Shock Dr R S Gopika M D Hom
 Prof. & Ho. D Department of")



















. The lungs are usually the")




. There will be dilation of proximal")




 Generally associated with septic shock. Endotoxin increases expression of tissue")



- Slides: 46
Shock Dr. R. S. Gopika M. D. (Hom) Prof. & Ho. D Department of Pathology SKHMC
Definition
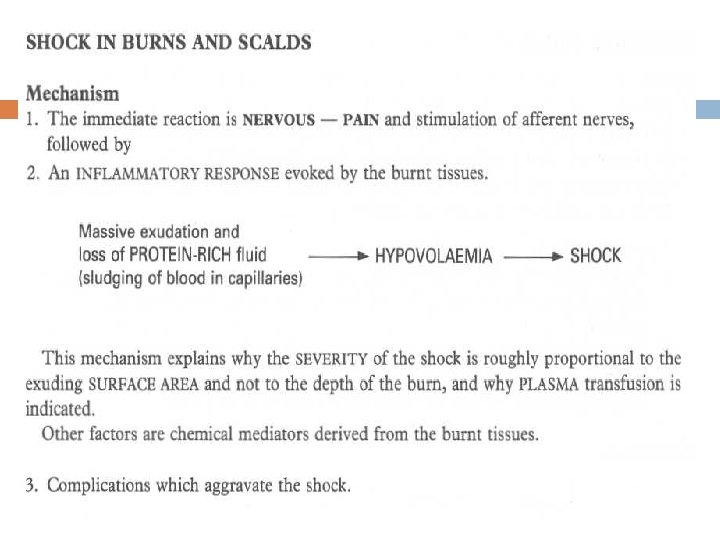
Causes & types HYPOVOLAEMIC SHOCK results from loss of blood or plasma volume -trauma (a) severe haemorrhage-internal/external (b)severe injury (c) burns - dehydration
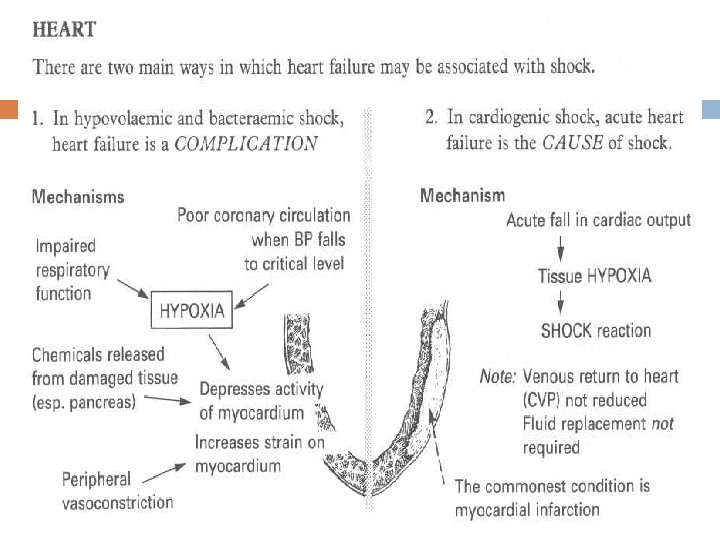
CARDIOGENIC SHOCK Failure of myocardial pump resulting from intrinsic myocardial damage, extrinsic pressure, or obstruction to outflow. Myocardial infarction Ventricular rupture Arrhythmia Cardiac tamponade Pulmonary embolism
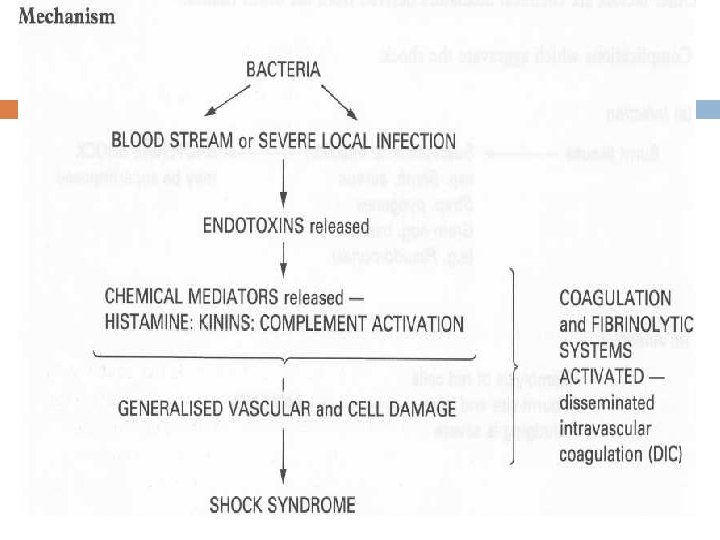
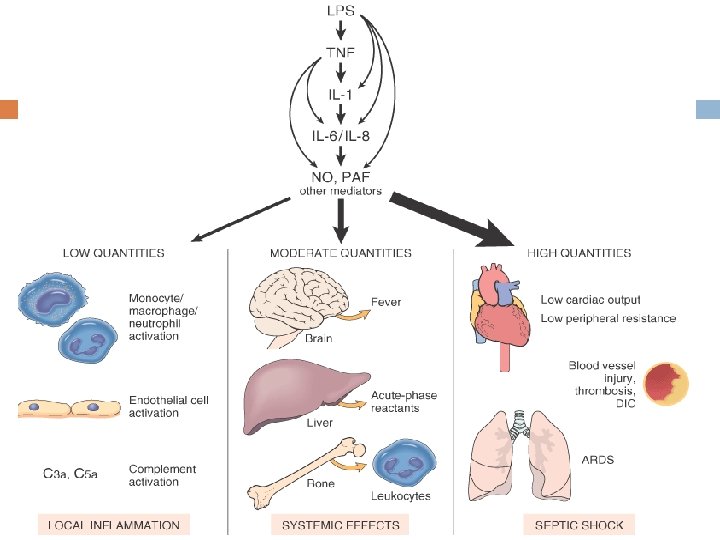
SEPTIC SHOCK Overwhelming microbial infections there need not be systemic bacteremia to induce septic shock; host inflammatory responses to local extravascular infections may be sufficient. Endotoxic shock Gram-positive septicemia Fungal sepsis Superantigens
Special types ANAPHYLACTIC SHOCK Severe immune hypersensitivity reactions Anaphylactic shock represents systemic vasodilation and increased vascular permeability caused by an immunoglobulin E hypersensitivity reaction. In these situations, acute severe widespread vasodilation results in tissue hypoperfusion and cellular anoxia.
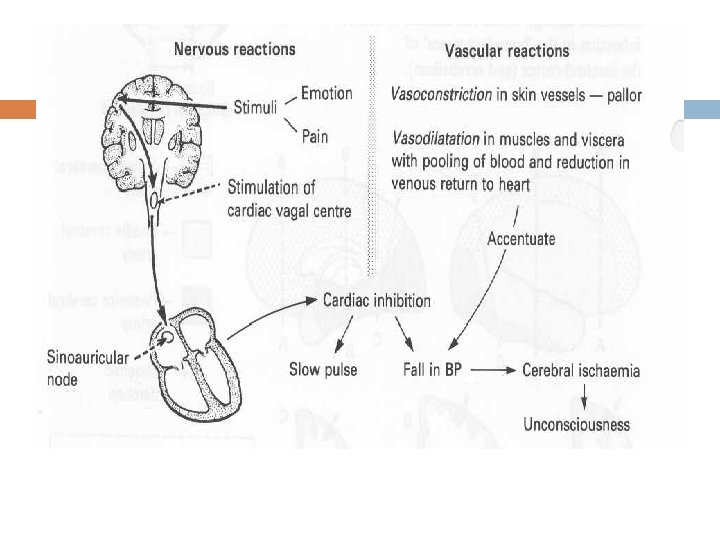
NEUROGENIC SHOCK shock may occur in the setting of an anesthetic accident or a spinal cord injury (neurogenic shock), as a result of loss of vascular tone and peripheral pooling of blood. In special type, acute severe widespread vasodilation results in tissue hypoperfusion and cellular anoxia.
Main consequences of shock Low cardiac output Hypotension Impaired tissue perfusion Cellular hypoxia
Pathogenesis Shock is a progressive disorder that if uncorrected leads to death. Unless the insult is massive and rapidly lethal (e. g. , a massive hemorrhage from a ruptured aortic aneurysm), shock tends to evolve through three general stages
Stages An initial nonprogressive stage during which reflex compensatory mechanisms are activated and perfusion of vital organs is maintained A progressive stage characterized by tissue hypoperfusion and onset of worsening circulatory and metabolic imbalances An irreversible stage that sets in after the body has incurred cellular and tissue injury so severe that even if the hemodynamic defects are corrected, survival is not possible
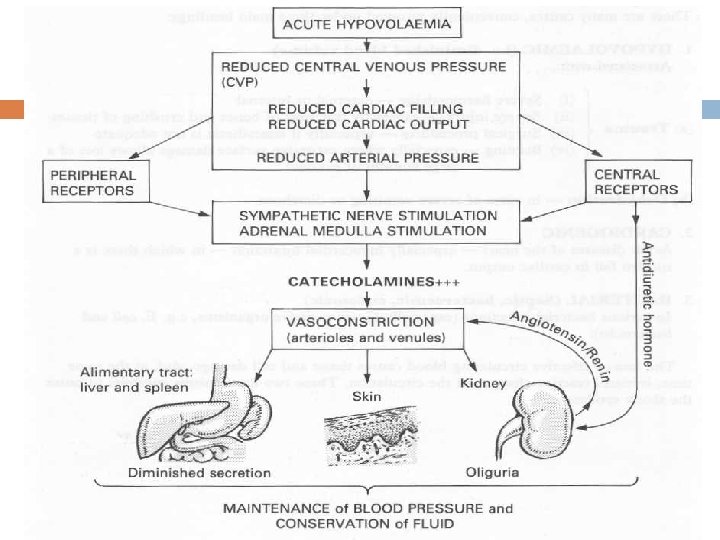
Nonprogressive phase of shock various neurohumoral mechanisms help maintain cardiac output and blood pressure. These include baroreceptor reflexes, release of catecholamines, activation of the renin-angiotensin axis, antidiuretic hormone release, and generalized sympathetic stimulation. The net effect is tachycardia, peripheral vasoconstriction, and renal conservation of fluid. Cutaneous vasoconstriction is responsible for the characteristic coolness and pallor of skin in shock (although septic shock may initially cause cutaneous vasodilation and thus present with warm, flushed skin). Coronary and cerebral vessels are less sensitive to the sympathetic response and thus maintain relatively normal
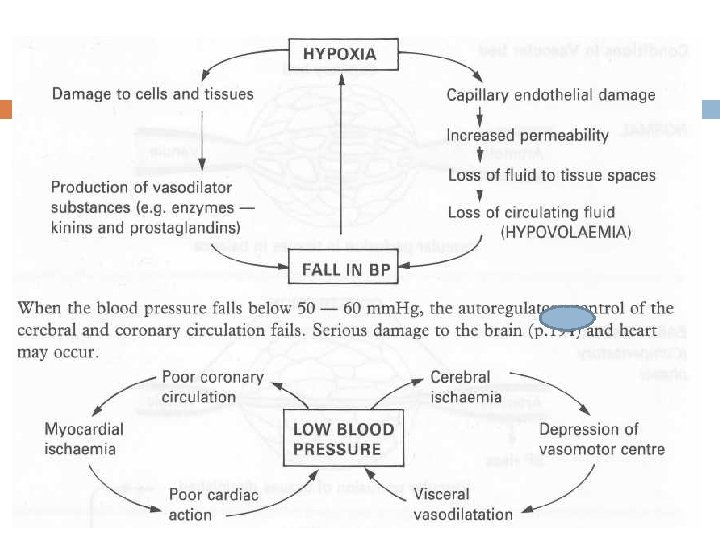
progressive phase If the underlying causes are not corrected, shock passes to the progressive phase, during which there is widespread tissue hypoxia. In the setting of persistent oxygen deficit, intracellular aerobic respiration is replaced by anaerobic glycolysis, with excessive production of lactic acid. The resultant metabolic lactic acidosis lowers the tissue p. H and blunts the vasomotor response; arterioles dilate, and blood begins to pool in the microcirculation. Peripheral pooling not only worsens the cardiac output but also puts endothelial cells at risk of developing anoxic injury with subsequent DIC. With widespread tissue hypoxia, vital organs are affected and begin to fail
irreversible stage Unless there is intervention, the process eventually enters an irreversible stage. Widespread cell injury is reflected in lysosomal enzyme leakage, further aggravating the shock state. Myocardial contractile function worsens, in part because of nitric oxide synthesis. If ischemic bowel allows intestinal flora to enter the circulation, endotoxic shock may also be superimposed. At this point, the patient has complete renal shutdown due to ischemic acute tubular necrosis inevitably culminates in death.
Septic shock
. Hypotension, DIC, and metabolic disturbances constitute the clinical triad of septic shock Septic shock = severe sepsis leading to diffuse vasodilatory hypotension and distributive shock. Common mediators of septic shock include TNF-α, IL 1, NO, and Ceramide is derived from sphingomyelin and mediates inflammatory cascades, including apoptosis. All of these cytokines released during sepsis cause extreme diffuse vasodilation and vascular leakage, leading to distributive shock.
Special type of shock
Pathophysiology of Shock
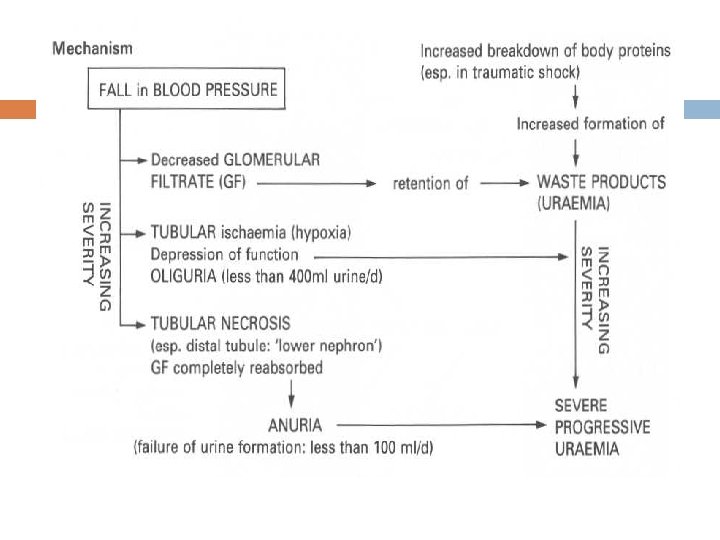
Kidneys Shock causes “pre-renal” acute renal failure. Ischemia of tubule epithelium leads to vasoconstriction, reduced GFR, oliguria, Ischemia leads to Acute Tubular Necrosis (ATN). This may lead to formation of epithelial cell casts, tubule obstruction, back-pressure, and further reduction of GFR.
GI tract The GI tract is at very high risk of infarction. Shock causes infarction of the GI epithelium. The resulting ileus leads to fluid imbalances and acidosis. Liver Centrilobular necrosis is common. There is diminished reticuloendothelial clearance, intrahepatic cholestasis, and elevated bilirubin.
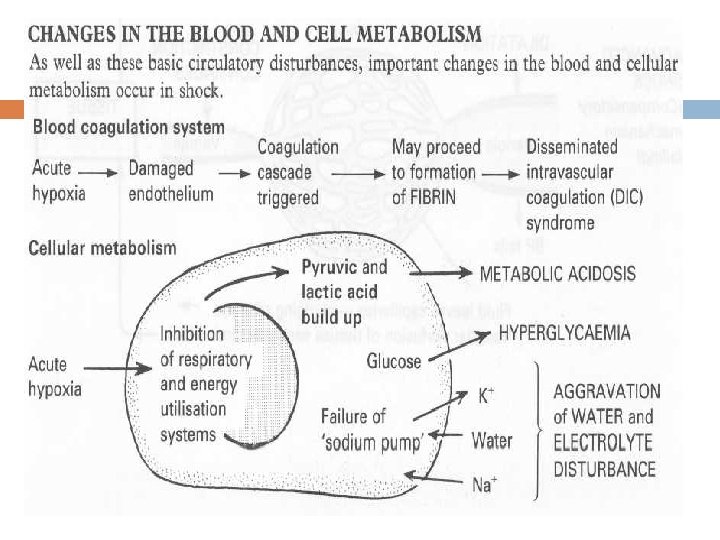
Blood -- DIC WBC count may go up or down. Platelets go way down as they are all used up in DIC. Diffuse fibrin thrombosis consumes feedback inhibitors, leading to more and more clotting. Consumption of clotting factors leads to bleeding (especially from mucosal membranes).
Pathology of Shock leads to multi-organ dysfunction syndrome (MODS). The lungs are usually the first organ to fail, folowed by kidneys, liver, GI tract, and then brain.
Pathology Heart Grossly, subendocardial hemorrhages are common. Microscopically, contraction bands are seen in myocardial cells. Contraction bands are red bands of clumped sarcomeres, most commonly seen after reperfusion injuries, shock, drowning, or other situations of acute ischemia.
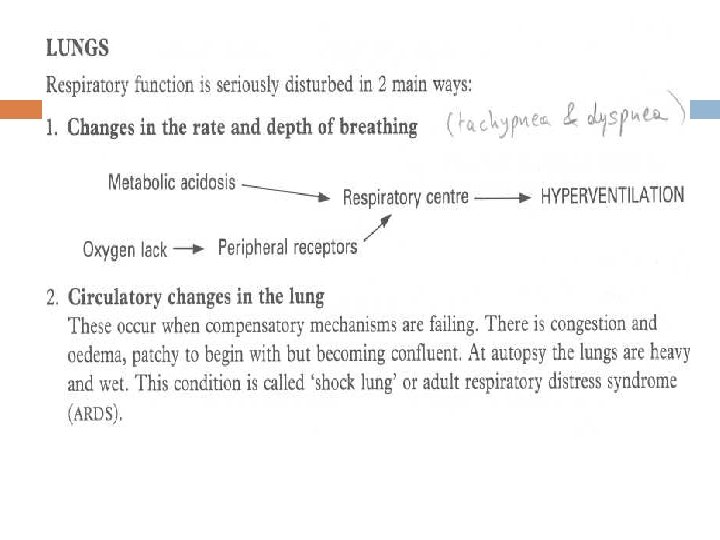
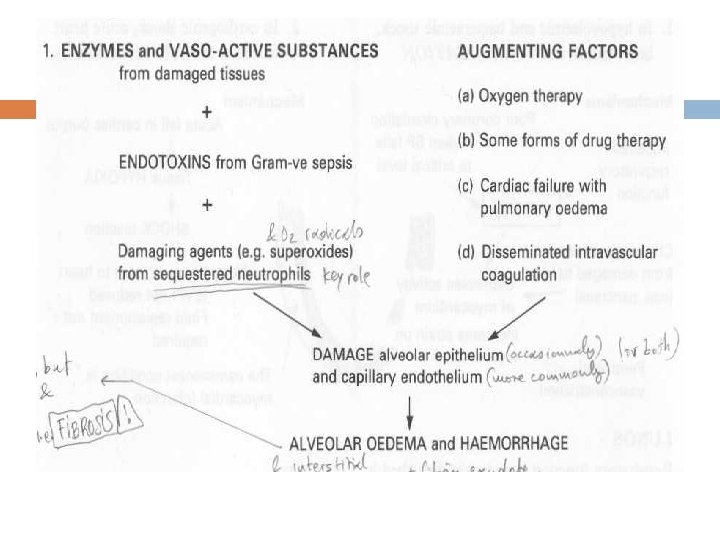
Lung Shock causes release of inflammatory mediators such as TNF-α. This injures endothelial cells. Endothelial injury allows leakage of proteinaceous fluid and neutrophils into the interstitium. This is the interstitial edema and inflammation common in shock. Since it’s interstitial, not alveolar, the septae between alveoli are greatly widened.
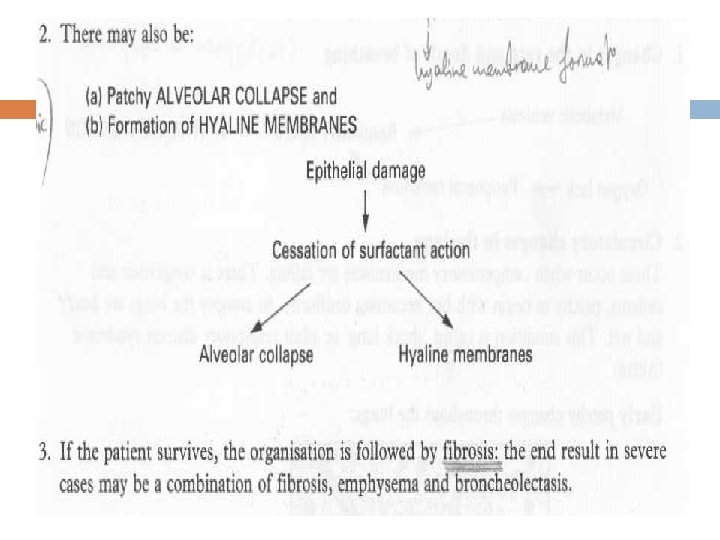
Lung cont…. Lungs become heavy, stiff, and hemorrhagic. Type I pneumocytes and protein are shed into the alveoli, and condense into hyaline membranes. Interstitial fibrosis and chronic respiratory insufficiency may result if the shock is bad
Kidneys The most susceptible kidney cells are those in the proximal tubules and thick ascending Loop of Henle. In shock, the damaged epithelium fails to absorb salt. More salt is delivered to the JGA. Tubuloglomerular feedback causes afferent vasoconstriction, reduced GFR, and oliguria. Damaged epithelial cells may also shed into tubules and aggregate into casts, which exert back-pressure on the glomerulus and further reduce GFR.
Kidney cont…. Microscopically, - acute tubular necrosis (ATN). There will be dilation of proximal tubules due to flattening of the epithelium. Brownish casts may be seen. Glomeruli will look normal, and inflammation is minimal. ATN is generally reversible.
Brain Watershed infarcts are a common consequence of shock. These are long, wedge-shaped infarcts at the very distal tips of a major arterial supply. Laminar necrosis is another common consequence of shock. These lesions trace the surface topology, and represent death of deeper cortical gray matter which is supplied by short penetrating arteries. The most vulnerable neurons are pyramidal cells in hippocampus and cortical layers 3/5, and cerebellar Purkinje cells.
GI tract Shock often causes mucosal hemorrhage and necrosis. This may result in septicemia. Severe shock can denude whole sections of mucosa down to the lamina propria. Grossly, the GI tract may appear swollen and bloody
Liver Shock generally causes centrilobular necrosis, because the hepatocytes closest to the central vein are the furthest from the blood supply. Ischemic injury to the liver is generally reversible. Pancreas The pancreas may also experience ischemic injury, causing leakage of enzymes and acute pancreatitis.
Adrenals Shock may cause hemorrhage and lipiddepletion of the adrenal cortex. Waterhouse-Friderichsen Syndrome is massive bilateral adrenal hemorrhage and shock caused by meningococcal septicemia. Usually fatal.
Disseminated Intravascular Coagulation (DIC) Generally associated with septic shock. Endotoxin increases expression of tissue factor, which activates the common coagulation cascade. Ischemic injury to endothelial cells exposes the ECM, which initiates platelet aggregation. Platelets and anti-thrombin become depleted, so in addition to all of the coagulation and fibrin thrombi being formed, patients may also have bleeding and mucosal hemorrhages.
The clinical manifestations of shock depend on the precipitating insult. In hypovolemic and cardiogenic shock, the patient presents with hypotension; a weak, rapid pulse; tachypnea; and cool, clammy, cyanotic skin. In septic shock, the skin may be warm and flushed as a result of peripheral vasodilation. The initial threat to life stems from the underlying cause that precipitated the shock state (e. g. , a myocardial infarct, severe hemorrhage, or bacterial infection).
c/f the cardiac, cerebral, and pulmonary changes that occur secondary to the shock state materially worsen the problem. If patients survive the initial complications, they enter a second phase, dominated by renal insufficiency and marked by a progressive fall in urine output as well as acidosis, and severe fluid and electrolyte imbalances
THANK YOU