Treatment of Cardiogenic Shock in the Community Setting


")








")






 Inflow (ventricle) aortic valve Flow")

Data,")
Data, AMI/CGS Apr")








 100% 87% 90% 80% 67% 65% 70%")



- Slides: 37
Treatment of Cardiogenic Shock – in the Community Setting Farhan J. Khawaja MD, FACC, FSCAI, RPVI
OUTLINE • • Definition of Cardiogenic Shock Epidemiology- A Call to Action Treatment of Cardiogenic Shock Advances in the Treatment of Cardiogenic Shock
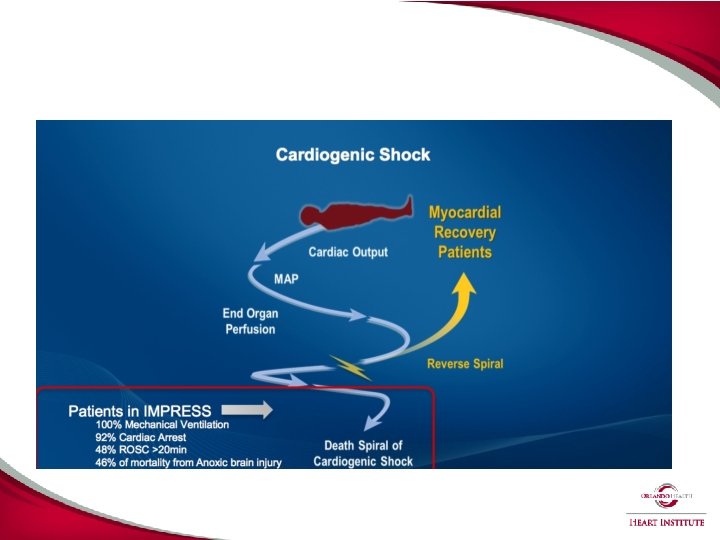
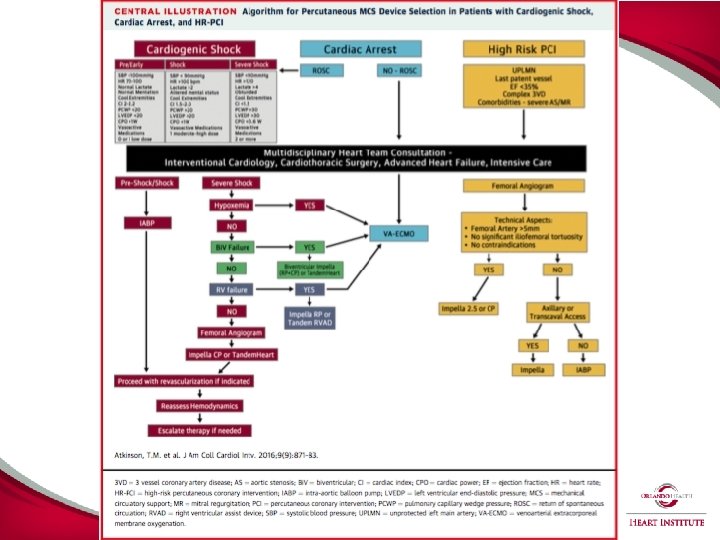
Cardiogenic Shock Atkinson (J Am Coll Cardiol Intv 2016; 9: 871– 83)
4 INCIDENCE OF CARDIOGENIC SHOCK GROWING Cardiogenic Shock in STEMI Increasing 1 STEMI Cardiogenic Shock in Medicare Age Increasing 2 Cardiogenic Shock (%) 56, 508 36, 969 53% 2010 2014 Age >65 only, excludes non-Medicare population 1. Dhaval Kolte et al. J Am Heart Assoc 2014 NATIONWIDE INPATIENT SAMPLE 2. Centers for Medicare and Medicaid database, MEDPAR FY 14
5 CARDIOGENIC SHOCK REMAINS LEADING CAUSE OF MORTALITY IN ACUTE MYOCARDIAL INFARCTION High In-Hospital Mortality During AMI Cardiogenic Shock 1 … and Ongoing Hazard Post Discharge after AMI Cardiogenic Shock 2 N = 23, 696 N = 112, 668 % 100 Mortality % Post Discharge 90 Death Rate, % 80 70 60 50 40 30 20 10 0 2001 2002 1. Jeger, et al. Ann Intern Med. 2008 2. Shah, et al. JACC 2016 NCDR Registry 2003 2004 2005 2006
MORTALITY IN PCI WITH CARDIOGENIC SHOCK REMAINS A CLINICAL CHALLENGE In-Hospital Mortality AMI Cardiogenic Shock with PCI 1 N = 32, 598 31% 28% p<0. 0001 11% 2005 -2006 2011 -2013 AMI Cardiogenic Shock with PCI only; Overall mortality >50% Wayangankar, et al. JACC Int 2016 CATH-PCI Registry 6
AMI SHOCK OFTEN TREATED IN COMMUNITY HOSPITALS AMI Cardiogenic Shock with PCI N = 56, 497 2005 -06 90% Private/Community 2011 -13 69% 52% 48% 31% 10% Wayangankar et al. JACC Interventions 2016 CATH-PCI REGISTRY Academic/ Gov’t >500 PCI <500 PCI 7
Treatment of Cardiogenic Shock • Revascularization
The 2011 Guideline for PCI Class I • PPCI should be performed within 12 hours of onset of STEMI (LOE = A) • PPCI should be performed in patients with STEMI who develop severe heart failure or cardiogenic shock and are suitable candidates irrespective of the time delay (LOE = B) Class I • PPCI is recommended in patients with acute MI who develop cardiogenic shock and are suitable candidates (LOE = B) Levine GN, et al. J Am Coll Cardiol 2011; 58: e 44 -122.
ESC Guidelines 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation: The Task Force for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2017; Aug 26:
Primary Study Endpoint All-Cause Mortality or Renal Replacement Therapy 60 Immediate multivessel PCI All-cause mortality or renal replacement therapy (%) 55. 4% Culprit lesion only PCI 50 45. 9% 40 30 20 10 Relative risk 0. 83; 95% confidence interval 0. 71 -0. 96; P=0. 01 0 0 5 10 15 20 25 30 Days after randomization Number at risk: Culprit lesion only PCI 344 219 207 198 192 189 184 Immediate multivessel 341 PCI 199 172 162 156 153 152
Mechanical Circulatory Support Atkinson (J Am Coll Cardiol Intv 2016; 9: 871– 83)
13 IABP IN AMI CARDIOGENIC SHOCK: NO HEMODYNAMIC OR SURVIVAL BENEFIT IABP SHOCK I Randomized Controlled Trial 1 N = 40 IABP (n=19) Medical Therapy (n=21) IABP-SHOCK II Randomized Controlled Trial 2 N = 600 IABP (n=301) Medical Therapy (n=299) 41. 3% 39. 7% CPO = MAP x Cardiac Output x 0. 0022 log-rank, p=0. 92 IABP Increased hazard risk of stroke, downgraded to Class III (harm), Level of Evidence A, ESC STEMI Guidelines 2014 1 - Prondzinsky R. et al. Jn Critical Care Medicine IABP SHOCK I 2010 – Clinicaltrial. gov # NCT 00469248 2 - Thiele H et al. NEJM 2012 - Clinicaltrial. gov # NCT 00491036
1414 NEW CARDIOGENIC SHOCK INDICATED THERAPY: IMPELLA
15 FDA INDICATION The Impella 2. 5™, Impella CP , Impella 5. 0 ™ and Impella LD ™ catheters, in conjunction with the Automated Impella Controller console, are intended for short-term use (<4 days for the Impella 2. 5 and Impella CP and <6 days for the Impella 5. 0 and Impella LD) and indicated for the treatment of ongoing cardiogenic shock that occurs immediately (<48 hours) following acute myocardial infarction (AMI) or open heart surgery as a result of isolated left ventricular failure that is not responsive to optimal medical management and conventional treatment measures with or without an intraaortic balloon pump. ® The intent of the Impella system therapy is to reduce ventricular work and to provide the circulatory support necessary to allow heart recovery and early assessment of residual myocardial function. * Optimal medical management and conventional treatment measures include volume loading and use of pressors and inotropes, with or without IABP
16 Protected PCI Cardiogenic Shock DATA SUPPORTING FDA INDICATIONS Scientific Evidence Total # of Patients # of Impella Patients Recover I FDA Study 17 17 ISAR Shock RCT 26 13 U. S. Impella Registry 401 Literature review 2, 537 692 Total 2, 981 1, 123 Protect I FDA Study 20 20 Protect II FDA Study 452 225 U. S. Impella Registry 1, 322 637 Literature review 2, 537 756 Total 4, 331 1, 638 24, 000 Patients from FDA medical device reporting (MDR) database
17 RANDOMIZATION IN AMI CS IS CHALLENGING Prospective Impella Trials In Emergent Settings Study Trial ID Pts Duration Condition Required Enrolled (months) (n) Status Reason for Discontinuation NCT 0031484 7 AMI CS 200 19 52 ISAR-SHOCK (2006) NCT 0041737 8 AMI CS 26 26 19 IMPRESS (2007) NTR 1079 trialregister. nl STEMI Pre-CS 130 18 22 NCT 0059672 6 PCCS Up to 20 17 28 NCT 0097227 0 AMI CS 384 1 18 Discontinued Low Enrollment RELIEF I (2010) NCT 0118569 1 ADHF 20 1 33 Discontinued Low Enrollment DANSHOCK (2012) NCT 0163350 2 AMI CS 360 ~50 40 FRENCH TRIAL (2006) RECOVER I FDA (2008) RECOVER II FDA (2009) Discontinued Low Enrollment Completed N/A Discontinued Low Enrollment Completed Enrolling N/A
POPULATION STUDIES SHOW REDUCED MORTALITY WITH PVAD IN AMI CARDIOGENIC SHOCK Mortality AMI Cardiogenic Shock Pre/Post PVAD Era 52% Mortality In AMI Cardiogenic Shock ECMO/e. LVAD vs. PVAD 56% p=0. 012 p<0. 001 43% 42% N=1188 Co-morbidity Matching N=11, 887 2004 - 2007 2008 - 2011 No PVAD Era Stretch, et. al JACC 2014 National Inpatient Sample Maini, et. al. CCI, 2014 and SCAI/ACC/STS /HFSA Expert Consensus Document Surgical MCS PVAD 18
HEMODYNAMIC EFFECTS OF IMPELLA SUPPORT ® Outflow (aortic root) Inflow (ventricle) aortic valve Flow LVEDP and LVEDV MAP Wall Tension Mechanical Work Microvascular Resistance Coronary Perfusion Cardiac Power Output End Organ Perfusion O 2 Supply O 2 Demand Unloading to Myocardial Recovery Fincke J, et al. Am Coll Cardiol 2004 Suga H. et al. Am J Physiol 1979 Sauren LDC, et al. Artif Organs 2007 Reesink KD, et al. Chest 2004 den Uil CA, et al. Eur Heart J 2010 Suga H, et al. Am J Physiol 1981 Meyns B, et al. J Am Coll Cardiol 2003 Valgimigli M, et al. Catheter Cardiovasc Interv 2005 Mendoza DD, et al. AMJ 2007 Burkhoff D. et al. Am J Physiol Heart Circ 2005 Remmelink M, et al. atheter. Cardiovasc Interv 2007 Remmelink M. et al. Catheter Cardiovasc Interv 2010 Torgersen C, et al. Crit Care 2009 Burkhoff D. et al. Mechanical Properties Of The Heart And Its Interaction With The Vascular System. (White Paper) 2011 Aqel RA, et al. J Nucl Cardiol 2009 Naidu S. et al. Novel Circulation. 2011 Lam K, . et al. Clin Res Cardiol 2009 Weber DM, et al. Cardiac Interventions Today Supplement Aug/Sep 2009 Torre-Amione G, et al. J Card Fail 2009 19
IMPRESS Dagmar M. Ouweneel et al. JACC 2017; 69: 278 -287
National Variation in Impella AMI/CGS Outcomes 1. 2. Data on file. Abiomed Impella Quality(IQ)Data, AMI/CGS Apr 2015 – Mar 2016. Danvers, MA: Abiomed. Greater than 90% of survivors were explanted with native heart recovery
Improvement in National Outcomes 1. 2. Data on file. Abiomed Impella Quality(IQ)Data, AMI/CGS Apr 2016 – Sept 2017. Danvers, MA: Abiomed. 525 sites supporting >6 AMICS patients, 7, 483 patients total since March 2016
RV SUPPORT Shishehbor CCJM 2017
STANDARDIZED APPROACH • Protocol • Early Initiation of Hemodynamic Support • Hemodynamic Monitoring
IMPELLA PRE
HEMODYNAMIC MONITORING
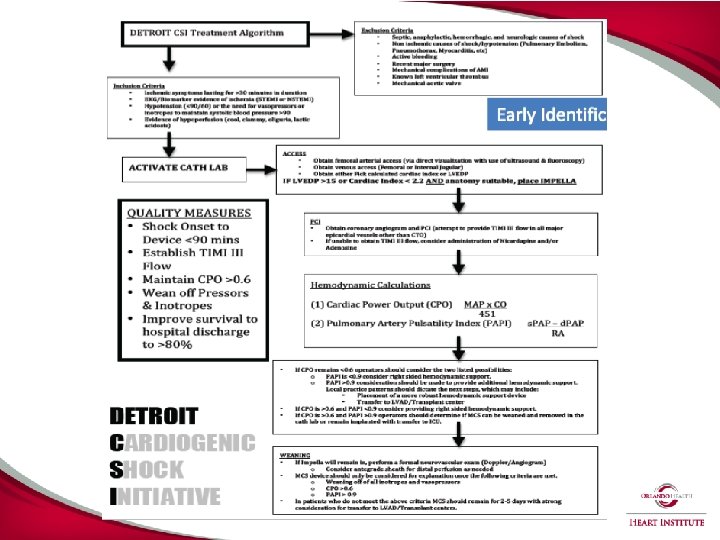
DETROIT CSI INITIATIVE
Orlando Health Cardiogenic Shock Protocol
Orlando Health Cardiogenic Shock Protocol
Orlando Health Cardiogenic Shock Protocol
Orlando Health Impella Survival to Discharge (AMI/CGS) 100% 87% 90% 80% 67% 65% 70% 58% 50% 40% 30% 11/19 11/17 13/15 4/6 ORMC HC DPH SLK 20% 10% 0%
Registry Outcomes Muharrem Akin et al. JCIN 2018; 11: 1811 -1820
Registry Outcomes Muharrem Akin et al. JCIN 2018; 11: 1811 -1820
Conclusion • Cardiogenic Shock remains lethal • Early Revascularization improves survival • Mechanical Circulatory Support is redefining the treatment paradigm • Protocol Driven Approaches are promising