Shock Shawn Dowling PGY5 Objectives Briefly discuss general

Shock Shawn Dowling, PGY-5

Objectives Briefly discuss general pathophysiology Classification of shock Review of vasopressors Lots of cases We will not talk about septic shock - this will be discussed in a future set of rounds

Intro 35 M. Pulled from an industrial fire. Brought in by EMS. Pt is awake, but clearly altered. Only complaint is a HA. Prev well. T 37, HR 110, BP 160/70, RR 20/100% c/s 7 The nurses have already drawn a venous gas CO is 18%, lactate is 13 Is this patient in shock?

What do you think is going on? Lactate > 10 is highly predictive of cyanide toxicity with inhalational exposure regardless of CO level Baud FJ, et al: Elevated blood cyanide concentrations in victims of smoke inhalation. N Engl J Med 2001; 325: 1761– 1766. How do you want to treat this patient other than with O 2 +/- hyperbarics? Why? Only give the sodium thiosulfate portion of the Cyanide Antidote Kit – if you give them the nitrite component you induce more of a functional anemia which they will not tolerate because of the other functional anemia – the CO

Definition of shock Rude unhinging of the machinery of life Or The inability of the circulatory system to adequately supply tissues with 02 & nutrients and remove cellular waste

Diagnosis of Shock – Rosen’s Need 4 of 6 Ill appearance or decreased LOC (as a general rule MAP< 50 before AMS) HR > 100 RR > 22 or PC 02 < 32 Base deficit <-5 or lactate >4 Urine output < 0. 5 ml/kg/hr Hypotension > 20 minute duration NOTE - ↓BP not required for Dx

Diagnosing Shock The more advanced the shock state, the easier the Dx, but… Significant tissue hypoxia appears to exist prior to development of significant signs & symptoms THE BETTER WE CAN RECOGNIZE SHOCK, THE EARLIER WE CAN INSTITUTE Tx TIME IS TISSUE (see RIVERS STUDY) Can be is shock with “normal” vitals Normal BP in face of hypovolemia means some organs are hypoperfused to maintain systemic BP

Shock is the transition between life and death

Shock unifying features: Imbalance between cellular O 2 demand supply Disrupted cellular homeostasis Failed aerobic metabolism –> anaerobic metabolism –> lactic acidosis Calcium shifts - impairs cardiac contractility Failed ion gradients and cellular pumps Cell edema and death

How does our body compensate? Counter-regulatory mediators Catecholamines, glucocorticoids, angiotensin, vasopressin, insulin Increased substrates glucose, TG and FFA Anaerobic metabolism incr CO 2: 02 ratio

Pertinent Critical Care formulas CO = HR x SV BP = CO x SVR O 2 content = 1. 34 x hgb x O 2 saturation + 0. 003 x Po 2 (02 bound to hgb) (02 in plasma) Oxygen delivery is the CO x O 2 content Why is this equation so important to a shock talk? In which shock scenario do we target the O 2 in plasma for treatment? CO poisoning

What are some different shock classifications?

Classification of Shock Many different ways Mnemonics Physiologic Clinical It doesn’t matter which you use as long as You know it cold It’s exhaustive

Shock BP = ↓CO x ↓SVR Hypovolemic Cardiogenic Obstructive Distributive

Shock Hypovolemic Cardiogenic Bleeding or Fluid Loss • Overt • Occult • Excessive Losses • Vessels • Rhythm • Valvular • Myocardium • Pericardium Obstructive • Intravascular • Extravascular Distributive NASTE Neurogenic Anaphylactic Septic Toxicologic Endocrine

Hypovolemic Overt/Occult losses of blood 5 sources of life threatening hemorrhage in trauma? Chest, Abdo, Pelvis, Long bones, Street (from skin) Excessive Fluid loss 3 rd spacing (burns, pancreatitis, dermatologic, ascites) Excessive sweating/vomiting/diarrhea/urine output(diuretics, DI)

Cardiogenic Vessels AMI or acute or chronic– usually need to infarct 40% to cause shock Ao. D Rhythm Brady Tachydysthrythmias Valvular Stenosis Regurgitation Myocardium Rupture (FW or VSD) Myocarditis Cardiomyopathy RV involvement Pericardium Tamponade

Obstructive Intravascular PE Amniotic Fluid Embolism Air embolism Fat embolism Extravascular Tension PTX Cardiac tamponade SVC syndrome
, CO, cyanide, iron, ASA, etc Endocrine")
Distributive Neurogenic Anaphylactic Septic Toxicologic (Ca. CB, BB), CO, cyanide, iron, ASA, etc Endocrine Adrenal insufficiency, thyroid storm, electrolytes (hyper. K)

Top three causes of shock in infants Sepsis Hypovolemic Cardiac SHOCK in a neonate Sepsis Cardiac non-Accidental Trauma Metabolic Surgical

Physical Exam Two purposes 1. Try to determine if the patients is in shock – Look for evidence of end organ damage 2. Determine the cause of the shock – JVP & perfusion status is VERY helpful

Thanks to ICU Crash Course

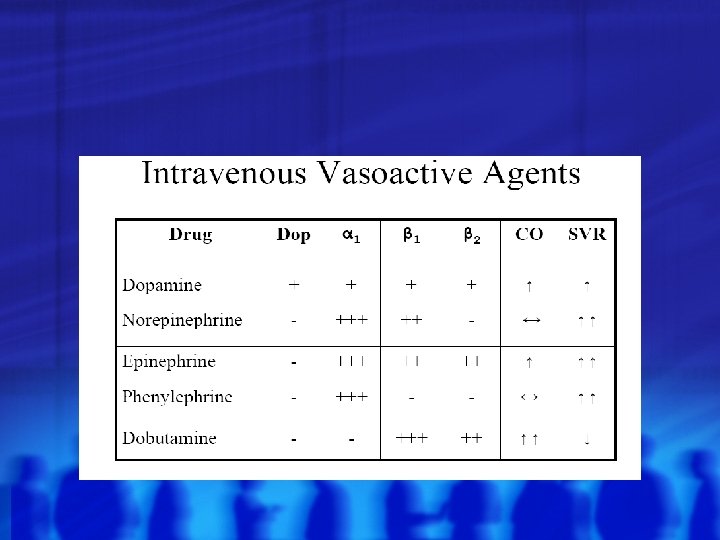
Match the shock with the appropriate vasopressor and why Sepsis Neurogenic Shock Anaphylactic Shock Epinephrine Ephedrine Phenylephrine Norepinephrine Dopamine Milrinone

Direct vs indirect vasopressors Direct agents stimulate the receptor directly Indirect agents have their effect by stimulating the adrenals to release catecholamines : . If stressor has been ongoing for a period of time -> body’s catecholamine reserve is likely deplete and the indirect agents will have less effect Direct Norepi Epi Phenylephrine Indirect Dopamine Dobutamine Ephedrine

Receptor Primary location Primary fx α ß 1 ß 2 D D=Dopaminergic

Receptor Primary location Primary fx α Vessel walls Peripheral Arterial Constriction ß 1 Heart Inotropy/Chronotropy ß 2 Lungs/Skeletal muscle Dilatation of smooth muscle (skeletal and bronchial) D Kidneys Increase renal blood flow D=Dopaminergic

 Feb. 11, 2005. § § For all kinds of shock RCTs")
Cochrane Review: (updated) Feb. 11, 2005. § § For all kinds of shock RCTs § § § Levo + dob vs epi (2 studies, N=52) § § Levo vs Dop (3 studies, N=62) RR death 0. 88 (0. 57, 1. 36) RR death 0. 98 (0. 57, 1. 67) Unfortunately, these studies are too small to definitively answer the question but better data to support that norepi achieves HD endpoints better and since it’s a direct agent likely better for septic patients

Case 1 PP: 8 yo F with known allergy to wasps PMHx: Healthy and no meds HPI: At day camp and “forgot” her epi-pen Stung by 2 hornets after accidentally running into a nest Presents by personal vehicle to ED Given PO Benadryl by family member

Case 1 Generally Appears unwell and flushed HR=128, RR=38, T=37. 8, BP=85/40, Sat 89% RA CVS Tachy, warm extremities Resp Significant indrawing Audible wheeze throughout No stridor noted Derm Urticarial rash and diffuse flushing ENT Lip swelling noted and uvula swollen on exam
 Name the general category of shock 2) Describe the pathophysiology 3)")
Case 1 1) Name the general category of shock 2) Describe the pathophysiology 3) Name the management goals 4) Define the best interventions to obtain the above goals 5) Name potential pitfalls

Case 1 The pediatric nurse is panicked…. . He wants to know how much Epinephrine you want to give this child and by what route…. .

Case 1 The patient is not responding to your IM epinephrine The pressure is 60 systolic and the patient has become obtunded…. .

Case 2 PP: 58 yo Male with known shrimp allergy PMHX MI 2 years ago NIDDM HTN HPI: Ate the “egg roll special” at a Thai restaurant Immediate throat swelling EMS called and IM epinephrine given on route

Case 2 Generally Appears flushed and unwell with marked work of breathing and distress HR 62, RR 28, BP 80/46, Sat 89% on mask, T 37. 4 CVS Normal heart sounds, normal cap refill Resp Diffuse wheeze throughout Abdomen Soft but mildly tender Neuro Starting to appear somnolent

Case 2 You repeat another IM injection of 0. 3 cc of 1: 1000 epi and give H 1 and H 2 blockers intravenously There is no improvement and the patient remains hypotensive and relatively bradycardic…. .
 Name the general category of shock 2) Describe the pathophysiology •")
Case 2 1) Name the general category of shock 2) Describe the pathophysiology • Difference between anaphylaxis and anaphylactoid? 3) Name the management goals 4) Define the best interventions to obtain the above goals 5) Name potential pitfalls

Management Fluids Meds Epi is the first line Tx for anaphylaxis IV (1: 10, 000) 1 m. L (100 ug) aliquot – repeat q 60 sec until desired effect Infusion - 1 ug/min-4 ug/min If pt not in shock – IM (why not SC? ) Ventolin nebs Benadryl 50 mg IV Zantac 50 mg IV Solu-medrol 125 mg IV
 1 -2 mg IV Then 5 -15")
Glucagon (for pts on ßß, ? ACE-I) 1 -2 mg IV Then 5 -15 mcg/min infusion Inotropic/chronotropic/vasoactive properties beyond the b-receptor

Case 3 80 M. Hx of COPD. Presents with productive cough and feels unwell. T-40, RR 28, sats 85% on NRB, HR-120, BP 90/50 Working Dx – Pneumonia + Sepsis You decide you going to intubate this patient because of failure to oxygenate Any concerns? How are you going to prepare? Induction agent? Other meds?

Sepsis and airway management Sepsis significantly increases you O 2 requirements – therefore these patients can desaturate quite rapidly – : . Optimize the conditions (i. e. positioning, pre-oxygenate, best-intubator, etc) Use of accessory muscles can ↑O 2 consumption by 50 -100%! Another reason to manage their airway early or if you are not meeting your physiologic end points Any other concerns

Post-intubation hypotension Septic patients are very catecholamine driven – intubating can remove that stimuli and they can drop their pressures precipitously Also, the agents we give for intubation may play a role ↑ intra-thoracic pressure (from mechanical ventilation) can drop the preload : . causing hypotension)

Intubating a septic patient Pre-oxygenate as much as possible Pretreat with fluids +/- bicarb if you thing they are really acidotic (no evidence) Careful choice of induction agent Ketamine or ½ dose etomidate (0. 15 mg/kg) are likely best options, AVOID propofol Have some pressors drawn up (phenyl/norepi) Why not dopamine or ephedrine? phenylephrine How do you mix this? 10 mg in 100 m. L bag – draw up 10 cc and give 1 cc(100 Ug)/dose RSI if no CI (gives you the best look)

http: //ca. youtube. com/watch? v=p. Y 8 ja. G s 7 x. J 0

Case 3 PP: 38 yo Male transfer by STARS Pm. Hx: Asthma but otherwise healthy Meds: Ventolin and Flovent PRN HPI: Patient riding QUAD in kananaskis country and flipped + Helmet and no LOC Trapped under bike for 10 minutes extrication by friends STARS scene call No major blood loss noted on scene

Case 3 Generally GCS 12/15 patient confused and aggitated HR 120, BP 81/40, RR 15, Temp 37. 2, Sats 92% CVS Tachycardic, normal HS, Cap refill 4 seconds, weak thready pulse Resp Clear bilaterally but poor inspiratory effort Abdomen Diffusely tender to palpation Soft and not distended MSK Pelvis is grossly unstable to palpation Perineal hematoma noted Femurs and hips normal to exam Neuro PEARL, No signs of depressed skull or basal skull injury No signs of head trauma

 Name the general category of shock 2) Describe the pathophysiology 3)")
Case 3 1) Name the general category of shock 2) Describe the pathophysiology 3) Name the management goals 4) Define the best interventions to obtain the above goals 5) Name potential pitfalls

Case 3 You do a ED FAST and it is negative for free fluid in the abdomen What do you want to do now?

Case 4 68 yo Male with known small cell lung Ca Meds: Undergoing outpatient chemotherapy and radiotherapy at TBCC for last 2 months HPI: 3 day history of dyspnea, apprehension and mild chest pain Presents today feeling very unwell, presyncopal and markedly short of breath on minimal exertion

Case 4 Generally Appears unwell and dyspneic, markedly diphoretic HR 119, RR 24, BP 90/55, Sat 98% RA, Temp 36. 9 CVS Faint HS appreciated, normal S 1 S 2 and no EHS Extremities cool and cap refill 3 -4 seconds, +mottled Peripheral edema is noted JVP = 6 cm above sternal angle and pulsus paradoxus = 22 mm. Hg Resp Chest clear throughout but shallow breaths Abd Soft but tender to palpation diffusely Neuro Alert but confused and disorientated

DDX of pulsus paradoxus Cardiac: pericardial effusion Tamponade PE Cardiogenic shock Pulmonary: Asthma COPD Tension pneumothorax Other: Anaphylaxis SVC syndrome

EKG

EDUS
 Name the general category of shock 2) Describe the pathophysiology 3)")
Case 4 1) Name the general category of shock 2) Describe the pathophysiology 3) Name the management goals 4) Define the best interventions to obtain the above goals 5) Name potential pitfalls
 Temporizing Measures")
Management of Tamponade Maximize preload Fluids to ↑ filling pressure Pressors (dialysis) Temporizing Measures Uremic pce is an indication Pericardiocentesis See remergs. com for how to (thoracotomy) If post-traumatic Definitive Measures

Case 5 PP: 26 yo Female PMHx: Healthy HPI: Involved in motorcycle accident at highway speeds + Helmet + LOC on scene and now GCS 9 STARS transfer and advised hypotensive on route unresponsive to fluids

Case 5 Generally GCS 6, collared, not responding to pain No obvious sites of external bleeding HR 57, RR 16, BP 79/40, Sats 98% 3 L NP, T 37. 8 CVS Heart sounds normal, no pedal edema, JVP normal Warm and dry skin Resp Normal Abdomen Soft and non-distended MSK Pelvis stable Neuro PEARL, no signs of depressed or basal skull fracture Reflexes absent Poor rectal tone

C-spine xray

Case 5 What is the difference between spinal shock and neurogenic shock?

Spinal Shock Concussive injury to the spinal cord Causes total neurological dysfunction distal to the site of injury Usually lasts <24 hrs May persist for several days The end of spinal shock is heralded by the return of…. . Bulbocavernousus reflex

Neurogenic Shock Disruption of sympathetic autonomic ganglia resulting in loss of vasomotor tone and lack of reflex tachycardia Results in hypotension (low SVR) Bradycardia: can be absolute or relative Due to unopposed vagal tone to heart Usually only occurs is lesion is at/above T 4
 Neurogenic Shock Adrenal insufficiency")
DDx for hypotension & bradycardia Medications (Ca. CB, BB, digoxin) Neurogenic Shock Adrenal insufficiency ++ vagal tone (yng, intra-abdominal issue)
 Name the general category of shock 2) Describe the pathophysiology 3)")
Case 5 1) Name the general category of shock 2) Describe the pathophysiology 3) Name the management goals 4) Define the best interventions to obtain the above goals 5) Name potential pitfalls

Management of neurogenic shock Fluids – they have relative hypovolemia Atropine 0. 5 mg – 1. 0 mg iv Can try to help with their pressure transiently Have ready for intubation as they may brady down 2 ndary to the vagal response Pressors Phenylephrine: 100 mcg aliquots is a good temporizer Ephedrine is an alternative

Case 6 53 yo M 1400 golfing and severe central CP radiating to R shoulder and SOB Within minutes was unresponsive and EMS called Nitro given and BP ↓↓ Palpable pressure on route

Case 6 Generally Appears very unwell, pale diaphoretic and cool periphery. Minimally responsive HR 108, BP 88/65, Sats 84% non-rebreather, RR 30 CVS Tachy with no obvious murmur Cool peripheries and thready pulse Resp Diffuse crackles throughout Pink froth at the mouth Significant respiratory distress

EKG
 Name the general category of shock 2) Describe the pathophysiology 3)")
Case 6 1) Name the general category of shock 2) Describe the pathophysiology 3) Name the management goals 4) Define the best interventions to obtain the above goals 5) Name potential pitfall

Shock Post-MI DDx Myocardium: pump failure, VSD, FWR, RV infarct Valvular: acute MR Rhythm: brady/tachycardia Other (later): PE, pericardial effusion, stroke, bleed (from a/c)

Cardiogenic shock approach AMI +shock? RV infarct? YES Volume resuscitate NO Response adequate YES NO Revascularize NO Pulmonary congestion present? YES Pressor Response adequate YES NO IABP and PTCA Thanks Phil

How does a IABP work?

Cardiogenic Shock: Approach Stabilize the ABCs Identify etiology of cardiogenic shock Small fluid bolus (250 cc) Don’t be shy on fluids if RV infarct Ionotropic/vasopressor support Manage infarct (avoid ßß & nitrates) Cath vs lytics

MI + Cardiogenic shock: How to manage the MI? Options Thrombolysis Get BP up with ionotropes then thrombolyse Stabilize with IABP then thrombolyse Early Revascularization (PTCA or CABG) What does the literature tell us?

MI + Cardiogenic shock: How to manage the MI? Thrombolysis in cardiogenic shock GISSI (N=280) streptokinase medical mx 30 day MR 70. 1% 69. 6% NO trial has shown reduction mortality with cardiogenic shock with thrombolysis Thanks Rob
")
SHOCK trial RCT of AMI + cardiogenic shock 152 early revascularization (PTCA or CABG) or 150 initial medical mx only (lysis initially, some had PTCA/CABG after 52 hrs) End Point early revasc. Med Mx stats 30 d MR 46. 7% 56% p=. 11 6 mth MR 50. 3% 63. 1% p=. 027

Cardiogenic Shock: the SHOCK trial Hochman JS. One year survival following early revascularization for cardiogenic shock. JAMA 2001. End Point early revasc. Med Mx 1 yr survival 46. 7% 33. 6% stats p=. 03

MI + Cardiogenic shock: How to manage the MI? Conclusions ……. Patients with AMI complicated by cardiogenic shock, especially those < 75 yo, should undergo emergent revascularization (PTCA or CABG)

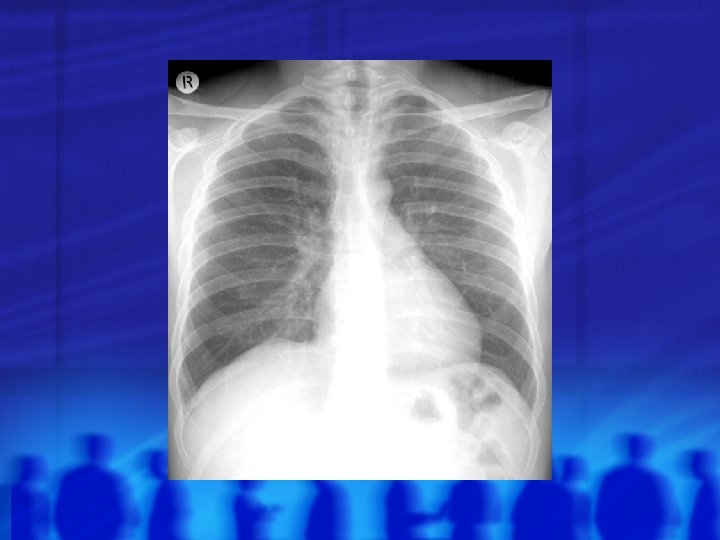
Bonus Case 78 F. Presents with SOB, hypoxia + hypotension PMHX: CAD, CHF VS: HR 110 BP 80/50, RR 28, sats 88%RA JVP up, lungs are clear, no peripheral edema – poorly perfused You order a portable CXR

N CXR

What do you think? What do you want to do?

Which can help you make the Dx? Empiric heparin STAT ECHO while investigating CT (if no CI) – but this patient is not stable enough for CT

As the p. CXR is being done the patient finally stops pestering you with questions about what you think is going on. You’re enjoying the silence until you see the monitor…

What do you want to do know?

Jerjes-Sanchez C. et al. Streptokinase and Heparin versus Heparin Alone in Massive Pulmonary Embolism: A Randomised Controlled Trial. Journal of Thrombosis and Thrombolysis. 1995. Prospective and randomised trial, N=8 all had “massive” PE and in cardiogenic shock high prob. V/Q, with abnormal RH on echo or >9 obstructed segments on V/Q 100% survival in streptokinase plus heparin group 100% mortality in heparin group Small study, lots of limitations BUT one of the few studies on this

t. PA in PE The role for t. PA in submassive PE is debatable – not a decision for us to make If the patient is in shock & they have a PE – give t. PA (likely in consultation with ICU) In the mean time intubate, heparinize + fluids PRN +/pressors If the patient has a cardiac arrest – give it t. PA dosing 1 mg/kg over 2 -5 mins if in CA Over 30 mins if perfusing If stable 100 mg over 2 H & ask yourself why you’re giving it in emerg

- Slides: 89