The American Association for Thoracic Surgery guidelines call


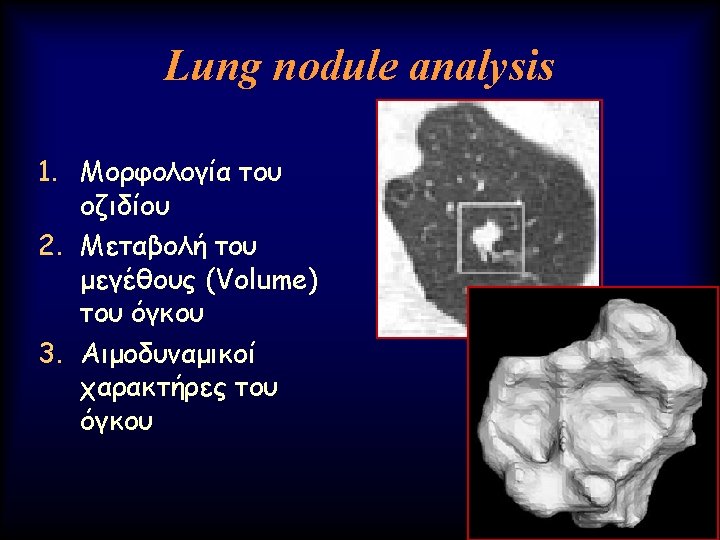

 του όγκου Ø Γρήγορο doubling time")















- Slides: 70
The American Association for Thoracic Surgery guidelines call for Annual lung cancer screening with low-dose computed tomography screening for North Americans from age 55 to 79 years with a 30 pack-year history of smoking. Long-term lung cancer survivors should have annual low-dose computed tomography to de tect second primary lung cancer until the age of 79 years. Annual low-dose computed tomography lung cancer screening should be offered starting at age 50 years with a 20 pack-year history if there is an additional cumulative risk of developing lung cancer of 5 % or greater over the following 5 years.
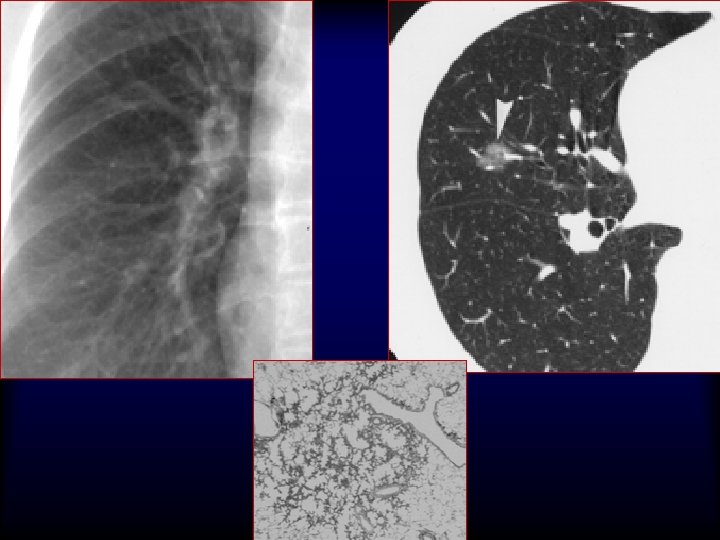
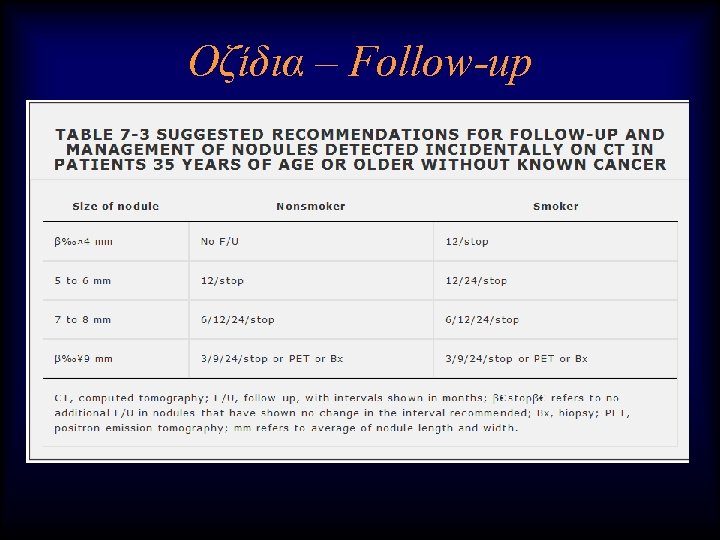
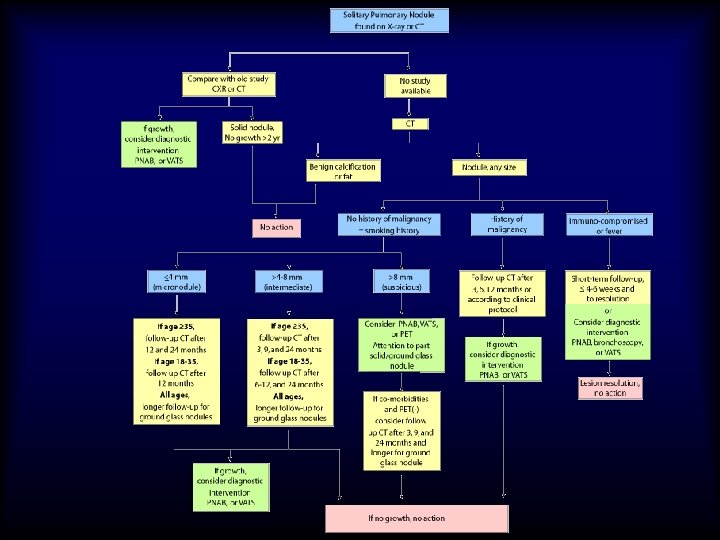
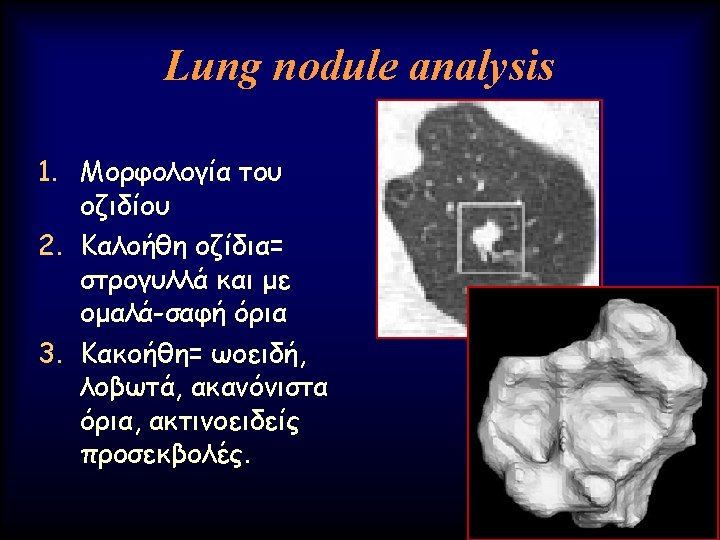
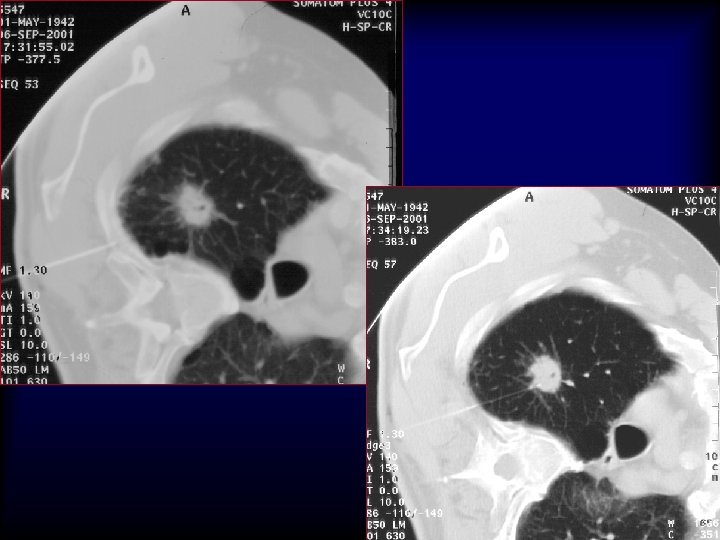
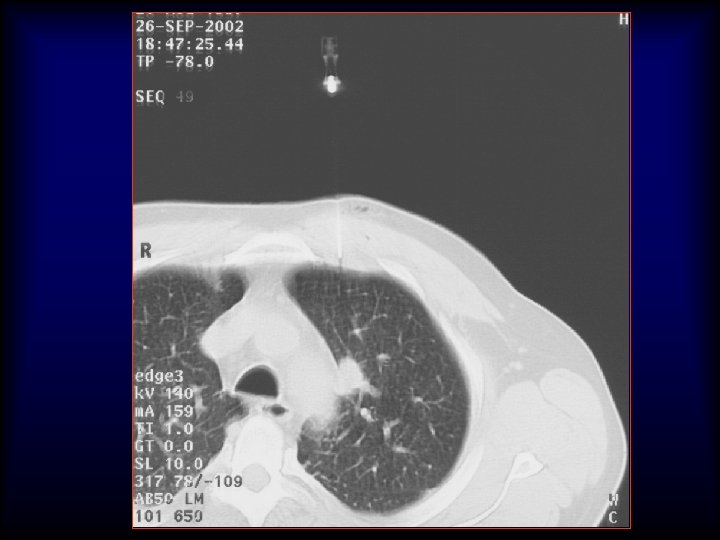
Lung nodule analysis • Evaluating Pulmonary Nodules Pulmonary nodules ≤ 4 mm have a low risk of being cancerous; nodules between 4 -8 mm are of intermediate risk for cancer; follow up CT scans for both categories are recommended on different schedules • Pulmonary nodules >8 mm and mixed solid/ground glass nodules are suspicious for cancer; percutaneous needle aspiration biopsy (PNAB), positron emission tomography (PET), or video assisted thoracic surgery (VATS) should be considered
Advanced Lung analysis 1. Μεταβολή του μεγέθους (Volume) του όγκου Ø Γρήγορο doubling time Authors of a number of other series (20, 21) have confirmed similar findings and have estimated the median tumor doubling times, assuming a constant growth rate to be in the 160– 180 -day range.
Dynamic Contrast Enhanced MRI
Dynamic Contrast Enhanced MRI
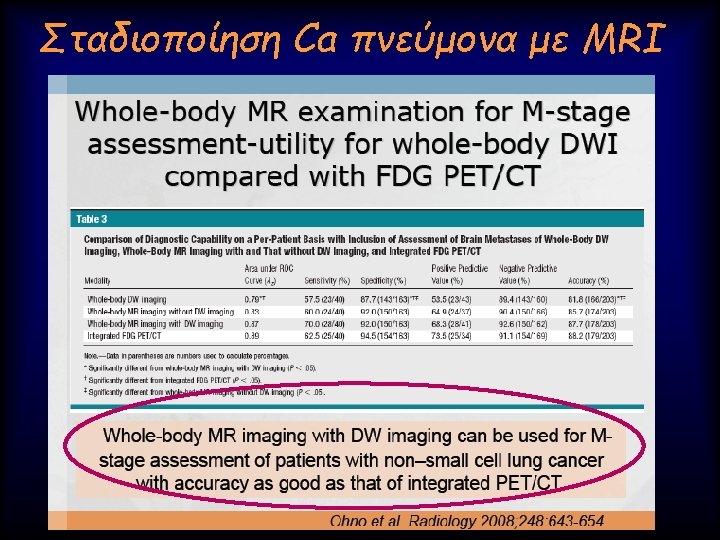
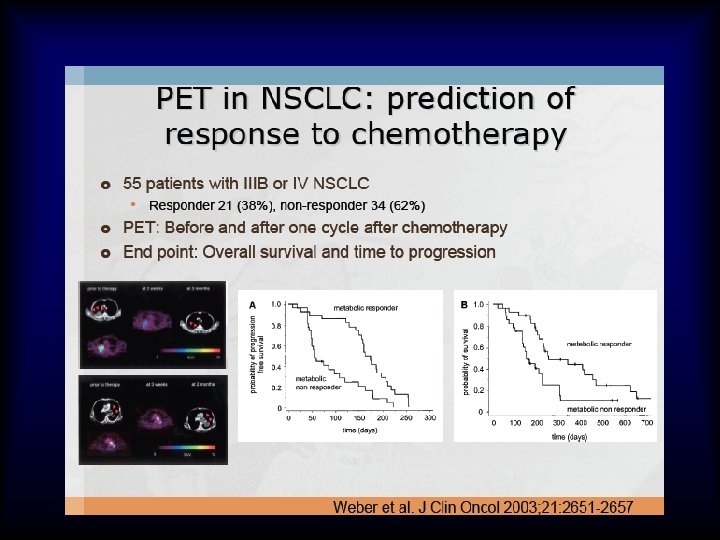
FDG-PET/CT vs 3 T MRI
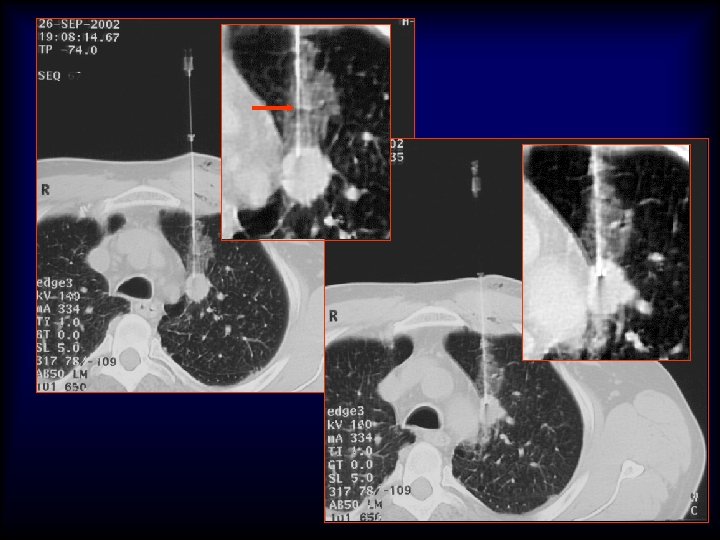
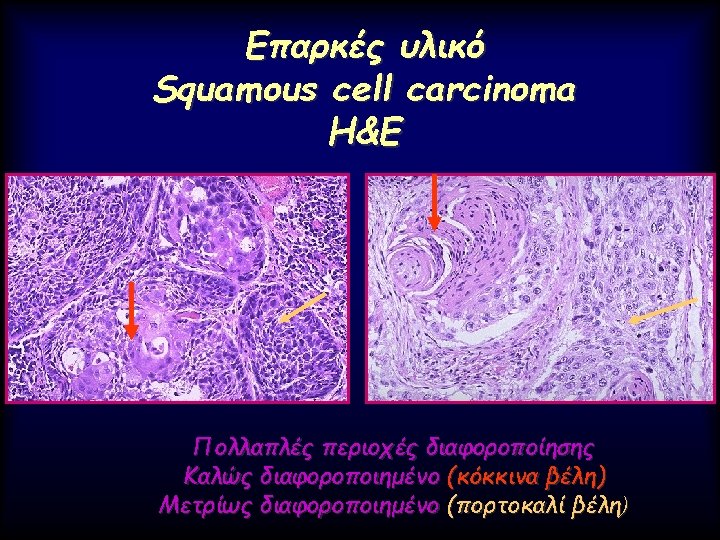
20 G/9 cm/10 T x 25 x 40 x 200 5 mm Adenocarcinoma H&E
Mοριακοί δείκτες που εμπλέκονται στη θεραπεία του Ca πνεύμονα 1. Receptor Tyrosine Kinase Growth Factors Erb. B-1 (EGFR) Erb. B-2 (Her-2/neu) 2. Peptide Growth Factors Neuropeptides 3. Ras, Raf, kit signaling 4. Retinoid Acid Receptor β 5. Eicosanoid pathways Cox-2 6. Apoptotic markers Fas, Bcl-x. L, Bcl-2, Survivin Bax, capsase-3 7. Proliferative markers Rb, p 16, cyclin E Ki-67 8. Angiogenesis markers VEGF, Angiostatin, MMP 2, 9 TIMP 1, 2 Θεραπευτικοί στόχοι Ναι Ναι ? Ναι Ναι Μη σχετιζόμενοι
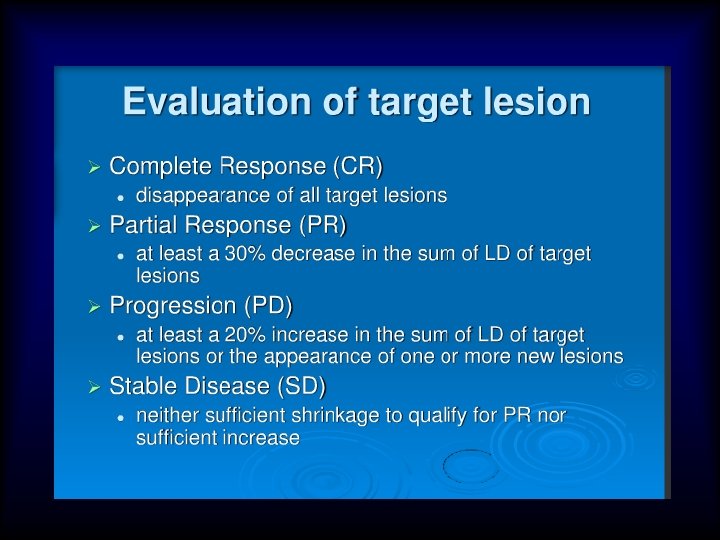
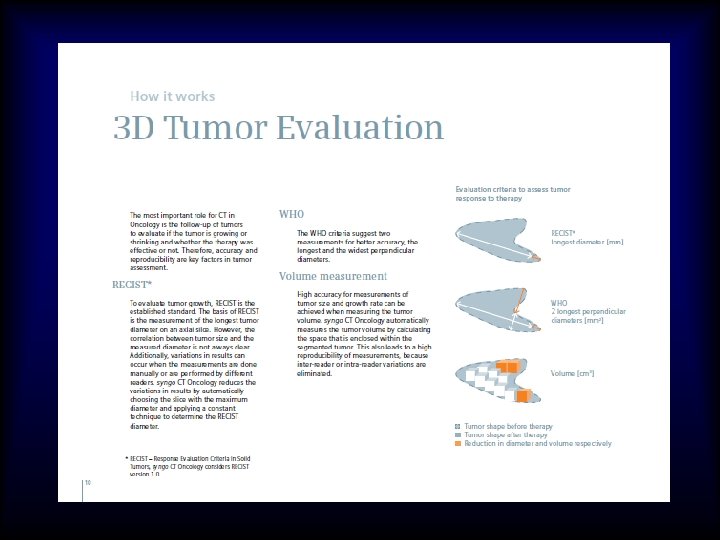
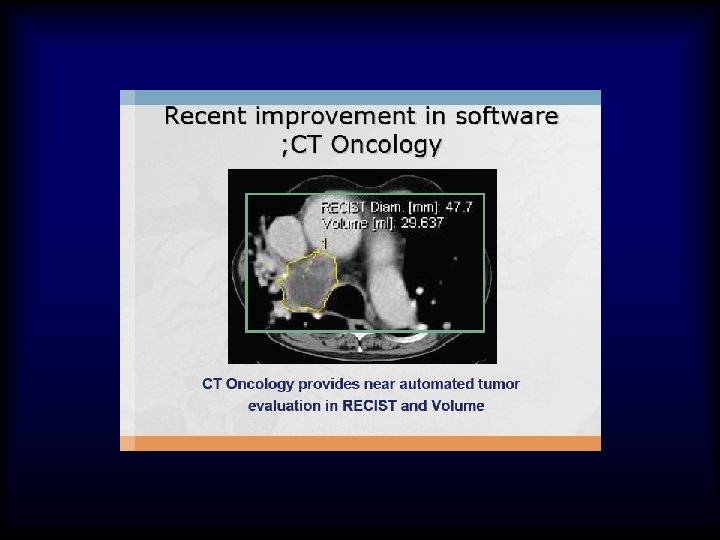
Response Evaluation in Solid Tumors - RECIST
CT perfusion
CT perfusion