Vasoactive Drugs Maya Govender Practice Educator CTICU FCCNC









 acetylcholine is the neurotransmitter Sympathetic Nervous System (SNS) are noradrenergic")















- Slides: 26
Vasoactive Drugs Maya Govender Practice Educator CTICU FCCNC – 30 th January 2018
Objectives • To define Inotropes • To explain the mechanisms of Inotropes • To identify the Risks and Benefits of Inotropes • To give the indications for common inotropes used in the critical care unit
Inotropes An INOTROPE is an agent which increases or decreases the force or energy of muscular contractions • Negatively Inotropic agents weaken the force of muscular contractions • Positively Inotropic agents increase the strength of muscular contraction
Vasoconstrictor • An Agent that narrows the blood vessels, which in turn increases resistance to blood flow and raises blood pressure • Causes narrowing of blood vessels
Inotropes • Inotropes strengthen the contractions of the heart so the heart can pump more blood with fewer beats • Certain inotropes may be prescribed to slow the heart rate of people with an abnormally fast heart rhythm (tachycardia) • Or to strengthen the pumping ability of a heart that is weakened because of heart failure
The Mechanism of Inotropes work via the automatic immune system: • The Autonomic Nervous System regulates activities that are automatic , or involuntary • The Nerves of the Autonomic Nervous System CONTROL Functions of the body that are NOT UNDER CONSCIOUS CONTROL • The Autonomic Nervous system seems to be concerned with striking a balance or MAINTAINING HOMEOSTASIS IN THE FUNCTIONING OF MANY ORGANS OF THE BODY
• THE AUTONOMIC NERVOUS SYSTEM IS FURTHER SUBDIVIDED INTO TWO PARTS: A. THE SYMPATHETIC DIVISION B. THE PARASYMPATHETIC DIVISION • The TWO parts have OPPOSITE EFFECTS on the ORGANS they control • Most organs controlled by the Autonomic Division are under control of both Sympathetic and Parasympathetic Neurons
Autonomic Nervous System
HOW DO INOTROPES WORK? • Inotropes act directly or indirectly on the Sympathetic Nervous System, but the effect of each varies according to which sympathetic receptor the drug has greatest affinity for • The duration of action also varies • Direct acting drugs act by stimulating the SNS receptor whereas indirect acting drugs cause the release of noradrenaline from the receptor which produces the effect • Some drugs have a mixed effect
Parasympathetic Nervous System (PNS) acetylcholine is the neurotransmitter Sympathetic Nervous System (SNS) are noradrenergic receptors and noradrenaline is the neurotransmitter • Noradrenalin is the primary neurotransmitter released by the sympathetic nervous system, which mediates the “fight or flight” reaction, preparing the body for action by affecting cardiovascular function, gastrointestinal motility and secretion, bronchiole dilation, glucose metabolism, and so on These noradrenergic receptors are further subdivided, Alpha 1 (a 1), Beta 1 (b 1), Beta 2 (b 2) and Dopamine (D)
So When you Stimulate the Sympathetic Nervous System What happens? Depends on what you stimulate it with but…. • Noradrenaline and Adrenaline levels go up • This causes activation of adrenergic receptors located in the ENDOTHELIUM
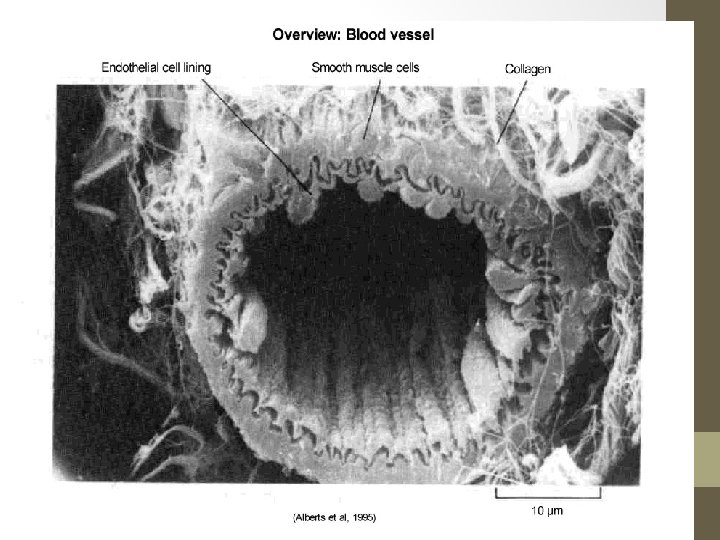
The Endothelium • The endothelium compromises a layer of cells that line the interior surface of blood vessels • Endothelial cells line the entire circulatory system, from the heart to the smallest capillary • Endothelium of the interior surfaces of the heart chambers are termed as endocardium Both blood and lymphatic capillaries are composed of a single layer of endothelial cells
Endothelial cells: • vasoconstriction and vasodilation, and hence the control of blood pressure • blood clotting (thrombosis & fibrinolysis) • Atherosclerosis • formation of new blood vessels • inflammation and swelling (oedema)
How do they work? Two types of Adrenergic receptors Both found in the vascular endothelium • Alpha (α) 1 & 2: Vascular smooth muscle and urinary tract • Beta (β) 1 & 2: Heart (B 1)
Alpha Receptors Cardiac alpha 1 Stimulation causes increase in contractility without an increase in rate. Alpha 1 and alpha 2 In peripheral vessels mediate vasoconstriction
Beta Receptors • Beta 1 STIMULATION causes increased rate and force of cardiac contraction • Beta 2 receptors = Bronchial smooth muscle dilation. Vasodilation in skeletal muscle. Also some cardiac effects
Dopamine Receptors • Stimulation = increased renal and coronary blood flow • Arterial vasodilatation
Inotropic Drugs • POSITIVE: ↑cardiac contractibility Adrenaline and Noradrenaline • NEGATIVE: ↓cardiac contractibility Beta blockers Dobutamine Dopamine Isoprenaline Calcium channel blockers
Risks and Benefits of Inotropes BENEFITS: RISK: • Improves cardiac performance • Improves contractility of myocardium • Increase blood pressure • Increased heart rate causing further deterioration of failing heart pump • Increases myocardial oxygen requirements • Potentially arrythmogenic • Can increase ischaemia
Inotropes: Noradrenaline • 0. 01 -0. 4 mcg/kg/min • Short acting – double pumping • Predominates Alpha-1 receptor agonist – vasoconstriction causing increases SVR • Uses – septic shock with low SVR Adrenaline • 0. 01 -0. 3 mcg/kg/min • Short acting – double pumping • Both alpha and beta receptor agonist. Low dose = beta activity, higher doses pre-dominantly alpha. Can cause arrhythmia • Uses – low CO, bronchospasm, cardiac arrest
Vasopressors: • Vasopressin • 0 – 4 units/hr • Controls water excretion in the kidneys + vasoconstriction of vascular smooth muscle • Deficiency in septic shock • Useful in vasoplegia, right heart failure, PHT • Side effects – abdominal cramps and reduced absorption, myocardial and peripheral ischemia • Expensive - £ 500 per box • A patient on 4 units/hr – 2 days treatment • Over 50 k spend April 2013 – April 2014 – number one cost drug on CTICU
Inotropes: Milrinone • 0 -750 ng/kg/min • Vasodilation and increased myocardial contractility • Increases CO, PCWP and reduces SVR • Long half life and accumulates in renal failure • Uses – severe congestive heart failure Dopamine • Low dose (0 -2. 5 mcg/kg/min) – increase renal + mesenteric blood flow via dopamine receptors • 2. 5 -10 mcg/kg/min – beta receptors – increase myocardial contractility, SV and CO • > 10 mcg/kg/min – alpha receptors – increase SVR, reduce renal blood flow, potential for arrhythmias
Administration • Supremely dangerous • Miniscule doses calculated on body weight • Titrated infusion (except adrenaline in cardiac arrest) • Close monitoring (ECG & Arterial line) • Double Pumping • Side effects
Inotrope infusions are a stop gap measure • The underlying cause must be treated or symptoms controlled • Managing infusions Don’t let infusions run out – make up infusions with time to spare Change over infusions with new lines as quickly as possible