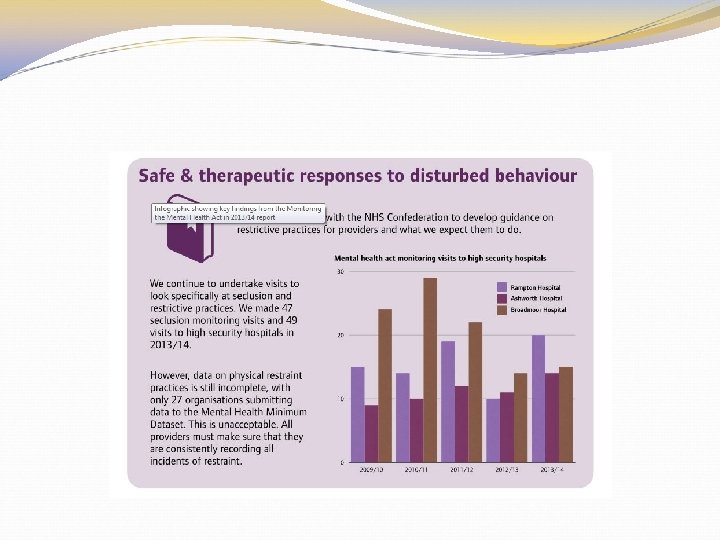
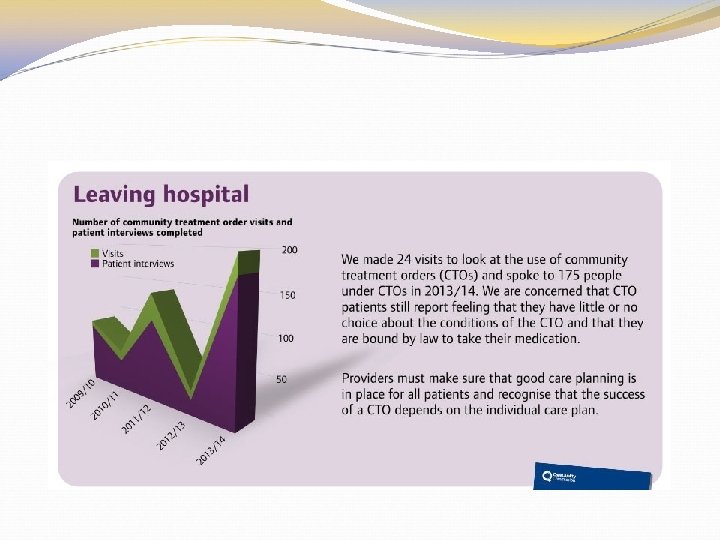
Challenges for the future.