Vasoactive drugs Ian Lyons Senior Clinical Fellow Critical




![Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2](https://slidetodoc.com/presentation_image_h/33c2284fde6bd1b5deb56e1fb964076b/image-5.jpg "Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2")
![Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2](https://slidetodoc.com/presentation_image_h/33c2284fde6bd1b5deb56e1fb964076b/image-6.jpg "Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2")
![Vasopressors DO 2 =CO{(1. 34 x [Hb] x Sp. O 2 ) + (Pa.](https://slidetodoc.com/presentation_image_h/33c2284fde6bd1b5deb56e1fb964076b/image-7.jpg "Vasopressors DO 2 =CO{(1. 34 x [Hb] x Sp. O 2 ) + (Pa.")













 BP = CO x SVR")



 Levosimendan")




 V – Inhibitors")





![Distributive shock DO 2 =CO[(1. 34 x [Hb] x Sp. O 2 ) +](https://slidetodoc.com/presentation_image_h/33c2284fde6bd1b5deb56e1fb964076b/image-39.jpg "Distributive shock DO 2 =CO[(1. 34 x [Hb] x Sp. O 2 ) +")
")







 ◦ 0 -40 ml/hr � IV bolus ◦")
 ◦ 0 -40 ml/hr � IV bolus ◦")






 � Start it when")






![Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2](https://slidetodoc.com/presentation_image_h/33c2284fde6bd1b5deb56e1fb964076b/image-63.jpg "Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2")


















 2) 3) are asked to see the patient… What further")







 Why? ◦ 2) What are your immediate management steps?")
 Why? ◦ 2) What are your immediate management steps?")


 What other drugs should be started? � 2) What other management")


 What do you think is going on? � 2)")
 What do you think is going on? ◦ Likely")

 What are your priorities? � 2) Who else")
 Dressings taken down � 2) TV ultrasound scan in")




 � Tracheostomy � Ongoing CVVH")

- Slides: 107
Vasoactive drugs Ian Lyons, Senior Clinical Fellow, Critical Care October 2017
Overview � The science bit…. � Practicalities �A case
The science bit…. � Basic science � Systemic circulation ◦ Pressors ◦ Dilators ◦ Drugs affecting cardiac output � Pulmonary ◦ Dilators ◦ Hypoxia circulation
Basic science
Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2 ) + (Pa. O 2 x 0. 023)]
Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2 ) + (Pa. O 2 x 0. 023)] BP = CO x SVR
Vasopressors DO 2 =CO{(1. 34 x [Hb] x Sp. O 2 ) + (Pa. O 2 x 0. 023)} BP = CO x SVR
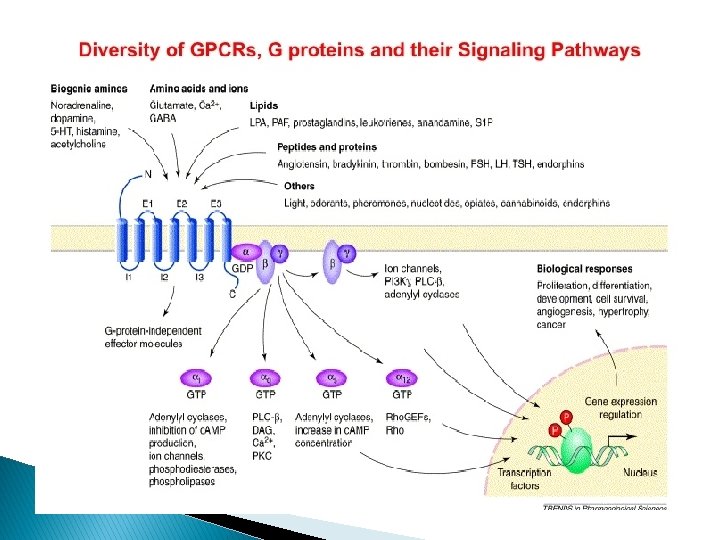
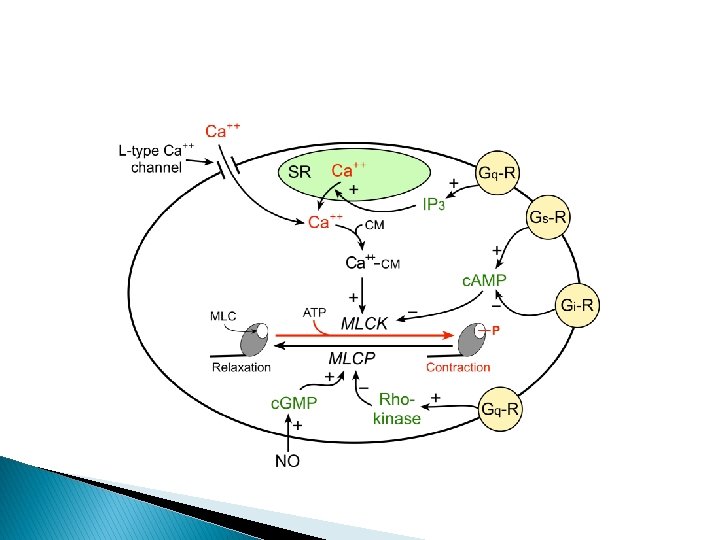
‘Basically it modulates the intracellular calcium levels……’
Shock
Shock
Adrenoceptor agonists
Adrenoceptors and functions
Adrenoceptor agonists � Noradrenaline ◦ Produced in adrenal gland, and in sympathetic nerve terminals ◦ Acts on both α and β adrenoceptors �Main effect by α 1 adrenoceptors Increases SVR Peripheral vasoconstriction Splanchnic vasoconstriction Other agents with a mainly alpha effect: Metaraminol Phenylephrine
Adrenoceptor agonists � Adrenaline ◦ Produced in the adrenal gland ◦ Acts on β receptors more than α initially ◦ Increases cardiac output �Both contraction (inotropy) and heart rate (chonotropy) ◦ May reduce SVR at lower doses �Increases SVR at higher doses
Adrenoceptor agonists � Adrenaline ◦ β effects predominant at low doses ◦ α 1 effects increase at higher doses � Ephedrine ◦ α and β effects � Dopamine ◦ β (low dose) and α (high dose) effects as well as direct dopamine receptor effects
Vasopressin � Antidiuretic � Potent hormone vasoconstrictor ◦ Doesn’t act on adrenoceptors � Can be effective when unresponsive to adrenoceptor agonists
Vasopressin
Calcium � Second messenger throughout the body ◦ Can increase cardiac contractility. ◦ May aid vasoconstriction if Ca 2+ is low
Vasodilators � Indications ◦ Hypertension ◦ Heart failure ◦ Angina ◦ Specific regions �Ischaemic limbs �Pulmonary hypertension
Vasodilators � Arterial � BP vs venous = CO x SVR
Anti-adrenergics �α blockers ◦ (e. g. Prazosin, Phentolamine, Phenoxybenzamine) BP = CO x SVR �β blockers (e. g. Labetalol, Bisoprolol, Esmolol)
Nitrates � Typically infusions � Act via endothelium ◦ c. GMP-mediated pathway ◦ Sodium Nitroprusside ◦ Glyceryl Trinitrate ◦ Arterial and Venous action
Calcium channel blockers Different mechanisms of action E. g. Verapamil – primarily cardiac Dihydropyidines act predominantly on the vasculature ◦ E. g. Amlodipine, Felodipine, Nimodipine
When should I use what � If needing to block both α and β receptors, then block α first (e. g. phaeochromocytoma) � If labile BP, then infusion (e. g. GTN, esmolol) are best � Don’t use Calcium channel blockers and β-blockers
Inotropes/Mixed effects � BP = CO x SVR Calcium β-agonists Inodilators (PDE inhibitors) Levosimendan
Inodilators � � E. g. Milrinone, Aminophylline Increases CO, reduces ED pressure, myocardial oxygen extraction unchanged May cause arrhythmia, may effect coronary perfusion
Levosimendan � Calcium sensitising agent ◦ Originally used for heart failure ◦ Currently being investigated in sepsis � Single � Trial infusion 7 days effect results suggest it’s not effective….
Pulmonary circulation p. BP = CO x PVR
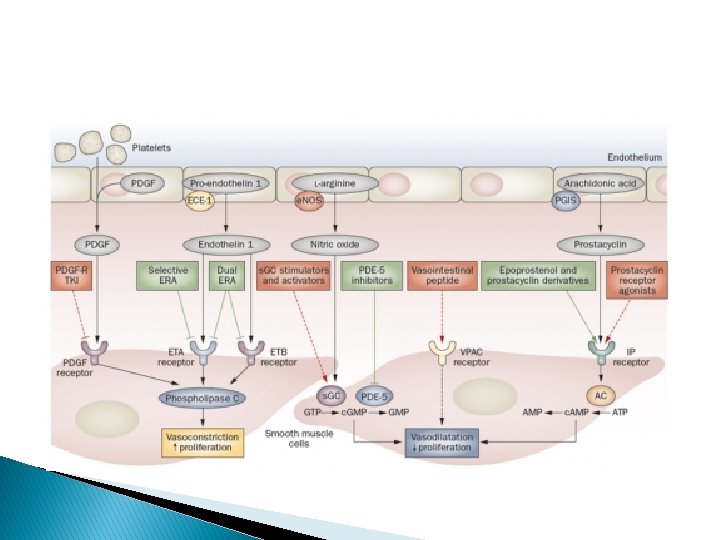
Pulmonary hypertension � Characterised pressure by high pulmonary artery ◦ Variety of causes � Pulmonary hypertension ◦ Many different causes �Require investigation at specialist centre (Sheffield) ◦ Less production of NO and Prostacyclin
The same approach – different drugs � Prostanoids � PDE (Iloprost) V – Inhibitors (Sildenafil) � Endothelin antagonists (Bosentan)
Hypoxic pulmonary vasoconstriction � Hypoxia is a potent vasoconstrictor in the pulmonary circulation � Can be a useful response – improves V/Q
Hypoxic pulmonary vasoconstriction � Calcium mediated response ◦ Volatile agents can reduce HPV ◦ Can lead to chronic change
Summary � Most vasoactive drugs act to directly or indirectly alter calcium �A variety of different receptors – usually GPCR � Many drugs have both vasoactive and inotropic effects � Pulmonary and systemic circulations respond to different drugs. .
Practicalities……
Practicalities � Treat the right thing… � When and which one should I start? � How much is too much? � Starting � What adjuncts and other drugs else should I do…
Distributive shock DO 2 =CO[(1. 34 x [Hb] x Sp. O 2 ) + (Pa. O 2 x 0. 023)] BP = CO x SVR
Distributive shock � Causes: ◦ ◦ ◦ Sepsis Burns Pancreatitis Anaphylaxis CNS (spinal injury) Adrenal insufficiency
Distributive shock � Fix ◦ ◦ ◦ the underlying problem Sepsis – Source control Burns – Burns management + grafting Pancreatitis – Organ support +/- intervention Anaphylaxis – Specific management CNS (spinal injury) – Sheffield protocol Adrenal insufficiency - Steroids
Distributive shock � Targets: ◦ BP ◦ Sp. O 2 ◦ U. O. ◦ Lactate
Distributive shock � Targets: ◦ BP - 65 -70 mm. Hg (Higher if known HTN) �Higher in specific protocols (Spines, TBI) ◦ Sp. O 2 - <94 � 88 -92 in specific circumstances ◦ U. O. - >0. 5 ml/kg/hr ◦ Lactate - <2. 0? ? ?
Distributive shock � When should I start something?
Distributive shock � When should I start something? ◦ Adequately fluid resuscitated? ◦ Signs of inadequate end organ perfusion? ◦ Low BP?
Distributive shock � What to start? BP = CO x SVR
Metaraminol
Metaraminol � Infusion (0. 5 mg/ml) ◦ 0 -40 ml/hr � IV bolus ◦ (1 ampoule in 20 ml) ◦ 0. 5 mg-1 mg boluses �Can give higher if needed � Can give peripherally ◦ Good in a rush, or to bridge to CVC
Metaraminol � Infusion (0. 5 mg/ml) ◦ 0 -40 ml/hr � IV bolus ◦ 0. 5 mg-1 mg boluses �Can give higher if needed � Can give peripherally ◦ Good in a rush, or to bridge to CVC � Can get tachyphylaxis � Less potent than other drugs � Can cause a reflex bradycardia � If on escalating doses, do we need a CVC and something stronger?
Noradrenaline
Noradrenaline � MUST be an infusion via CVC � Very potent vasoconstrictor � 1 st choice to counter vasodilatation
Noradrenaline � MUST � We � Very � Start be an infusion via CVC potent vasoconstrictor � 1 st choice to counter vasodilatation talk about ml/hr ◦ We should talk about mcg/kg/min it at a decent dose to get it down the line ◦ ~0. 4 ml to get into circulation � If on norad you need an art line ◦ Doesn’t mean you have to wait till you’ve got on in to start…
Noradrenaline – what do the doses mean � 0 -0. 4 mcg/kg/min ◦ Noradrenaline is usually sufficient alone � 0. 4 -0. 6 mcg/kg/min ◦ ◦ Consider CO monitoring (especially if adding 2 nd agent) Consider 2 nd agent (? Vasopressin ? Adrenaline) ? Steroids / ? calcium ? Senior input � >0. 6 mcg/kg/min ◦ High dose – risk of ischaemic injury ◦ Increasing doses will have less and less effect ◦ Senior input (if not already aware)
Adding a second agent � Which one should I pick? ◦ Adrenaline? �Risk factors for Cardiac pathology �? Myocardial suppression in sepsis �Consider Scv. O 2 �Aiming for 70% ◦ Vasopressin? �Further vasoconstriction needed
Adding a second agent � Which one should I pick? ◦ Adrenaline? �Risk factors for Cardiac pathology �? Myocardial suppression in sepsis �Consider Scv. O 2 �Aiming for 70% ◦ Vasopressin? �Further vasoconstriction needed
Vasopressin � Antidiuretic hormone ◦ Standard infusion (0 -6 ml/hr) � Start it when there’s SVR is still low with noradrenaline � Be careful in gut pathology ◦ Lactate may rise… � If you’re starting it someone senior ought to know � Watch the sodium…
Distributive shock � Common things to consider ◦ Are we adequately fluid resuscitated? �Art line swing? �SVV (aim for less than 10%) �Clinical examination (CRT, cold peripheries) ◦ Are drugs the answer? �Do we need to image? �Do we need to go to theatre? �Otherapies
Other drugs we use � Steroids ◦ No one agrees when to start…. �Generally around 0. 3 -0. 4 mcg/kg/min and increasing doses of noradrenaline �Typically hydrocortisone 100 mg loading �Then 50 mg qds ◦ Stop when the noradrenaline is improving (certainly less than 0. 3 mcg/kg/min) ◦ Things to watch out �BMs (? Sliding scale) �Electrolytes (Na+ and K+)
Other drugs we use � Calcium ◦ Some people like it, some REALLY don’t �Remember how much of the body’s Calcium is in the blood �If Calcium is low (<2. 0 mmol/L or <1. 0 mol/L on ABG) then possibly replace �May be effective if on inotrope/vasopressor �Can cause arrhythmias… � 10 ml of 10% Calcium gluconate in 100 ml 0. 9% saline over 30 mins �Can use 10% calcium chloride – it’s 3 x stronger
A few quirks of distributive shock � Burns ◦ Noradrenaline can be used ◦ Vasoconstriction affects the skin before most other sites � Anaphylaxis ◦ Adrenaline is the key… �Mast cell stabilisation…. �Can help with diagnosis (HR will decrease…)
What’s the diagnosis?
Cardiogenic shock � What’s the underlying cause? ◦ Acute Heart failure �MI? �Cardiomyopathy? �Is it obstructive?
Maintaining delivery of oxygen DO 2 =CO[(1. 34 x [Hb] x Sp. O 2 ) + (Pa. O 2 x 0. 023)] BP = CO x SVR
Cardiogenic shock �A fine balance…… ◦ A failing heart should not be unduly stressed ◦ CO should meet the bodies needs…… � Adrenaline or Dobutamine (or GTN)
Which drug to start… � Dobutamine ◦ Can reduce LV afterload in systolic failure � Can be used peripherally � Typical doses 2. 520 mcg/kg/min
Which drug to start… � Dobutamine ◦ Can reduce LV afterload in systolic failure � Can be used peripherally � Typical doses 2. 520 mcg/kg/min � In acute heart failure can increase mortality � Can cause a tachycardia. . � In our units we don’t use it very often at all…
Which drug to start… � Adrenaline � In an emergency, bolus peripherally ◦ Cardiac arrests � Can be used in an infusion ◦ Central line � Good in mixed shock ◦ Or when dobutamine isnt enough
Which drug to start… � Adrenaline � Lactate � In � Tachycardia an emergency, bolus peripherally ◦ Cardiac arrests � Can be used in an infusion ◦ Central line � Good in mixed shock ◦ Or when dobutamine isn’t enough acidosis ◦ Often limits dose � May BP cause a DROP in ◦ Vasodilatation � Can � If cause arrhythmias it doesn’t work…
Which drug to start… � Adrenaline � In an emergency, bolus peripherally ◦ Cardiac arrests � Can be used in an infusion ◦ Central line � Good in mixed shock ◦ Or when dobutamine isn’t enough � Dose range is 01 mcg/kg/min � Low doses - primarily β effect � High doses- increasing α effect
Which drug to start � GTN � Vasodilator ◦ Good to lower BP in some situations ◦ Cardiogenic pulmonary oedema ◦ Reduce LV afterload � Can be given as a sublingual dose ◦ Can be given as an infusion � Can rapidly develop tolerance � Not a good choice in some conditions ◦ TBI/Neurosurgery
Cardiogenic shock – Other treatments � Rule ◦ ◦ ◦ out reversible factors Hypovolaemia Tamponade Acute MI Electrolytes Dysrhythmias
Cardiogenic shock – Other treatments � Many inotropes are also vasodilators ◦ May need some constriction… �A difficult balance � Mechanical support ◦ Intraaortic balloon counterpulsation �Often (in NUH) put in post PPCI �Effective at improving coronary perfusion � 18% get limb ischaemia… �May need anticoagulation ◦ LVAD and ECMO… ◦ A bridge to transplant…
Don’t forget hypovolaemia
Hypovolaemia � Common in many pathologies ◦ If you’re underfilled… �You can’t squeeze an underfilled circulation �You can’t pump blood you don’t have � Consider hypovolaemia and fluid resuscitation in all forms of shock… ◦ Fluid therapy is a different talk…
Summary � Make sure you’ve got the right diagnosis � Drugs work better if your well filled � In distributive shock � In cardiogenic shock ◦ Noradrenaline then Vasopressin (or Adrenaline) ◦ Remember adjuncts ◦ Adrenaline is often the answer ◦ Mechanical therapies may be needed
A case study
Case �A 65 year old presents having fallen over in her garden 24 hours beforehand… she has a painful rapidly advancing cellulitis on her right leg � PMH ◦ Mild asthma ◦ HTN
Case � Pre-morbid state ◦ Lives independently ◦ ET – Unlimited � NKDA � Meds ◦ Amlodipine
Case � BP 80/50 � HR 120 � Sp. O 2 95% on 24% O 2 � RR 30 � Temp 38. 5 o. C � VBG ◦ p. H 7. 32 ◦ BE -3. 0 ◦ Lac 2. 0
Case � Treatments so far?
Case � Treatments ◦ ◦ ◦ so far Oxygen IV Access IV antibiotics 5 L Crystalloid Paracetamol Clexane…
Case � You 1) 2) 3) are asked to see the patient… What further history would you like? What further investigations should be performed What is your management plan….
On going management � Seen by plastics ◦ Make stab incisions – no fat necrosis ◦ Recommend conservative management with Abx � Any ◦ ◦ further specialist opinions Where should the patient be admitted? What investigations are needed? What treatments are needed? What procedures are needed?
Initial critical care management � Admitted to Critical care ◦ Art line inserted �BP 70/50, HR 130 ◦ CVC inserted Catheterised 60 ml urine (not passed urine in the 6 hours prior to admission to crit care ABG (on 40% O 2) p. H 7. 32, p. CO 2 3. 2, p. O 2 10. 2, HCO 3 - 12
Further management � 4 litres of crystalloid given in AICU ◦ U. O. remains <10 ml/hr ◦ Noradrenaline started (0. 15 mcg/kg/min) ◦ Further fluid boluses � D/W micro ◦ Fluclox and Clinda ◦ IVIg � Repeat ABG (60% O 2) � Patient looks ‘tired’ ◦ p. H 7. 25, p. CO 2 5. 2, p. O 2 8. 2, HCO 3 9, Lactate 5. 3 ◦ GCS now 13/15 (E 3 V 4 M 6)
Further Management � BP 90/50 � HR 120 � U. O. ~15 ml/hr � Sp. O 2 89% on 60% O 2 � RR 20 � T 38. 9 � CRT ~3 secs, cold below elbows � Norad now 0. 2 mcg/kg/min
Next steps � What are your management priorities?
Next steps? � Decision to intubate � Plastics called back – will review within the hour � Bloods chased ◦ ◦ AKI (e. GFR 22; previously >90) Coagulopathic, plt 70 WCC 4. 0 Calcium 1. 8
Intubation � Pre-O 2 � Midazolam 3 mg � Fentanyl 200 mcg � Propofol 20 mg � Rocuronium 100 mg � Metaraminol 1. 5 mg (in 0. 5 mg boluses) � uneventful intubation � shortly after intubation BP drops acutely… ◦ Unresponsive to metaraminol
Intubation � Hypotensive… ◦ 1) Why? ◦ 2) What are your immediate management steps? � What additional monitoring would you like?
Intubation � Hypotensive… ◦ 1) Why? ◦ 2) What are your immediate management steps? � What ◦ ◦ additional monitoring would you like? Art line – no swing. . Negative straight leg raise CO monitoring PAFC? ?
Post-intubation � 2 Litres of fluid given stat � Noradrenaline increased to 0. 7 mcg/kg/min � Vas cath inserted � Reassessed � BP 100/50 mm. Hg, HR 110 � No change with fluid bolus � Lactate 8. 2 on gas � U. O. ~15 ml/hr � Sp. O 2 ~92%
Post-intubation � Further investigations � Nurses report rapid progression of erythema ◦ Scv. O 2 52% ◦ Micro contact AICU – Gram +ve cocci in blood cultures. . ◦ Pathology phone – Coagulatopathic, plt 13. .
Post-intubation � 1) What other drugs should be started? � 2) What other management should occur? � 3) How would you interpret the blood results? ◦ ◦ ◦ Hb 93, Plt 13, WCC 2. 4 Na 131, K 4. 9, Ur 4. 5, Cr 180 ALT 300, Alb 19, Bil 30, ALP 200 CK 14000 PT and APTT prolonged, fibrinogen 0. 4
Post-intubation � Adrenaline started � Surgeons r/v ◦ For urgent surgery – debridement � Haematology ◦ Vitamin K ◦ Platelets ◦ Cryo
Theatre � Necrosed fat throughout leg � Debrided ankle to hip � In theatre lactate climbs to 14 � 10 L of crystalloid in theatre � Given hydrocortisone � FICE echo in theatre ◦ Mildly impaired LV function ◦ Well filled
Return from theatre � 1) What do you think is going on? � 2) What monitoring would you like? � 3) Any furtherapies?
Return from theatre � 1) What do you think is going on? ◦ Likely necrotising fasciitis with MOF �Respiratory �CVS �DIC �Renal � 2) What monitoring would you like? � 3) Any furtherapies? �CO monitoring �Multiple vasoactives �Steroids �Specialist input
The next day � Noradrenaline 1. 1 mcg/kg/min � Vasopressin 6 ml/hr � Adrenaline 0. 7 mcg/kg/min � SVR – low; CO – high; SVV – 15% � BP 85/45, HR 120, U. O. 5 ml/hr � Respiration not changed � Lactate risen to 11… � Micro confirm Group A strep � Steroids (Hydrocrotisone 50 mg qds) started
The next day. . � 1) What are your priorities? � 2) Who else do we need to speak to? � 3) When should we return to theatre (if at all)?
Taken to theatre � 1) Dressings taken down � 2) TV ultrasound scan in theatre � 3) Laparotomy � 4) 6 Litres crystalloid in theatre ◦ further necrosis – debrided ◦ Free fluid in pelvis ◦ Essentially negative
After theatre trip � CO 9 L/min, SVV 6% � BP 120/50, HR 110, Anuric (On CVVH) � At present: ◦ Noradrenaline 1. 0 mcg/kg/min ◦ Adrenaline 0. 7 mcg/kg/min ◦ Vasopressin 6 ml/kg/min � Lactate improved 11 7. 0
after theatre… � Which infusion should we reduce first? � What should we tell the family? � What would you expect to see on an ECHO?
3 days later � CVS stable � Inotropes/vasopressors weaning � Remains sedated and ventilated � Steroids stopped
Longer term ICM management � Weaning inotropes/vasopressin � Transferred to city hospital ◦ When should you transfer the transfer? ◦ Who should go?
Further progress � 6 further trips (debridements and SSG) � Tracheostomy � Ongoing CVVH � Discharged to Gillies ward 2 months after � Discharged home 3 months after admission
Questions. .